
Abstract
Background
Insufficient fasting prior to endoscopic procedures performed under sedation may result in potential aspiration of gastric contents. Fasting as per ASA guidelines is recommended prior to these procedures. However, the effect of chewing gum on fasting status has been a subject of debate and often leads to procedural delays.
Objective
Evaluation of the effect of chewing gum on the gastric volume and pH.
Methods
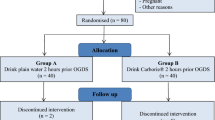
In this randomized controlled prospective observer blinded trail, ASA I–III patients aged more than 18 years scheduled for esophagogastroduodenoscopy (EGD) or a combined EGD and colonoscopy under conscious sedation were studied. Patients randomized to the chewing gum group (Group-C) were allowed to chew gum until just before the start of their procedure; the remaining patients were included into Group-NC. After sedation and endoscope insertion, stomach contents were aspirated under vision of a gastroenterologist (blinded to groups).
Results
Volume and pH of gastric contents aspirated from 67 patients (34 in Group-C and 33 in Group-NC) were analyzed. The demographic parameters of the groups were comparable. Gastric volume (median-interquartile range) was statistically higher in Group-C (13 ml (7.75–40.75) vs Group-NC 6 ml (1.00–14.00) (P < 0.001)]. The mean pH in both groups was comparable: 2.84 ± 2.11 in Group-C and 3.79 ± 2.53 in Group-NC (P = 0.141).
Conclusion
Although our results show gastric volume in patients chewing gum was statistically higher, clinical relevance of such a small difference is questionable. Thus patients who chewed gum inadvertently prior to procedure should not be denied or delayed administration of sedative and anesthetic medications.


Similar content being viewed by others


References
American Society of Anesthesiologists Committee. Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures: an updated report by the American Society of Anesthesiologists Committee on Standards and Practice Parameters. Anesthesiology. 2011;114:495–511.
Dubin SA, Jense HG, McCranie JM, Zubar V. Sugarless gum chewing before surgery does not increase gastric fluid volume or acidity. Can J Anaesth. 1994;41:603–606.
Søreide E, Holst-Larsen H, Veel T, Steen PA. The effects of chewing gum on gastric content prior to induction of general anesthesia. Anesth Analg.. 1995;80:985–989.
Schoenfelder RC, Ponnamma CM, Freyle D, Wang S-M, Kain ZN. Residual gastric fluid volume and chewing gum before surgery. Anesth Analg. 2006;102:415–417.
Taylor WJ, Champion MC, Barry AW, Hurtig JB. Measuring gastric contents during general anaesthesia: evaluation of blind gastric aspiration. Can J Anaesth. 1989;36:51–54.
Goudra B, Singh P, Sinha A. Outpatient endoscopic retrograde cholangiopancreatography: safety and efficacy of anesthetic management with a natural airway in 653 consecutive procedures. Saudi J Anaesth. 2013;7:259.
Goudra BG, Singh PM, Manjunath A, Reihmer J. Sedation spectrum in patients undergoing advanced gastrointestinal (GI) endoscopic procedures with propofol. Presented at the annual meeting of international society of anesthetic pharmacology, San Fransisco October 11th 2013.
James CF, Modell JH, Gibbs CP, Kuck EJ, Ruiz BC. Pulmonary aspiration-effects of volume and pH in the rat. Anesth Analg. 1984;63:665–668.
Heintze U, Birkhed D, Björn H. Secretion rate and buffer effect of resting and stimulated whole saliva as a function of age and sex. Swed Dent J. 1983;7:227–238.
Jensen JL, Karatsaidis A, Brodin P. Salivary secretion: stimulatory effects of chewing-gum versus paraffin tablets. Eur J Oral Sci. 1998;106:892–896.
Husslein H, Franz M, Gutschi M, Worda C, Polterauer S, Leipold H. Postoperative gum chewing after gynecologic laparoscopic surgery: a randomized controlled trial. Obstet Gynecol. 2013;122:85–90.
Leier H. Does gum chewing help prevent impaired gastric motility in the postoperative period? J Am Acad Nurse Pract. 2007;19:133–136.
Hocevar BJ, Robinson B, Gray M. Does chewing gum shorten the duration of postoperative ileus in patients undergoing abdominal surgery and creation of a stoma? J Wound Ostomy Cont Nurs. 2010;37:140–146.
Vásquez W, Hernández AV, Garcia-Sabrido JL. Is gum chewing useful for ileus after elective colorectal surgery? A systematic review and meta-analysis of randomized clinical trials. J Gastrointest Surg. 2009;13:649–656.
Parnaby CN, MacDonald AJ, Jenkins JT. Sham feed or sham? A meta-analysis of randomized clinical trials assessing the effect of gum chewing on gut function after elective colorectal surgery. Int J Colorectal Dis. 2009;24:585–592.
Zaghiyan K, Felder S, Ovsepyan G, et al. A prospective randomized controlled trial of sugared chewing gum on gastrointestinal recovery after major colorectal surgery in patients managed with early enteral feeding. Dis Colon Rectum. 2013;56:328–335.
Poulton TJ. Gum chewing during pre-anesthetic fasting. Paediatr Anaesth. 2012;22:288–296.
Acknowledgments
We wish to acknowledge the help of Dr Lakshmi Penugonda MD, Research Scholar, Department of Anesthesiology and Critical Care Medicine, Hospital of the University of Pennsylvania, Philadelphia who is currently an Anesthesiology Resident, Department of Anesthesiology and critical care medicine, Drexel University, Philadelphia, USA
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Goudra, B.G., Singh, P.M., Carlin, A. et al. Effect of Gum Chewing on the Volume and pH of Gastric Contents: A Prospective Randomized Study. Dig Dis Sci 60, 979–983 (2015). https://doi.org/10.1007/s10620-014-3404-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-014-3404-z