
Abstract
Purpose
Emotion regulation is a complex process that often involves the presence of others, also known as interpersonal emotion regulation (IER). However, little is known about how psychotic symptoms relate to IER. We investigated whether young adults with elevated psychosis proneness engage in IER less frequently and find it less helpful than those with low psychosis proneness.
Methods
Psychosis-prone young adults with attenuated negative (PP-NES, n = 37) and positive symptoms (PP-POS, n = 20) and a low psychosis-prone control group (CG, n = 52) were recruited based on a priori defined cut-offs for the Community Assessment of Psychic Experiences. Participants provided daily diaries over one week, reporting negative symptoms, paranoia, positive and negative affect, and the frequency and efficacy of IER strategies to upregulate positive and downregulate negative emotions.
Results
Multilevel models showed that PP-NES reported using IER less frequently and found it less effective compared to CG. PP-POS reported turning to others for advice in distressing situations more than the CG. These group differences were related to aberrant affect levels in PP-NES. Across groups, participants used IER less on days on which they reported more negative symptoms and used it more on days on which they reported more paranoia.
Conclusions
These findings suggest symptom-specific aberrations in everyday IER in psychosis-prone young adults. Moreover, from day to day, young adults (psychosis-prone or not) appear to adjust their use of IER depending on current social motivation and distress levels. Future research should investigate whether these aberrations are dysfunctional regarding social inclusion and symptom trajectories.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Poor social functioning has long since been identified as an early precursor of psychotic disorders (Häfner et al., 1995) and is an important predictor for the transition to psychosis from an at-risk state (Addington et al., 2019). However, the mechanism by which poor social functioning contributes to the transition is unclear. In light of high levels of negative affect, social isolation, and loneliness in at-risk individuals (e.g., Cohen et al., 2015; Gayer-Anderson & Morgan, 2013; Yee et al., 2019), a potentially relevant candidate mechanism is impaired interpersonal emotion regulation (IER), i.e., the regulation of emotions through social relationships. The present study sought to establish the degree to which people at risk of psychosis engage in IER and perceive IER as helpful. This can serve as a basis for investigating IER as a mechanism for the transition to psychosis.
Interpersonal Emotion Regulation
IER is defined as a goal-directed process of using interpersonal contact to regulate the intensity, frequency, and/or duration of positive and negative emotions (Zaki & Williams, 2013). IER involves seeking out others to influence one’s own emotions (i.e., intrinsic IER; Zaki & Williams, 2013) and attempts to regulate other people’s emotions (i.e., extrinsic IER). Thus, contrary to related constructs such as attachment, social support, or emotional contagion, IER involves specific self-focused or other-focused emotion modification goals (Williams et al., 2018; Zaki & Williams, 2013). To achieve these goals, IER uses social means and, therefore, depends on the availability of social contacts and specific interaction dynamics (Petrova & Gross, 2023). In the case of intrinsic IER, these dynamics come in varying levels of feedback from the regulating others, ranging from response-independent processes that require the mere presence of others to response-dependent processes aimed at receiving supportive behaviors or validation from one’s interaction partner (Williams et al., 2018). In contrast, intrapersonal emotion regulation (ER) entails strategies that individuals use on their own to manage their emotions (Lincoln et al., 2022; Petrova & Gross, 2023).
Based on the described IER framework, Hofmann et al. (2016) developed one of the first methods for assessing intrinsic IER, the Interpersonal Emotion Regulation Questionnaire (IERQ). In a series of four studies, the authors demonstrated that the IERQ assesses four distinct intrinsic IER strategies. The first strategy (enhancement of positive affect) targets upregulating positive emotions and includes seeking the presence of others when in a positive affective state (e.g., for sharing the experience with others). The remaining three strategies are aimed at downregulating negative emotions and entail asking others about their opinion (perspective taking), imitating their way of dealing with emotional events (social modeling), or seeking their compassion (soothing). This set of strategies has been validated across various languages and cultures (Ding et al., 2021; Koç et al., 2019; Pruessner et al., 2020).
The relevance of IER strategies in everyday life has been highlighted by recent research revealing that more than two-thirds of daily ER episodes occur within interpersonal contexts, such as among friends, colleagues, family members, or romantic partners (Paul et al., 2023).
IER and Psychopathology
Importantly, frequently using IER to regulate one’s emotions has been linked with various mental health outcomes (e.g., Chan & Rawana, 2021; Dixon-Gordon et al., 2018; Hofmann, 2014; Marroquín, 2011). Most of the available studies indicate that higher use of IER to enhance one’s positive emotions has beneficial mental health outcomes. It is related to lower anxiety, depression, stress, and negative affect (Chan & Rawana, 2021; Koç et al., 2019; Pruessner et al., 2020) and to higher well-being, positive affect, and relationship satisfaction (Chan & Rawana, 2021; Mueller et al., 2024; Pruessner et al., 2020).
In contrast, using IER strategies to decrease negative emotions has revealed less consistent links with psychological outcome measures. Higher reliance on others to regulate negative emotions has been proposed to indicate that individuals are less effective in using their own personal regulatory strategies (Hofmann et al., 2016). In line with this assumption, previous studies found that using IER strategies to regulate negative emotions, including soothing, social modeling, and perspective taking, is linked to higher levels of anxiety, depression, and substance abuse (Hofmann et al., 2016) and lower well-being (Chan & Rawana, 2021). However, other studies suggest that employing perspective taking as an IER strategy in the context of negative emotions is linked with lower levels of psychological distress (Akkuş & Peker, 2022; Altan-Atalay & Saritas-Atalar, 2022).
IER and Psychotic Symptoms
Research on how IER relates to psychotic symptoms has been limited. Aspects of IER in psychotic disorders have been analyzed in only a few studies, primarily using ecological momentary assessment (EMA) methodologies (Ludwig et al., 2020; Nittel et al., 2018; Visser et al., 2018). These studies found that using the broadly defined IER strategy of social sharing (i.e., talking with someone about an emotional event) more frequently was related to higher state levels of paranoia (i.e., a strong suspicion that others intend harm to oneself) and negative emotions at any given point in time (Nittel et al., 2018). However, talking with someone about emotional events did not predict changes in paranoia over time (Ludwig et al., 2020; Nittel et al., 2018). This putatively increased use of IER strategies in paranoid states aligns with the generally heightened use of ER strategies that has been noted in psychotic disorders (Lincoln et al., 2022; Visser et al., 2018). The tendency may reflect a greater need for regulation due to the elevated negative affect associated with distressing symptoms such as paranoia (e.g., Nittel et al., 2018). However, these findings also highlight the limited efficacy of IER in alleviating paranoid symptom distress. Additional research has shown that people with elevated levels of positive schizotypal traits (i.e., attenuated trait-level positive symptoms) experience a desire to be alone when with others, mediated by anxiety (Kwapil et al., 2012). This suggests that others may not only fail to alleviate positive psychotic symptom distress but may even exacerbate it. Furthermore, people with high schizotypal traits have been found not to show as much of an increase in positive affect when socializing as those with low schizotypal traits (Minor et al., 2020).
Even less is known about how IER may relate to the negative symptoms associated with psychotic disorders (i.e., amotivation, avolition, and diminished emotional expression). There is reason to assume these symptoms could be related to diminished IER strategy use. Reduced social drive is a core part of the amotivation in psychotic disorders (Marder & Galderisi, 2017), at-risk populations (Strauss et al., 2020), and people with negative schizotypal traits (Kwapil et al., 2012, 2020). This social disinterest is presumably caused by an expectation that social contact will not be beneficial (Jeganathan & Breakspear, 2021; White et al., 2013) or even stressful (Silvia & Kwapil, 2011) and unsurprisingly leads to a diminished initiation of social contact (e.g., Pillny et al., 2020). This likely includes diminished initiation of IER. Moreover, because diminished emotional expression impedes social interactions (e.g., Riehle & Lincoln, 2017; Riehle et al., 2018), people who experience negative symptoms can be expected to perceive the efficacy of IER strategies as relatively low.
The Present Study
In sum, the limited available evidence suggests that psychotic symptoms are likely related to aberrant use and limited efficacy of IER strategies. Underuse of IER may be an important candidate mechanism to explain how social dysfunction leads to psychosis. If an individual cannot access other people as a helpful resource to deal with distressing feelings, they may resort to less functional alternatives which may perpetuate or aggravate attenuated psychotic symptoms. For example, another person might alleviate the distress caused by an initial suspicious thought by offering convincing alternative explanations of a situation (IERQ strategy perspective taking). Without such effective IER, an individual may resort to avoidance behavior that does not challenge the suspicious thought which over time could aggravate into paranoia. However, it is currently unknown whether such difficulties in IER are present in people at risk for psychosis.
It is worth noting that both positive and negative symptoms map onto a continuum from low to high severity in the general population (van Os et al., 2009). Moreover, attenuated positive and negative symptoms are an important risk marker for psychotic disorders, particularly in young adults (Howes & Murray, 2014). We therefore investigated IER strategy use in a sample of young adults (ages 18–29) with low and high psychosis proneness. More specifically, we compared a group with attenuated positive and a group with attenuated negative symptoms to young adults with low psychosis proneness. Since both the frequency and efficacy of IER strategies have been demonstrated to be also modulated by day-to-day contextual factors, such as relationship closeness or emotions to be regulated (Paul et al., 2023; Springstein et al., 2022), we used daily diaries to assess IER strategy use and positive and negative symptoms over one week. We hypothesized that young adults with attenuated negative symptoms would use fewer IER strategies and that young adults with attenuated positive symptoms would use more IER strategies in their daily lives than people with low psychosis proneness. We also hypothesized that young adults with attenuated negative and positive psychotic symptoms would rate using IER strategies in their daily lives as less helpful than people with low psychosis proneness. Furthermore, we expected daily fluctuations in symptoms to predict daily IER use and efficacy in addition to the hypothesized group-level differences.
Methods
Study Design and Procedure
This study was an online 7-day diary study conducted between October 2021 and July 2022 using the data collection software Limesurvey (Limesurvey GmbH, Germany). Its procedures were approved by the local ethics committee of the University of Hamburg (2021_394_Bach_Dalmis_Riehle_Schlussvotum).
After consenting to participate, participants provided demographic data and completed a baseline assessment. Participants who fulfilled the inclusion criteria in the baseline assessment were sent an individualized diary link every day for the seven subsequent days. Diary assessments could be completed between 5 p.m. and midnight each day. We selected a daily diary approach over a more fine-grained EMA design as previous findings suggest a relatively infrequent occurrence of IER in everyday life (Liu et al., 2021; Tran et al., 2023) and as this approach enabled us to use a comprehensive measure of IER (a diary-adapted version of the IERQ) rather than a brief assessment as is often necessary in EMA studies. Moreover, this decision was guided by the consideration that daily diaries increase the accessibility and reduce the intrusiveness of the assessment protocol compared to EMA.
Sample
The participants were young adults (age 18–29) who received course credit or partook in a lottery with a chance of winning 25€. Besides age, other inclusion criteria were sufficient German skills (to be able to understand the study material), internet and email access for the one-week participation period, answering correctly to all four attention check items in the baseline assessment, and fulfilling the inclusion criteria of one of the three study groups: psychosis-prone – negative symptoms (PP-NES), psychosis-prone – positive symptoms (PP-POS), and low psychosis proneness (control group, CG). For group allocation, we derived cut-offs for positive and negative psychotic symptom scores on the Community Assessment of Psychic Experiences (CAPE; Stefanis et al., 2002, cape42.homestead.com) a priori from a German community validation sample (Schlier et al., 2015). PP-NES had to score above the 90th percentile in negative symptoms (> 1.40) and PP-POS above the 90th percentile in positive symptoms (> 0.74). Because we were interested in symptom-specific correlates of attenuated negative and positive psychotic symptoms, PP-NES had to score below the 90th percentile in positive symptoms and PP-POS below the 90th percentile in negative symptoms. CG had to score below the median on negative and positive psychotic symptoms (< 0.90 and < 0.38, respectively). These specific cut-off scores on the high end have not been validated for their potential to indicate a psychosis risk state. However, given that they surpass the mean levels found for people with psychotic disorders (Jaya et al., 2021), they can be considered as sufficiently indicative of relevant symptom burden. Additionally, because participants in the two attenuated symptom groups were eligible when scoring up to the 90th percentile of the respective other symptom domains, both groups were expected, on average, to present with risk-carrying symptom burden (Werbeloff et al., 2015).
Participants were recruited via university and other online platforms (such as relevant Facebook groups) and with flyers sent to early psychosis detection centers throughout Germany and Austria.
Baseline Assessment
Community Assessment of Psychic Experiences
The CAPE is a 42-item questionnaire assessing subthreshold psychotic experiences in three subscales: positive symptoms (20 items, McDonald’s ω in this sample = 0.86), negative symptoms (14 items, ω = 0.90), and depression (8 items, ω = 0.90). Items (e.g., “Do you ever feel that you are not a very animated person?” [negative symptoms]) were answered on a 0 (never) to 3 (nearly always) frequency scale. We calculated mean subscale scores, with higher scores indicating higher symptom levels.
Interpersonal Emotion Regulation Questionnaire
The Interpersonal Emotion Regulation Questionnaire (IERQ; Hofmann et al., 2016; German version: Pruessner et al., 2020) assesses the habitual use of IER for upregulating positive (subscale enhancing positive affect, IERQ-EP) and downregulating negative emotions (subscales social modeling, IERQ-SM, soothing, IERQ-SO, perspective taking, IERQ-PT). We included this assessment to supplement our diary assessments with a measurement of habitual IER use. The IERQ’s 20 items (5 per subscale; e.g., “I like being around others when I’m excited to share my joy”) were answered on a 1 (not true for me at all) to 5 (extremely true for me) agreement scale. We calculated mean subscale scores for the four IERQ subscales (IERQ-EP, ω = 0.85; IERQ-SM, ω = 0.80; IERQ-SO, ω = 0.86; IERQ-PT, ω = 0.79), with higher scores indicating more habitual strategy use.
Emotion Regulation Questionnaire
To contrast habitual IER with intrapersonal ER, we used the Emotion Regulation Questionnaire (ERQ; Gross & John, 2003; German version: Abler & Kessler, 2009). The ERQ is a 10-item questionnaire that assesses the habitual use of the intrapersonal ER strategies cognitive reappraisal (6 items, ω = 0.81) and expressive suppression (4 items, ω = 0.76). Items (e.g., “I control my emotions by not expressing them”) were answered on a 1 (strongly disagree) to 7 (strongly agree) agreement scale. We calculated mean subscale scores with higher scores indicating more habitual strategy use.
Corona-Related Social Distancing
Since our data collection fell into the late stage of Corona-related social restrictions in Germany and because these could negatively impact IER use, we assessed the degree to which participants refrained from meeting other people in person due to the pandemic (Schlier et al., under review) as a control measure. The questionnaire captured participants’ pre-pandemic level of engagement in eight different social activities (e.g., meeting other people, going to a sports club) on a 4-point Likert-scale (0 = low to 3 = high) and the degree to which participants have reduced engaging in these activities because of the pandemic on a 5-point Likert scale (0 = engaging on pre-pandemic level to 4 = not engaging in this activity anymore). We calculated the product of pre-pandemic engagement and pandemic-related reduced engagement for each activity. We averaged these weighted item scores (ω = 0.69), with higher scores indicating more Corona-related social distancing.
Diary Assessments
Interpersonal Emotion Regulation
For the diary assessment of IER, we developed a diary-adapted version of the IERQ (Diary-IERQ). For this, we rephrased each of the 20 IERQ items to reflect IER use during a given day. Moreover, to assess frequency and efficacy separately in the Diary-IERQ, we cleared several original IERQ items of references to IER efficacy. For example, we rephrased the original IERQ item “Having people remind me that others are worse off helps me when I'm upset.” to “When I was upset today, I had people remind me that others are worse off.”. We assessed the frequency of IER (“To which extent does the statement describe you today?”; 0 [not at all to 4 [completely]) and the perceived efficacy of IER for each item with a frequency score > 1 (“To which extent did this make you feel better today?”; 0 [not at all] to 4 [very much]). The complete Diary-IERQ is presented in the online supplementary material.
We calculated daily mean frequency and efficacy scores for each of the four original subscales contained in the IERQ using the same item-to-subscale allocation. Multilevel internal consistencies for the frequency scores were as follows: Diary-IERQ-EP: ωwithin = 0.89, ωbetween = 0.95; Diary-IERQ-SM: ωwithin = 0.84, ωbetween = 0.74; Diary-IERQ-SO: ωwithin = 0.87, ωbetween = 0.73; Diary-IERQ-PT: ωwithin = 0.90, ωbetween = 0.65). For the efficacy scores they were: Diary-IERQ-EP: ωwithin = 0.89, ωbetween = 0.95; Diary-IERQ-SM: ωwithin = 0.84, ωbetween = 0.74; Diary-IERQ-SO: ωwithin = 0.87, ωbetween = 0.73; Diary-IERQ-PT: ωwithin = 0.90, ωbetween = 0.65).
Negative Symptoms
We adopted a negative symptoms assessment developed for an EMA study (Pillny et al., 2020) based on the Motivation and Anticipation of Pleasure – Self-Report Scale (Llerena et al., 2013). Nine items assessed behavioral engagement (“Which percentage of your time did you spend today doing the following activities?”), motivation (“How motivated were you today to do…”), and anticipation of pleasure (“Looking ahead for tomorrow, how much pleasure do you expect from…”) for three types of activities: i) spending time with family/friends/acquaintances, ii) pursuing hobbies/recreational activities, iii) engaging in self-care. All items were answered using visual analogue sliders (0 = 0%/not motivated at all/no pleasure to 100 = 100%/very motivated/very much pleasure). We calculated the daily mean score on the inverted item scores so that higher scores indicated higher daily negative symptoms (ωwithin = 0.67, ωbetween = 0.90).
Paranoia
We used the 3-item version of the Brief Paranoia Checklist (Schlier et al., 2016), a shortened and state-adapted version of the Paranoia Checklist (Freeman et al., 2005). Items (e.g., “I need to be on my guard against others”) were answered on a 1 (not at all) to 5 (very much) agreement scale. We calculated the daily mean score with higher scores indicating higher paranoia (ωwithin = 0.63, ωbetween = 0.89).
Positive and Negative Affect
We used the Positive and Negative Affect Schedule (PANAS; Watson et al., 1988) to assess daily positive and negative affect levels. The PANAS includes 20 adjectives, with ten each describing positive (e.g., interested, proud) and negative emotional states (e.g., distressed, nervous). Participants rated the extent to which they had felt this way over the day on a 1 (very slightly or not at all) to 5 (extremely) Likert scale. We calculated sum scores for positive (PA; ωwithin = 0.88, ωbetween = 0.93) and negative affect (NA; ωwithin = 0.84, ωbetween = 0.93), with higher scores indicating stronger affect.
Transparency and Openness
We report power calculations, all data exclusions, and all measures in the study. All data and analysis code needed to reproduce this report are available at https://doi.org/10.23668/psycharchives.12663 (data) and https://doi.org/10.23668/psycharchives.15228 (code). All data analyses were performed using R version 4.1.0 (Table S1 in the supplementary material details the R-packages used). The study’s design and the analyses were not pre-registered.
Data Analysis
We first excluded all cases that provided less than three diaries to ensure that day-to-day within-participant fluctuations could be assessed with adequate statistical power. We then tested for differences in baseline data between PP-NES, PP-POS, and CG using ANOVAs and pairwise t-test comparisons. To test for group differences in the Diary-IERQ, we used multilevel linear models (MLM) because diary entries (level 1) were nested within participants (level 2). We included group as a dummy-coded level-2 predictor. In those models, we also tested for the impact of daily fluctuations in symptoms on the Diary-IERQ by adding negative symptoms and paranoia as subject-wise mean-centered level-1 predictors alongside group to the MLMs (random-intercept-only models as random-slope models failed to converge due to low slope variation). The model equation was given by.
The between-subjects SD (random effect of the intercept) and the intraclass correlation coefficient (ICC) were obtained from null models. We report unstandardized (b) and standardized (β) fixed effects estimates and calculated Cohen’s d as an effect size of group differences by dividing the difference between two groups’ estimated marginal means by the between-subjects SD obtained from the null model. Thereby, d provided an effect size of the group difference on level 2 (i.e., between subjects) after partialling out the within-subject day-to-day variation. We additionally report explained variance (R2) according to the decomposition approach by Rights and Sterba (2019) in the supplementary material. All tests were performed at an α-level of p = 0.05 using Benjamini–Hochberg correction within each set of hypotheses.
We tested for group differences in the other diary variables (negative symptoms, paranoia, positive and negative affect) in multilevel models containing only the dummy-coded group factor.
Power analyses using the R package EMAtools (Kleiman, 2021) with a maximum number of 7 diary entries per subject and intraclass correlation coefficients (ICC) ranging between 0.24–0.51 (the observed values in this study) revealed that the achieved sample size was sufficiently large to detect medium-sized effects (Cohen’s d = 0.5) at the lowest level (i.e., level 1) with a power of β > 0.80 and an α-level of p < 0.05.
Results
Sample Characteristics
The baseline assessment was completed by 372 participants, of which 163 (43.8%) fulfilled the inclusion criteria for one of the three study groups, 175 (47.0%) were excluded due to providing symptom ratings above the median in at least one of the two symptom domains (i.e., positive and negative symptoms) but below the 90th percentile in both symptom domains, and 34 (9.9%) were excluded due to providing symptom ratings above the 90th percentile in both symptom domains. The diary study was completed by 127 participants, of which 109 (the final sample; nPP-NES = 37, nPP-POS = 20, nCG = 52) provided at least three diary entries (14% attrition, no group differences, χ2(2) = 1.83, p = 0.401).
The adherence rate for the diaries was high, with 14% missing completely (i.e., 107 diaries). For 22 additional diaries, state paranoia ratings were missing due to participants not completing the diary (the Brief Paranoia Checklist was the last page). Additional missings occurred for the four Diary-IERQ efficacy scales when participants had Diary-IERQ frequency values of 0 on any given frequency scale and thus were not prompted to provide an efficacy rating (9–27% of the diaries depending on the respective Diary-IERQ scale). Regarding group differences in adherence, on average, PP-NES and PP-POS provided roughly one diary entry (thus, significantly) less than CG (PP-NES: M = 5.76, SD = 1.52; PP-POS: M = 5.50, SD = 1.40; CG: M = 6.40, SD = 0.98; F(2,44.41) = 5.09, p = 0.010).
Further sample characteristics and results of the baseline assessment are presented in Table 1. As can be seen there, the three groups did not differ on any demographic variables assessed. The group differences in CAPE negative and positive psychotic symptoms reflected the group allocation procedure. Additionally, PP-NES scored significantly higher on CAPE depression than both other groups, whereas PP-POS scored higher on CAPE depression than CG. Moreover, the PP-NES group reported less habitual use of the IER strategies enhancement of positive affect and soothing than the CG. Furthermore, we found a main effect of group on the habitual use of IERQ perspective taking, but the pair-wise comparisons did not yield significant group differences. PP-NES also reported higher levels of emotional suppression in the ERQ than both other groups.
Between-person Effects: Group Differences in Daily Diary Variables
Interpersonal Emotion Regulation
Table 2 shows the results of the multilevel models testing for group differences in the Diary-IERQ (frequency and efficacy), and Figs. 1 and 2 illustrate these differences alongside the sample distributions. The full model results are reported in the supplementary material (Tables S2-S14). For the multiple tests of group differences reported in Table 2, the Benjamini–Hochberg correction suggested a corrected α-level of p ≤ 0.018.

Half-violin plots with box plots and individual participant data illustrating the group differences in the frequency of interpersonal emotion regulation in daily life as estimated via MLM. Note. Horizontal lines represent the estimated mean values of participants, with line lengths corresponding to the number of diary entries provided by each participant (shorter = fewer entries). PP-NES/-POS = Psychosis-prone – attenuated negative/positive symptoms, CG = control group. Diary-IERQ = Interpersonal Emotion Regulation Questionnaire (diary adapted version)

Half-violin plots with box plots and individual participant data illustrating the group differences in the efficacy of interpersonal emotion regulation in daily life as estimated via MLM. Note. Horizontal lines represent the estimated mean values of participants, with line lengths corresponding to the number of diary entries provided by each participant (shorter = fewer entries). PP-NES/-POS = Psychosis-prone – attenuated negative/positive symptoms, CG = control group. Diary-IERQ = Interpersonal Emotion Regulation Questionnaire (diary adapted version)
As shown in Table 2, the PP-NES group reported significantly less frequent use of the IER strategies enhancement of positive affect and social modeling than the CG with a large and moderate effect size, respectively. A moderate-to-large effect size difference between PP-NES and PP-POS suggesting that PP-NES used enhancement of positive affect less frequently did not reach significance. No group differences were found in the frequency of using soothing as an IER strategy. The PP-POS group reported asking others for a different perspective on an emotional event (perspective taking) significantly more often than the CG.
Regarding the efficacy of IER strategies, the PP-NES group reported significantly lower efficacy of the strategies enhancement of positive affect (large effect) and soothing (moderate effect) than the CG. The PP-POS group reported higher efficacy of the strategy perspective taking than both other groups (moderate to large effects).
Symptoms and Affect
As also shown in Table 2, the PP-NES group reported lower positive affect than both other groups (large effects). Both the PP-NES (large effect) and the PP-POS group (moderate effect) reported higher levels of negative affect than the CG, but this difference was only significant for the PP-NES group. Moreover, the PP-NES group reported significantly higher daily negative symptoms than both other groups (moderate-to-large effects). Both the PP-NES (moderate effect) and the PP-POS group (large effect) endorsed significantly higher daily paranoia levels than the CG.
Within-Person Effects: Daily Symptoms, Interpersonal Emotion Regulation, and Affect
The effects of within-person day-to-day fluctuations in negative symptoms and paranoia on the Diary-IERQ variables and the PANAS are shown in Table 3 (these all pertain to the models reported in Tables S3-S12 in the supplement). As can be seen there, participants across the three groups used the IER strategies enhancement of positive affect, social modeling, and soothing significantly less frequently on days on which they reported higher levels of negative symptoms. To the contrary, they used all IER strategies for downregulating negative emotions (i.e., social modeling, soothing, and perspective taking) more frequently on days on which they reported higher levels of paranoia.
Regarding within-person effects on the efficacy of IER strategies, we only found significant effects for the enhancement of positive affect, which participants reported to be less helpful on days with higher levels of negative symptoms and paranoia.
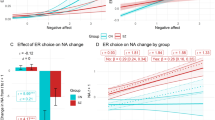
We also found that positive affect was significantly lower on days with higher levels of negative symptoms (not on days with higher levels of paranoia) and that negative affect was significantly higher on days with higher levels of negative symptoms and paranoia.
Additional Analyses
Since all items of the IERQ/Diary-IERQ assess response-focused ER strategies – thus, ER strategies that are used once an emotion is present – and since we found group differences in positive and negative affect, we were also interested in the degree to which aberrant affect levels entail an aberrant frequency of IER and whether this impacts our estimates of group differences in the frequency of using IER strategies in daily life. We, therefore, repeated our analyses for the Diary-IERQ frequency domain, controlling for the effects of positive affect (on the enhancement of positive affect) and negative affect (on each IER strategy for downregulating negative emotions). We added the respective affect scale as a person-centered predictor (i.e., day-to-day within-person fluctuations, level 1) and a person-mean predictor (i.e., person week-average, level 2) to the MLM that was described above. As is reported in Tables S15-S20 in the supplementary material, higher levels of PA were a significant predictor of a higher frequency of using the IER strategy enhancement of positive affect (both week-average and day-to-day PA: βs ≥ 0.38, ps < 0.001), with no significant group differences occurring in this model (ds ≤|0.18|, ps ≥ 0.437). Thus, the significant difference between the PP-NES group and the CG was no longer observable after controlling for PA levels. Higher levels of NA were a significant predictor of a higher frequency of using each of the three IER strategies for downregulating negative emotions (week-average NA: βs ≥ 0.23, ps ≤ 0.021; day-to-day NA: βs ≥ 0.07, ps ≤ 0.025). For the strategies social modeling and soothing, these models resulted in significant group differences such that the PP-NES group reported significantly less frequent strategy use than the CG (social modeling: b = -0.53, p < 0.001, d [95% CI] = -0.83 [-1.31, -0.35]; soothing: b = -0.55, p < 0.001, d [95% CI] = -0.82 [-1.29, -0.35]). The significant group difference between the PP-POS group and CG reported for the Diary-IERQ subscale perspective taking in Table 2 was no longer significant after controlling for NA (b = 0.26, p = 0.070, d [95% CI] = 0.51 [-0.05, 1.07]).
Next, we were interested in the degree to which the habitual use of IER and ER strategies, as assessed with the IERQ and ERQ, respectively, depressive symptoms (CAPE) and other baseline variables were associated with using IER in daily life. We calculated a series of random-intercept-only MLMs with a single level-2 predictor each to predict the Diary-IERQ variables. The results, shown in Table 4, revealed that each IERQ subscale was significantly associated with their Diary-IERQ counterparts. In contrast, most associations across subscales were either smaller in magnitude or non-significant. Also, we found this association of the IERQ with its diary version equally for the frequency and efficacy subdomains of the diary version. Regarding habitual intrapersonal ER assessed with the ERQ, emotional suppression was negatively related to all Diary-IERQ variables except perspective taking. In contrast, cognitive reappraisal was not associated with any Diary-IERQ variable. Higher levels of depression were also not related to any Diary-IERQ variable. Interestingly, more Corona-related social distancing was associated with a higher frequency and efficacy of Diary-IERQ perspective taking.
We also conducted a sensitivity analysis with an imputed data set using the multilevel multiple imputation approach according to Grund et al. (2016). This sensitivity analysis is presented in detail in the online supplementary material (text and Tables S21-S36) and confirmed the findings as reported above.
Finally, to test the degree to which our findings were attributable to time spent with others, we reanalyzed the data excluding the item assessing the amount of time spent with others (i.e., family/friends/acquaintances) from our diary negative symptom score. In these models, we used this alternative diary negative symptom score as a predictor and the time spent with others item as an additional covariate. We found that having spent more time with others was significantly related to all Diary-IERQ frequency variables (all ps ≤ 0.008), except perspective taking (ps ≥ 0.354). Crucially, all additional effects for diary negative symptoms and paranoia remained stable in these models as reported above, including in the models controlling for affect.
Discussion
In this study, we investigated the use of IER in the daily lives of young adults with varying degrees of psychosis proneness. We found IER to be altered with specific effects for positive and negative symptoms. The results for positive symptoms suggest that young adults turn to other people more when experiencing higher levels of paranoia. Negative symptoms, in contrast, appear to be associated with a decreased use and perceived efficacy of IER, although some of these effects seem to be contingent upon altered affective experience in this group. Our findings add to those of two other recent studies on IER in people with varying levels of schizotypy – both of which were published while the data collection of our study was ongoing (Gunn & Donahue, 2022; Schwartz et al., 2022). These studies are particularly relevant because schizotypy denotes traits that include attenuated positive and negative symptoms, as defined in our study (Modenato & Draganski, 2015).
IER Frequency and Attenuated Negative Symptoms
Our finding of a lower frequency of using IER strategies to enhance or sustain positive emotions in negative symptoms aligns with these two previous studies (Gunn & Donahue, 2022; Schwartz et al., 2022). The asociality (i.e., low social motivation and social withdrawal) that is an essential aspect of negative symptoms in daily life (e.g., Kwapil et al., 2012; Pillny et al., 2020) appears to be an obvious explanation for these findings. Young adults with negative symptoms would not engage in as many social interactions due to a lack of social interest and, therefore, report a lower frequency of using IER. Another explanation, however, may be the diminished experience of positive affect (i.e., anhedonia) in this group that we found in line with previous research (e.g., Kwapil et al., 2012; Schwartz et al., 2022). Because the diminished positive affect explained away the group difference in IER strategy use between the attenuated negative symptoms and the other two groups, we cannot rule out that the reduced use of IER strategies for positive emotions in negative symptoms is primarily contingent on a diminished regulatory need. However, our design did not allow for an analysis of the causal direction of the associations of affect and IER strategy use, leaving this an interesting avenue for future research.
Concerning the frequency of using IER strategies for negative emotions, our results indicated that young adults who experience attenuated negative symptoms appear to have someone guide them on how to deal with distressing emotions less frequently (social modeling) and seem to less frequently seek out others for comfort and sympathy (soothing). An important specification of these effects was that they were the strongest when we controlled for the elevated negative affect levels reported by this group. Under the assumption that negative affect precedes IER strategy use, this could be interpreted as a mismatch between the regulatory need for negative affect (high) and frequency of IER strategy use (moderate) in negative symptoms. Such a mismatch has recently been found for intrapersonal ER strategies in a clinical psychosis sample (Raugh & Strauss, 2022). Gunn and Donahue (2022) found an association in the habitual use of the two IER strategies, social modeling and soothing, with negative schizotypal traits when other schizotypal traits were accounted for in the analysis, but did not find associations when these other schizotypal traits were not accounted for. These findings could be consistent with the mismatch hypothesis when one assumes that controlling other schizotypal traits may be a proxy for controlling for elevated negative affect levels. However, replication of these findings focusing on this question is warranted – preferably in an ecological momentary assessment study where the causal direction of this relationship can be tested (i.e., people with attenuated negative symptoms respond to elevations of negative affect less likely with IER).
From a theoretical point of view, the reluctance of people with negative symptoms to engage in IER for distressing emotions could be explained by low expectations that others will react empathic or sympathetic to their displays of vulnerability (Jeganathan & Breakspear, 2021; Riehle, (in press); White et al., 2013). Further fueling this reluctance could be self-ascribed difficulties in describing emotions to others that have been found at an equal level both in schizophrenia and clinical high-risk samples (e.g., Kimhy et al., 2016). Taking IER strategy use into consideration, therefore, sheds new light on several previous findings, replicated by our study, showing that using emotional suppression more is associated with negative symptoms (Kimhy et al., 2016; Larson et al., 2020; Osborne et al., 2017; van der Velde et al., 2015; van Rijn et al., 2011). Negative experiences with using IER and/or disclosing feelings to others and self-ascribed difficulties in verbalizing emotional states each could form a vicious cycle with emotional suppression. Inquiring these processes further may open up an interesting avenue to better understand etiological paths to diminished emotional expression as a negative psychotic symptom.
It is also worth noting that the associations between negative symptoms and reduced IER strategy use to alleviate negative emotions are not necessarily indicative of impaired ER. For example, there have been mixed findings as to whether increased use of emotional suppression is related to lower social functioning levels in schizophrenia and high-risk samples (cf., Chapman et al., 2020; Kimhy et al., 2016; Lincoln et al., 2022). In addition, the results of our analyses of day-to-day changes in symptoms and IER strategy use (within-person effects) suggested that irrespective of the participant group, everyone was less inclined to use IER strategies on days where they experienced higher negative symptoms (i.e., motivational impairments). It could be considered particularly functional not to rely on IER on days with low motivation to seek out contact with others. Here, flexibility in strategy selection may be a key issue (Aldao et al., 2015; Bonanno & Burton, 2013; Lincoln et al., 2022). Interestingly, one study (Bortolon et al., 2022) found that attenuated negative symptoms were related to difficulties in enhancing emotional expression to provide extrinsic IER (i.e., accommodating the feelings of others). The ER flexibility framework has yet to be applied to the relationship between psychotic symptoms and the intrinsic IER strategies considered in our study.
An unresolved question is why negative symptoms specifically seem to affect IER strategies such as social modeling and soothing, but not perspective taking. Given that perspective taking was reported with the lowest frequency of all IER strategies, we cannot rule out that a floor effect may have prevented relevant group differences or symptom associations from showing up. However, since Gunn and Donahue (2022) even identified a positive association between negative schizotypy and perspective taking, future research should examine these contrasting effects.
IER Efficacy and Attenuated Negative Symptoms
The attenuated negative symptoms group also reported a lower perceived efficacy of using IER strategies for positive and negative emotions. An important implication of this finding is that the low perceived efficacy likely fuels a vicious cycle of negatively appraised social interactions, social disinterest, and withdrawal (Jaya et al., 2022; Jeganathan & Breakspear, 2021; Riehle, in press; White et al., 2013). Additionally, negative symptoms, particularly diminished expression, appear to be specifically related to more negative interpersonal experiences (Jeganathan & Breakspear, 2021; Riehle, in press; Riehle et al., 2018), and this also at subclinical symptom levels (Riehle & Lincoln, 2017). Accordingly, difficulties with expressing emotions could lead to misunderstandings or limited empathic concern in others, who then may not provide helpful responses. This could explain why attempts at using IER are rated as less helpful by those with negative symptoms. Interestingly, the study by Schwartz et al. (2022) suggested intact efficacy of IER for positive emotions in negative schizotypal traits. Of note, whereas Schwartz and colleagues (2022) assessed time-lagged changes in affect from one assessment to the next in their EMA (prospective indirect change measure), we asked for the perceived efficacy of the specific IER strategies that the participants had used throughout the day (retrospective direct change measure). It could, therefore, be that Schwartz and colleagues (2022) detected more short-term, momentary changes in affect that are not impaired by negative symptoms. The diminished efficacy of using IER strategies reported by the attenuated negative symptoms group could then be interpreted as negatively biased by negative beliefs about the pleasantness of social interactions. Such beliefs are common in negative symptoms (Pillny et al., 2018; Yang et al., 2018) and an important aspect of the cognitive conceptualization of negative symptoms (Beck et al., 2011). A more fine-grained EMA approach would be helpful to address these mixed findings further, as would be studies that assess subjective (e.g., perceived IER efficacy, affect changes) and objective (e.g., psychophysiological changes) markers of using IER.
IER Frequency and Efficacy in Attenuated Positive Symptoms
Our results concerning the attenuated positive symptoms group showed that this group turned to others for advice in distressing situations (perspective taking) more frequently than both other groups and also reported higher efficacy of this strategy. We found group differences for the habitual IERQ and the Diary-IERQ. Furthermore, irrespective of group, within-person effects showed that all IER strategies for alleviating negative emotions (i.e., soothing, social modeling, perspective taking) were used more frequently on days on which people felt more paranoid. In line with this, Gunn and Donahue (2022) found significant positive associations between positive schizotypal traits and those same three IER strategies assessed on a habitual level. Our results extend these findings to the everyday context of our diary study. This suggests that people in paranoid states frequently turn to others to deal with distressing emotions. Due to the strong association between negative affect and paranoia (e.g., Kramer et al., 2013; Krkovic et al., 2019; Kwapil et al., 2012, 2020), paranoia may come along with an additional need to regulate negative affect that people meet with increased IER just as they meet it with increased intrapersonal ER (Lincoln et al., 2022; Visser et al., 2018). Indeed, when controlling for negative affect levels, those associations largely disappeared or were notably reduced (but see Gunn & Donahue, 2022, where these effects remained stable after controlling for other schizotypal traits). Whereas it may seem counterintuitive that elevated levels of suspiciousness and paranoia would lead to increased IER, it is important to consider that the IERQ does not assess whether someone engages in IER with many different people, just a few, or even with only a single trusted person. Previous studies have suggested that most IER takes place with close others (Geiger et al., 2023; Liu et al., 2021), and it is a viable hypothesis to test whether the circle of people that are turned to for IER is smaller in people with positive psychotic symptoms.
We also found that daily paranoia levels were associated with a lower perceived efficacy of using IER to enhance positive affect. As for negative symptoms, this may be due to specific biases in the retrospective report potentially driven by paranoid rumination. However, we cannot disentangle whether this explains our findings, whether attempts at using IER for positive emotions when in a more paranoid state fail more readily, or whether experiencing failed attempts at using IER for positive emotions increases paranoia levels. Nevertheless, our study identifies these questions as important avenues for future research.
Implications for IER as a Transdiagnostic Factor
The contrasting use of IER strategies in attenuated negative and positive psychotic symptoms highlights the importance of considering interpersonal regulation processes as specific markers not only of different subtypes of psychosis proneness but also of different aspects of psychopathology per se. A growing body of research suggests that IER is affected differently in different forms of psychopathology (Barthel et al., 2018; Dixon-Gordon et al., 2018; Hofmann, 2014; Hofmann & Doan, 2018). For instance, depression has been found to be associated with decreased IER, whereas anxiety shows an opposite pattern with increased reassurance and support-seeking (Beesdo-Baum et al., 2012; Dixon-Gordon et al., 2018; Rector et al., 2019). One may suspect that the discrepancy between these findings and other research suggesting that depression and anxiety are both related to increased use of IER (e.g., Hofmann et al., 2016) may be attributable to variations in the definitions and measurements of IER constructs. In this study, we derived the Diary-IERQ from the IERQ (Hofmann et al., 2016). Nevertheless, we did not find significant effects of depressive symptoms on IER. Our results suggest that amotivational (negative psychotic) but not depressive symptoms are related to decreased use of IER. Future research should aim to disentangle the differential effects of IER use associated with these two symptom domains. For heightened levels of anxiety (e.g., worrying, paranoid thoughts), the data seem to consistently suggest increased use of IER aimed at alleviating negative affective states (e.g., reassurance seeking, seeking advice).
The effect of increased IER use in more anxious participants may also explain why corona-related social distancing was related to more frequent and effective use of perspective taking to downregulate negative emotions. Throughout our data collection (October 2021 – July 2022), meeting friends was largely unrestricted in Germany (Steinmetz et al., 2022). It is possible that at this late stage of the pandemic, more anxious individuals adhered to the remaining social restrictions more (e.g., Matthews et al., 2021). Following these restrictions may have increased contact with close others (e.g., partner, family) compared to non-close others (e.g., colleagues, acquaintances) and thus created additional opportunities for IER (Paul et al., 2023).
How frequently and effectively IER is used is likely a relevant transdiagnostic risk and maintenance factor. Further understanding the role of IER in psychopathology, thus, will likely help develop transdiagnostically effective preventive and therapeutic strategies. Regarding measurement, our diary adaptation of the IERQ showed significant associations with the habitual IERQ. Interindividual differences in habitual IERQ strategies explained 10–46% of the between-subject variation in the Diary-IERQ frequency scores of the same strategy, constituting moderate to large effects. Nevertheless, 53–67% of the total variation in the Diary-IERQ scores was due to within-person (i.e., day-to-day) variation. This suggests that the frequency of IER use is not an entirely stable construct, even though it shows a certain level of intraindividual stability. In our study, such residual within-person variance needed to be expected given that a one-week ecological momentary assessment can include non-representative weeks for some individuals. Moreover, a considerable portion of this within-person variation was explained by day-to-day fluctuations in other measured constructs (i.e., negative symptoms and paranoia), suggesting systematic in addition to random variation. Furthermore, we cannot rule out that rephrasing some of the IERQ items to fit the diary adaptation and to separate frequency from efficacy of strategy use also added to measurement inequivalence.
Limitations
A limitation of our study design is that it necessitated time-locked analyses, which prevented us from analyzing the causal direction of our effects and introduced potential bias due to retrospective assessments. More fine-grained EMA approaches and experimental investigations are needed to answer some of the questions raised by our study. Another limitation is that our assessment of time spent with others (part of the diary negative symptom assessment) did not include an evaluation of the types of motivation for spending time with others. We cannot disentangle whether our findings, particularly for PP-NES and negative symptoms, suggest that spending little time with others resulted in fewer opportunities for IER or whether not being motivated to use IER resulted in less time spent with others. Additionally, whereas restricting the sample to young adults elevates our findings’ relevance for the understanding of psychosis-risk states, our recruitment strategy attracted a sample for which the generalizability towards non-Western cultures, other age groups, and the lower socio-economic status portion of the population is limited (Henrich et al., 2010). The validity of our approach of preselecting groups of participants with high/low psychotic symptoms is limited as this approach prevented us from investigating the phenomena in question for the entire continuum of psychotic experiences. Moreover, whereas our extreme group approach helped to identify symptom-specific associations, this came at the cost of excluding participants who scored high in both symptom domains, which limits the generalizability of the findings to those with a more severe symptom profile. Additionally, our approach was limited based on our use of a self-report symptom measure (CAPE). Although this approach aligns with the other studies in the field (Gunn & Donahue, 2022; Schwartz et al., 2022), future studies may benefit from interview-based symptom assessments. These are the gold standard, particularly for negative symptoms, both in people at risk for psychosis (Strauss et al., 2020) and in people with schizophrenia (Kirkpatrick et al., 2010; Kring et al., 2013). We also did not assess disorganized symptoms, which could have unique associations with some aspects of IER (Gunn & Donahue, 2022; Kwapil et al., 2020). Another limitation is that we followed an IER definition that assumes an explicit emotion regulation goal (Petrova & Gross, 2023; Zaki & Williams, 2013). This definition also underlies the IERQ (Hofmann et al., 2016) and helps to distinguish IER from related concepts such as attachment, social support, or emotional contagion (Williams et al., 2018; Zaki & Williams, 2013). However, it falls short of potential implicit regulation goals or situations where a social context passively results in emotion regulation but was not actively sought or even intended. Moreover, it would be interesting to explore additional IER processes not encompassed in the current study, such as interpersonal regulatory difficulties (Dixon-Gordon et al., 2018; Williams et al., 2018) or extrinsic interpersonal strategy use (Niven et al., 2011). Finally, it should be considered that the sample size of the psychosis-prone positive symptoms group was relatively small, which may have limited our ability to detect group differences.
Conclusion
We found that young adults with attenuated negative symptoms make less use of IER and find it less helpful than young adults with attenuated positive symptoms and young adults with low psychosis proneness. This highlights that negative symptoms are closely associated with social dysfunction in psychosis risk states and suggests that IER is not as much of a resource for these people at a time when the transition to a psychotic disorder is most likely. The now three available studies on IER in psychosis-risk states (this study; Gunn & Donahue, 2022; Schwartz et al., 2022) suggest that some aberrations in IER are associated with psychosis risk. These initial results justify a more thorough inquiry into whether these aberrations have a mechanistic relationship to the transition to psychosis and poorer clinical outcomes over time. This inquiry also needs to clarify the degree to which aberrations, if dysfunctional, occur in IER frequency or efficacy. This knowledge could advance early intervention strategies by adding or optimizing IER modules, for example, for social skills training, systemic approaches, or family-based interventions.
References
Abler, B., & Kessler, H. (2009). Emotion regulation questionnaire—Eine deutschsprachige Fassung des ERQ von gross und john. Diagnostica, 55(3), 144–152. https://doi.org/10.1026/0012-1924.55.3.144
Addington, J., Farris, M., Stowkowy, J., Santesteban-Echarri, O., Metzak, P., & Kalathil, M. S. (2019). Predictors of transition to psychosis in individuals at clinical high risk. Current Psychiatry Reports, 21(6), 39. https://doi.org/10.1007/s11920-019-1027-y
Akkuş, K., & Peker, M. (2022). Exploring the relationship between interpersonal emotion regulation and social anxiety symptoms: the mediating role of negative mood regulation expectancies. Cognitive Therapy and Research, 46(2), 287–301. https://doi.org/10.1007/s10608-021-10262-0
Aldao, A., Sheppes, G., & Gross, J. J. (2015). Emotion regulation flexibility. Cognitive Therapy and Research, 39(3), 263–278. https://doi.org/10.1007/s10608-014-9662-4
Altan-Atalay, A., & Saritas-Atalar, D. (2022). Interpersonal emotion regulation strategies: how do they interact with negative mood regulation expectancies in explaining anxiety and depression? Current Psychology, 41(1), 379–385. https://doi.org/10.1007/s12144-019-00586-2
Barthel, A. L., Hay, A., Doan, S. N., & Hofmann, S. G. (2018). Interpersonal Emotion Regulation: A Review of Social and Developmental Components. Behaviour Change, 35(4), 203–216. https://doi.org/10.1017/bec.2018.19
Beck, A. T., Rector, N. A., Stolar, N., & Grant, P. (2011). A Cognitive Conceptualization of Negative Symptoms. In A. T. Beck, N. A. Rector, N. Stolar, & P. Grant (Eds.), Schizophrenia. Cognitive Theory, Research, and Therapy (pp. 142–158). Guilford Press.
Beesdo-Baum, K., Jenjahn, E., Höfler, M., Lueken, U., Becker, E. S., & Hoyer, J. (2012). Avoidance, safety behavior, and reassurance seeking in generalized anxiety disorder. Depression and Anxiety, 29(11), 948–957. https://doi.org/10.1002/da.21955
Bonanno, G. A., & Burton, C. L. (2013). Regulatory Flexibility. Perspectives on Psychological Science, 8(6), 591–612. https://doi.org/10.1177/1745691613504116
Bortolon, C., Chen, S., & Bonanno, G. A. (2022). Components of emotion regulation flexibility and psychosis: The association between psychosis-proneness and context sensitivity. British Journal of Clinical Psychology. https://doi.org/10.1111/bjc.12395
Chan, S., & Rawana, J. S. (2021). Examining the associations between interpersonal emotion regulation and psychosocial adjustment in emerging adulthood. Cognitive Therapy and Research. https://doi.org/10.1007/s10608-020-10185-2
Chapman, H. C., Visser, K. F., Mittal, V. A., Gibb, B. E., Coles, M. E., & Strauss, G. P. (2020). Emotion regulation across the psychosis continuum. Development and Psychopathology, 32(1), 219–227. https://doi.org/10.1017/S0954579418001682
Cohen, A. S., Mohr, C., Ettinger, U., Chan, R. C. K., & Park, S. (2015). Schizotypy as An Organizing Framework for Social and Affective Sciences. Schizophrenia Bulletin, 41(suppl 2), S427–S435. https://doi.org/10.1093/schbul/sbu195
Ding, R., He, W., Liu, J., Liu, T., Zhang, D., & Ni, S. (2021). Interpersonal Regulation Questionnaire (IRQ): Psychometric properties and gender differences in Chinese young adolescents. Psychological Assessment, 33(4), e13–e28. https://doi.org/10.1037/pas0000997
Dixon-Gordon, K. L., Haliczer, L. A., Conkey, L. C., & Whalen, D. J. (2018). Difficulties in Interpersonal Emotion Regulation: Initial Development and Validation of a Self-Report Measure. Journal of Psychopathology and Behavioral Assessment, 40(3), 528–549. https://doi.org/10.1007/s10862-018-9647-9
Freeman, D., Garety, P. A., Bebbington, P. E., Smith, B., Rollinson, R., Fowler, D., Kuipers, E., Ray, K., & Dunn, G. (2005). Psychological investigation of the structure of paranoia in a non-clinical population. British Journal of Psychiatry, 186(5), 427-435. https://doi.org/10.1192/bjp.186.5.427
Gayer-Anderson, C., & Morgan, C. (2013). Social networks, support and early psychosis: A systematic review. Epidemiology and Psychiatric Sciences, 22(2), 131–146. https://doi.org/10.1017/S2045796012000406
Geiger, E. J., Pruessner, L., Barnow, S., & Joormann, J. (2023). Empathy is associated with interpersonal emotion regulation goals in everyday life. Emotion. https://doi.org/10.1037/emo0001332
Gross, J. J., & John, O. P. (2003). Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology, 85(2), 348–362. https://doi.org/10.1037/0022-3514.85.2.348
Gunn, C. K., & Donahue, J. J. (2022). Intra- and interpersonal emotion regulation strategies and Schizotypic personality characteristics. Journal of Psychopathology and Behavioral Assessment. https://doi.org/10.1007/s10862-022-09987-3
Grund, S., Lüdtke, O., & Robitzsch, A. (2016). Multiple imputation of multilevel missing data. SAGE Open, 6(4), 215824401666822. https://doi.org/10.1177/2158244016668220
Häfner, H., Nowotny, B., Löffler, W., an der Heiden, W., & Maurer, K. (1995). When and how does schizophrenia produce social deficits? European Archives of Psychiatry and Clinical Neuroscience, 246(1), 17–28. https://doi.org/10.1007/BF02191811
Henrich, J., Heine, S. J., & Norenzayan, A. (2010). The weirdest people in the world? Behavioral and Brain Sciences, 33(2–3), 61–83. https://doi.org/10.1017/S0140525X0999152X
Hofmann, S. G. (2014). Interpersonal emotion regulation model of mood and anxiety disorders. Cognitive Therapy and Research, 38(5), 483–492. https://doi.org/10.1007/s10608-014-9620-1
Hofmann, S. G., Carpenter, J. K., & Curtiss, J. (2016). Interpersonal Emotion Regulation Questionnaire (IERQ): scale development and psychometric characteristics. Cognitive Therapy and Research, 40(3), 341–356. https://doi.org/10.1007/s10608-016-9756-2
Hofmann, S. G., & Doan, S. N. (2018). The social Foundations of Emotion: Developmental, Cultural, and Clinical Dimensions. American Psychological Association.
Howes, O. D., & Murray, R. M. (2014). Schizophrenia: An integrated sociodevelopmental-cognitive model. The Lancet, 383(9929), 1677–1687. https://doi.org/10.1016/S0140-6736(13)62036-X
Jaya, E. S., Pillny, M., Lincoln, T. M., & Riehle, M. (2022). Does social defeat cause negative symptoms? A prospective study in a multi-national community sample. Comprehensive Psychiatry. https://doi.org/10.1016/j.comppsych.2021.152289
Jaya, E. S., van Amelsvoort, T., Bartels-Velthuis, A. A., Bruggeman, R., Cahn, W., de Haan, L., Kahn, R. S., van Os, J., Schirmbeck, F., Simons, C. J. P., & Lincoln, T. M. (2021). The Community Assessment of Psychic Experiences: Optimal cut-off scores for detecting individuals with a psychotic disorder. International Journal of Methods in Psychiatric Research, 30(4), e1893. https://doi.org/10.1002/MPR.1893
Jeganathan, J., & Breakspear, M. (2021). An active inference perspective on the negative symptoms of schizophrenia. The Lancet Psychiatry, 8(8), 732–738. https://doi.org/10.1016/S2215-0366(20)30527-7
Kimhy, D., Gill, K. E., Brucato, G., Vakhrusheva, J., Arndt, L., Gross, J. J., & Girgis, R. R. (2016). The impact of emotion awareness and regulation on social functioning in individuals at clinical high risk for psychosis. Psychological Medicine, 46(14), 2907–2918. https://doi.org/10.1017/S0033291716000490
Kirkpatrick, B., Strauss, G. P., Nguyen, L., Fischer, B. A., Daniel, D. G., Cienfuegos, A., & Marder, S. R. (2010). The brief negative symptom scale : psychometric properties. Schizophrenia Bulletin. https://doi.org/10.1093/schbul/sbq059
Kleiman, E. (2021). EMAtools: Data Management Tools for Realt-Time Monitoring/Ecological Momentary Assessment Data. https://cran.r-project.org/package=EMAtools
Koç, M. S., Aka, B. T., Doğruyol, B., Curtiss, J., Carpenter, J. K., & Hofmann, S. G. (2019). Psychometric properties of the Turkish version of the Interpersonal Emotion Regulation Questionnaire (IERQ). Journal of Psychopathology and Behavioral Assessment, 41(2), 294–303. https://doi.org/10.1007/s10862-019-09732-3
Kramer, I., Simons, C. J. P., Wigman, J. T. W., Collip, D., Jacobs, N., Derom, C., Thiery, E., van Os, J., Myin-Germeys, I., & Wichers, M. (2013). Time-lagged moment-to-moment interplay between negative affect and paranoia: new insights in the affective pathway to psychosis. Schizophrenia Bulletin. https://doi.org/10.1093/schbul/sbs194
Kring, A. M., Gur, R. E., Blanchard, J. J., Horan, W. P., & Reise, S. P. (2013). The Clinical Assessment Interview for Negative Symptoms (CAINS): Final development and validation. The American Journal of Psychiatry, 170(2), 165–172. https://doi.org/10.1176/appi.ajp.2012.12010109
Krkovic, K., Clamor, A., Schlier, B., & Lincoln, T. M. (2019). Emotions and Persecutory Ideation in Daily Life: On the Trail of the “Chicken and Egg” Problem. Journal of Abnormal Psychology. https://doi.org/10.1037/ABN0000495
Kwapil, T. R., Brown, L. H., Silvia, P. J., Myin-Germeys, I., & Barrantes-Vidal, N. (2012). The expression of positive and negative schizotypy in daily life: an experience sampling study. Psychological Medicine, 42(12), 2555–2566. https://doi.org/10.1017/S0033291712000827
Kwapil, T. R., Kemp, K. C., Mielock, A., Sperry, S. H., Chun, C. A., Gross, G. M., & Barrantes-Vidal, N. (2020). Association of multidimensional schizotypy with psychotic-like experiences, affect, and social functioning in daily life: Comparable findings across samples and schizotypy measures. Journal of Abnormal Psychology, 129(5), 492–504. https://doi.org/10.1037/abn0000522
Larson, F. V., Wagner, A. P., Chisholm, K., Reniers, R. L. E. P., & Wood, S. J. (2020). Adding a Dimension to the Dichotomy: Affective Processes Are Implicated in the Relationship Between Autistic and Schizotypal Traits. Frontiers in Psychiatry. https://doi.org/10.3389/fpsyt.2020.00712
Lincoln, T. M., Schulze, L., & Renneberg, B. (2022). The role of emotion regulation in the characterization, development and treatment of psychopathology. Nature Reviews Psychology, 1(5), 272–286. https://doi.org/10.1038/s44159-022-00040-4
Liu, D. Y., Strube, M. J., & Thompson, R. J. (2021). Interpersonal emotion regulation: an experience sampling study. Affective Science, 2(3), 273–288. https://doi.org/10.1007/s42761-021-00044-y
Llerena, K., Park, S. G., McCarthy, J. M., Couture, S. M., Bennett, M. E., & Blanchard, J. J. (2013). The Motivation and Pleasure Scale-Self-Report (MAP-SR): Reliability and validity of a self-report measure of negative symptoms. Comprehensive Psychiatry, 54(5), 568–574. https://doi.org/10.1016/j.comppsych.2012.12.001
Ludwig, L., Mehl, S., Schlier, B., Krkovic, K., & Lincoln, T. M. (2020). Awareness and rumination moderate the affective pathway to paranoia in daily life. Schizophrenia Research, 216, 161–167. https://doi.org/10.1016/j.schres.2019.12.007
Marder, S. R., & Galderisi, S. (2017). The current conceptualization of negative symptoms in schizophrenia. World Psychiatry, 16(1), 14–24. https://doi.org/10.1002/wps.20385
Marroquín, B. (2011). Interpersonal emotion regulation as a mechanism of social support in depression. Clinical Psychology Review, 31(8), 1276–1290. https://doi.org/10.1016/j.cpr.2011.09.005
Matthews, V. S., Stough-Hunter, A., & Marazita, J. M. (2021). Attitudes towards social distancing in response to COVID-19. Public Health Nursing, 38(6), 1019–1029. https://doi.org/10.1111/phn.12954
Minor, K. S., Hardin, K. L., Beaudette, D. M., Waters, L. C., White, A. L., Gonzenbach, V., & Robbins, M. L. (2020). Social functioning in schizotypy: How affect influences social behavior in daily life. Journal of Clinical Psychology, 76(12), 2212–2221. https://doi.org/10.1002/jclp.23010
Modenato, C., & Draganski, B. (2015). The concept of schizotypy — A computational anatomy perspective. Schizophrenia Research: Cognition, 2(2), 89–92. https://doi.org/10.1016/j.scog.2015.05.001
Mueller, I., Pruessner, L., Holt, D. V., Zimmermann, V., Schulze, K., Strakosch, A.-M., & Barnow, S. (2024). If it Ain’t Broke, Don’t Fix it: Positive Versus Negative Emotion Regulation in Daily Life and Depressive Symptoms. Journal of Affective Disorders, 348, 398–408. https://doi.org/10.1016/j.jad.2023.12.037
Nittel, C. M., Lincoln, T. M., Lamster, F., Leube, D., Rief, W., Kircher, T., & Mehl, S. (2018). Expressive suppression is associated with state paranoia in psychosis: An experience sampling study on the association between adaptive and maladaptive emotion regulation strategies and paranoia. British Journal of Clinical Psychology, 57(3), 291–312. https://doi.org/10.1111/bjc.12174
Niven, K., Totterdell, P., Stride, C. B., & Holman, D. (2011). Emotion Regulation of Others and Self (EROS): the development and validation of a new individual difference measure. Current Psychology, 30(1), 53–73. https://doi.org/10.1007/s12144-011-9099-9
Osborne, K. J., Willroth, E. C., DeVylder, J. E., Mittal, V. A., & Hilimire, M. R. (2017). Investigating the association between emotion regulation and distress in adults with psychotic-like experiences. Psychiatry Research, 256, 66–70. https://doi.org/10.1016/j.psychres.2017.06.011
Paul, S., Pruessner, L., Strakosch, A.-M., Schulze, K., Miano, A., & Barnow, S. (2023). Examining the Strategy-Situation Fit of Emotion Regulation in Everyday Social Contexts. Emotion. https://doi.org/10.1037/emo0001209
Petrova, K., & Gross, J. J. (2023). The Future of Emotion Regulation Research: Broadening Our Field of View. Affective Science, 4(4), 609–616. https://doi.org/10.1007/s42761-023-00222-0
Pillny, M., Krkovic, K., & Lincoln, T. M. (2018). Development of the Demotivating Beliefs Inventory and Test of the Cognitive Triad of Amotivation. Cognitive Therapy and Research, 42(6), 867–877. https://doi.org/10.1007/s10608-018-9940-7
Pillny, M., Schlier, B., & Lincoln, T. M. (2020). “I just don’t look forward to anything”. How anticipatory pleasure and negative beliefs contribute to goal-directed activity in patients with negative symptoms of psychosis. Schizophrenia Research, 222, 429–436. https://doi.org/10.1016/j.schres.2020.03.059
Pruessner, L., Holt, D. V., Gölz, R., Sevcenko, N., Hofmann, S. G., & Backenstrass, M. (2020). Psychometrische Eigenschaften der deutschsprachigen Version des Interpersonal Emotion Regulation Questionnaire. Diagnostica, 66(1), 62–73. https://doi.org/10.1026/0012-1924/a000239
Raugh, I. M., & Strauss, G. P. (2022). Deconstructing emotion regulation in schizophrenia: The nature and consequences of abnormalities at the identification stage. European Archives of Psychiatry and Clinical Neuroscience, 272(6), 1061–1071. https://doi.org/10.1007/s00406-021-01350-z
Rector, N. A., Katz, D. E., Quilty, L. C., Laposa, J. M., Collimore, K., & Kay, T. (2019). Reassurance seeking in the anxiety disorders and OCD: Construct validation, clinical correlates and CBT treatment response. Journal of Anxiety Disorders, 67, 102109. https://doi.org/10.1016/j.janxdis.2019.102109
Riehle, M. (in press). Interpersonal risk factors for negative symptoms. In T. M. Lincoln, M. Brown, & D. Kimhy (Eds.), Negative Symptoms in Psychosis: Psychological and Social Approaches for Clinicians and Researchers. Oxford University Press.
Riehle, M., & Lincoln, T. M. (2017). Social consequences of subclinical negative symptoms: An EMG study of facial expressions within a social interaction. Journal of Behavior Therapy and Experimental Psychiatry, 55, 90–98. https://doi.org/10.1016/j.jbtep.2017.01.003
Riehle, M., Mehl, S., & Lincoln, T. M. (2018). The specific social costs of expressive negative symptoms in schizophrenia: Reduced smiling predicts interactional outcome. Acta Psychiatrica Scandinavica, 138(2), 133–144. https://doi.org/10.1111/acps.12892
Rights, J. D., & Sterba, S. K. (2019). Quantifying explained variance in multilevel models: An integrative framework for defining R-squared measures. Psychological Methods, 24(3), 309–338. https://doi.org/10.1037/met0000184
Schlier, B., Jaya, E. S., Moritz, S., & Lincoln, T. M. (2015). The Community Assessment of Psychic Experiences measures nine clusters of psychosis-like experiences: A validation of the German version of the CAPE. Schizophrenia Research, 169(1–3), 274–279. https://doi.org/10.1016/j.schres.2015.10.034
Schlier, B., Moritz, S., & Lincoln, T. M. (2016). Measuring fluctuations in paranoia: Validity and psychometric properties of brief state versions of the Paranoia Checklist. Psychiatry Research, 241, 323–332. https://doi.org/10.1016/j.psychres.2016.05.002
Schwartz, E. K., Le, T. P., & Cohen, A. S. (2022). Sharing positive events: Ecological momentary assessment of emotion regulation via social capitalization in schizotypy. Psychiatry Research, 308, 114377. https://doi.org/10.1016/j.psychres.2021.114377
Silvia, P. J., & Kwapil, T. R. (2011). Aberrant Asociality: How Individual Differences in Social Anhedonia Illuminate the Need to Belong. Journal of Personality, 79(6), 1315–1332. https://doi.org/10.1111/j.1467-6494.2010.00702.x
Springstein, T., Hamerling-Potts, K. K., Landa, I., & English, T. (2022). Adult attachment and interpersonal emotion regulation motives in daily life. Emotion. https://doi.org/10.1037/emo0001169
Stefanis, N. C., Hanssen, M., Smirnis, N. K., Avramopoulos, D. A., Evdokimidis, I. K., Stefanis, C. N., Verdoux, H., & van Os, J. (2002). Evidence that three dimensions of psychosis have a distribution in the general population. Psychological Medicine, 32(2), 347–358. https://doi.org/10.1017/S0033291701005141
Steinmetz, H., Batzdorfer, V., Scherhag, J., & Bosnjak, M. (2022). The ZPID Lockdown Measures Dataset for Germany. PsychArchives. https://doi.org/10.23668/PSYCHARCHIVES.6676
Strauss, G. P., Pelletier-Baldelli, A., Visser, K. F., Walker, E. F., & Mittal, V. A. (2020). A review of negative symptom assessment strategies in youth at clinical high-risk for psychosis. In Schizophrenia Research (Vol. 222, pp. 104–112). Elsevier B.V. https://doi.org/10.1016/j.schres.2020.04.019
Tran, A., Greenaway, K. H., Kostopoulos, J., O’Brien, S. T., & Kalokerinos, E. K. (2023). Mapping interpersonal emotion regulation in everyday Life. Affective Science, 4(4), 672–683. https://doi.org/10.1007/s42761-023-00223-z
van der Velde, J., Swart, M., van Rijn, S., van der Meer, L., Wunderink, L., Wiersma, D., Krabbendam, L., Bruggeman, R., & Aleman, A. (2015). Cognitive Alexithymia Is Associated with the Degree of Risk for Psychosis. PLoS One, 10(6), e0124803. https://doi.org/10.1371/journal.pone.0124803
van Os, J., Linscott, R. J., Myin-Germeys, I., Delespaul, P., & Krabbendam, L. (2009). A systematic review and meta-analysis of the psychosis continuum: Evidence for a psychosis proneness–persistence–impairment model of psychotic disorder. Psychological Medicine, 39(2), 179–195. https://doi.org/10.1017/S0033291708003814
van Rijn, S., Schothorst, P., WoutSprong, M. M., Ziermans, T., van Engeland, H., Aleman, A., & Swaab, H. (2011). Affective dysfunctions in adolescents at risk for psychosis: Emotion awareness and social functioning. Psychiatry Research, 187(1–2), 100–105. https://doi.org/10.1016/j.psychres.2010.10.007
Visser, K. F., Esfahlani, F. Z., Sayama, H., & Strauss, G. P. (2018). An ecological momentary assessment evaluation of emotion regulation abnormalities in schizophrenia. Psychological Medicine, 48(14), 2337–2345. https://doi.org/10.1017/S0033291717003865
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54(6), 1063–1070. https://doi.org/10.1037/0022-3514.54.6.1063
Werbeloff, N., Dohrenwend, B. P., Yoffe, R., van Os, J., Davidson, M., & Weiser, M. (2015). The Association between Negative Symptoms, Psychotic Experiences and Later Schizophrenia: A Population-Based Longitudinal Study. PLoS ONE, 10(3), e0119852. https://doi.org/10.1371/journal.pone.0119852
White, R. G., Laithwaite, H., & Gilbert, P. (2013). Negative symptoms in schizophrenia. The role of social defeat. In A. Gumley, A. Gillham, K. Taylor, & M. Schwannauer (Eds.), Psychosis and Emotion (pp. 178–190). Routledge.
Williams, W. C., Morelli, S. A., Ong, D. C., & Zaki, J. (2018). Interpersonal emotion regulation: Implications for affiliation, perceived support, relationships, and well-being. Journal of Personality and Social Psychology, 115(2), 224–254. https://doi.org/10.1037/pspi0000132
Yang, Y., Yang, Z., Zou, Y., Shi, H., Wang, Y., Xie, D., Zhang, R., Lui, S. S. Y., Cohen, A. C., Strauss, G. P., Cheung, E. F. C., & Chan, R. C. K. (2018). Low-pleasure beliefs in patients with schizophrenia and individuals with social anhedonia. Schizophrenia Research, 201, 137–144. https://doi.org/10.1016/j.schres.2018.05.018
Yee, C. I., Strauss, G. P., Allen, D. N., Haase, C. M., Kimhy, D., & Mittal, V. A. (2019). Trait emotional experience in individuals with schizophrenia and youth at clinical high risk for psychosis. Bjpsych Open, 5(5), e78. https://doi.org/10.1192/bjo.2019.64
Zaki, J., & Williams, W. C. (2013). Interpersonal emotion regulation. Emotion, 13(5), 803–810. https://doi.org/10.1037/a0033839
Acknowledgements
We would like to thank all participants and Nina Bach and Banu Dalmis for their help with the data collection.
Funding
Open Access funding enabled and organized by Projekt DEAL. This work did not receive external funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
All authors declare that they have no conflicts of interest regarding this work.
A preprint of this article has been posted on psyarxiv.com/pmzna/. All data and analysis code needed to reproduce the analyses of this report are available at https://doi.org/10.23668/psycharchives.12663.
Marcel Riehle served as lead for conceptualization, formal analysis, methodology, project administration, visualization, and writing the original draft and in a supervising role for the investigation and data curation. Luise Pruessner supported writing the original draft, formal analysis, validation, and methodology and provided key revisions and editing. Saskia Brauer performed the data curation and was involved with the investigation, validation, formal analysis, and revision and editing. Tania M. Lincoln supported the conceptualization and provided substantial revision and editing in all stages.
Informed Consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (national and institutional). Informed consent was obtained from all individual subjects participating in the study.
Animal Rights Statements
No animal studies were carried out by the authors for this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Riehle, M., Brauer, S., Lincoln, T.M. et al. Interpersonal Emotion Regulation in Young Adults With Low and High Psychosis Proneness: A Diary Study. Cogn Ther Res (2024). https://doi.org/10.1007/s10608-024-10525-6
Accepted:
Published:
DOI: https://doi.org/10.1007/s10608-024-10525-6