
Abstract
Prolonged high-intensity endurance exercise has been reported to have adverse effects on the heart, which are further correlated with exercise dose. However, its effect on the right ventricle (RV) of amateur runners is unknown. This study aimed was to evaluate the early right ventricular structure and systolic function of amateur marathon runners by three-dimensional speckle tracking echocardiography (3D-STE), and to further analyze the correlation between relevant parameters and the amount of training. A total of 30 amateur marathon runners (marathon group) and 27 healthy volunteers (control group) were enrolled. Conventional echocardiography combined with 3D-STE was performed in all subjects, and the marathon group was screened by echocardiography a week before a marathon (V1), within 1 h post-marathon (V2), and 4 days post-marathon (V3). RV global longitudinal strain (GLS) and RV end-diastolic volume (EDV) increased significantly in the marathon group compared to the control group (P < 0.05). RV GLS was significantly decreased in the marathon group within 1 h post-marathon (V1: − 26.2 ± 2.5% vs V2: − 23.0 ± 1.6% vs V3: − 25.6 ± 2.6%, P < 0.001). However, there was no significant difference in RV ejection fraction (RVEF) (P > 0.05). The results of the correlation analysis showed that RV EDV and RV end-systolic volume (ESV) were positively correlated with the average training volume (P < 0.001). Multivariate linear regression analysis showed that average training volume was an independent predictor of RV EDV in amateur marathoners (β = 0.642, P < 0.001). The systolic function of the RV was enhanced in amateur marathon runners in the early stage, manifested by an increase in RV EDV. After a long period of high-intensity endurance exercise, RV systolic function will temporarily be reduced. 3D-STE can identify this subclinical change with high sensitivity and provide valuable information to assess the structure and function of RV in amateur marathon runners.
Similar content being viewed by others


Introduction
A marathon is a popular long-distance exercise in China. With an increase in amateur marathon runners participating, there is growing concern about the effects of marathon running on the heart [1]. Regular and moderate exercise benefits physical health, while long-term high-intensity exercise may increase the risk of cardiovascular disease [2, 3]. Repeated high-intensity endurance exercise induces the body to produce a series of adaptation phenomena, such as enlargement of the heart cavity and thickening of the chamber wall, which is called the "athlete heart" [4]. The "athlete heart" has been reported to be a healthy and highly efficient adaptation to long-term high-intensity exercise [5]. However, left ventricular (LV) function has been confirmed to temporarily be impaired after intense exercise in professional athletes [6, 7]. Additionally, increasing evidence has shown that due to the different compensatory abilities of the pulmonary and systemic circulations, exercise-induced overload affects primarily the right ventricle (RV), and the effects are more apparent earlier than the effects on the left ventricle [8, 9], and some studies suggested the risk of "exercise-induced arrhythmia" [10,11,12].
Due to the irregular geometry and complex anatomical structure of the RV, it is challenging to quantitatively evaluate its function by two-dimensional echocardiography [13]. Three-dimensional speckle tracking echocardiography (3D-STE) is a new technology based on real-time three-dimensional echocardiography and two-dimensional speckle tracking technology, which can accurately and quantitatively assess myocardial motion and chamber capacity and detect subclinical changes in ventricular systolic function in the early stage with high sensitivity [14]. Previous studies have shown that the volume and strain values measured by 3D-STE are highly correlated with cardiac magnetic resonance [15].
Therefore, this study aims to analyze the early structural and functional changes of the right ventricular in amateur marathon runners by 3D-STE, to further elaborate the characteristics of heart remodeling in amateur marathon runners, and to provide a more in-depth theoretical basis for clinical guidance.
Materials and methods
Study population
From October 2020 to December 2022, we recruited 30 amateur marathon runners in Hangzhou, including 22 males and 8 females, aged between 27 and 51 years, with an average age of 38.77 ± 1.17 years. Clinical data such as age, body mass index, blood pressure, heart rate, competition times, and total training volume were recorded. The inclusion criteria are summarized as follows: (a) participating in marathon running for less than 3 years, (b) having completed a formal full marathon (42.195 km) at least once, (c) the average weekly running frequency ≥ 3 times, and the distance of each exercise ≥ 10 km, and (d) no strenuous exercise in the week before the marathon. Marathon runners were excluded if they had a history of congenital heart disease, hypertension, valvular heart disease, diabetes, kidney disease, and other systemic diseases. Marathon runners who have been involved in strength sports for a long time or were professional athletes were also excluded. 27 age- and sex-matched healthy sedentary subjects, including 21 males and 6 females, between 25 and 48 years old, with an average age of 36.00 ± 1.19 years were enrolled as controls. Control subjects had normal physical examinations, electrocardiograms, and echocardiograms. The Ethics Committee of the Affiliated Hospital of Hangzhou Normal University (Ethical approval number 2020E2-hS-001) approved the study. All participants had signed an informed consent form.
Conventional echocardiography
We used EPIQ 7C color Doppler echocardiography diagnostic instrument (Philips Medical Systems) equipped with an X5-1 probe (1 ~ 5MHZ). Echocardiography was performed at the following time points: a week before a marathon (V1), within 1 h post-marathon (V2), and 4 days post-marathon (V3).
Conventional echocardiography was performed according to the American Society of Echocardiography (ASE) recommended guidelines. Parameters of the right atrial diameter(RAD), RV area and LV volume were obtained, and the LV ejection fraction (LVEF) was obtained by the biplane Simpson method from the apical two- and four-chamber views. In the RV-focused apical four-chamber view, tricuspid annular plane systolic excursion (TAPSE-2D) was measured in M-mode, the systolic velocity of the lateral tricuspid annular peak (S’) and the RV myocardial performance index (MPI) was measured by pulsed wave tissue Doppler imaging, and RV fraction area change (FAC-2D) was calculated as (RV end-diastolic area—RV end-systolic area)/RV end-diastolic area × 100%.
Three-dimensional speckle-tracking echocardiography
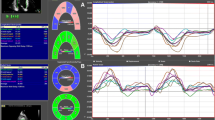
Off-line analysis workstation TomTec 3.2 software (4D RV-Analysis 2.0, Germany). RV-focused 3D full-volume images were acquired with a frame rate > 60 frames/s. After manually determining the landmarks, the software automatically tracked the RV endocardium in the apical four-chamber and three short-axis views during the cardiac cycle, and then reconstructed the 3D model of the RV. If not satisfied with the tracking effect, you can adjust it manually. Finally, the software automatically generated RV end-diastolic volume (EDV), RV end-systolic volume (ESV), RVEF, TAPSE-3D, RV FAC-3D, RV free wall longitudinal strain (FLS), RV septal wall longitudinal strain (SLS), and obtained the RV volume-time curve (Fig. 1).

Three-dimensional speckle tracking imaging parameters of the right ventricle Offline analysis and volume-time curve. Manual determination of the points reference (A), track right ventricle endocardium (B), volume-time curve of the control group (C), volume-time curve of the marathon group (D)
Reproducibility analysis
Ten cases were randomly selected from the athlete group and the control group. The same observers measured the 3D-STE parameters two weeks later to evaluate the intraobserver differences. Differences between observers were evaluated by measuring relevant data by another experienced physician who was not involved in the study. The intraobserver and interobserver variations were expressed as correlation coefficients (ICC).
Statistical analysis
Statistical analysis was performed using SPSS software version 22.0 (IBM, Chicago, IL, USA). The measured data was tested for normality using the Shapiro–Wilk test. Continuous variables were described as mean ± standard deviation for normally distributed variables and median and interquartile range (IQR) for nonnormally distributed variables. Categorical variables were described as frequencies and percentages and compared using Fisher’s exact test. For comparison between the two groups, the LSD-T test was used for variables that were normally distributed and the Mann–Whitney U test for variables with non-normal distribution. Differences between groups were compared using one-way ANOVA for continuous variables and the Kruskal–Wallis test for skewed variables. Spearman or Pearson’s correlation was used to test the correlation between clinical data and three-dimensional parameters. Multiple linear regression was used to analyze the predictive factors of RVEDV in amateur marathon runners. All statistical tests were two-sided and the P value < 0.05 was considered statistically significant.
Result
Clinical and demographic characteristics
A total of 30 amateur marathon runners and 27 healthy sedentary controls were included in the statistical analysis. Baseline demographic characteristics are summarized in Table 1. The heart rate of the marathon group was significantly lower than that of the control group (P < 0.05). There were no significant differences in age, body mass index, body surface area, systolic blood pressure, and diastolic blood pressure between the two groups (P > 0.05).
Conventional echocardiographic characteristic
The conventional echocardiographic parameters of the study population at baseline and during follow-up are shown in Table 2. The marathon group had significantly higher RAD1 and RAD2 compared to the control group (P < 0.05). However, there were no significant differences in LVEF, TAPSE-2D, S’ and RV FAC-2D (P < 0.05). Within the marathon group, TAPSE-2D was significantly lower and MPI was significantly higher within 1 h post-marathon compared to 1 week before a marathon and 4 days post-marathon (P < 0.05).
Three-dimensional speckle-tracking echocardiographic characteristic
The RV 3D-STE parameters are shown in Table 3 and Fig. 2. We found that RV EDV, RVEF, TAPSE-3D, RV FAC-3D, RV FLS, RV SLS and RV GLS of the marathon group increased significantly compared to the control group (P < 0.05). Within the marathon group, TAPSE-3D, RV FAC-3D, RV FLS, RV SLS and RV GLS within 1 h post-marathon were significantly lower than 1 week before the marathon and 4 days post-marathon (P < 0.05). However, there was no statistically significant difference in RVEF between the three time points of marathon runners (P > 0.05).

Comparison of the differences between the control group and the marathon group at baseline and during follow-up. For right ventricular end-diastolic volume, right ventricular ejection fraction, right ventricular global longitudinal strain, and right ventricular freewall longitudinal strain
Correlation analysis of amateur marathon runners
We found that RVEF and the average training volume were significantly correlated with the 3D-STE parameters in amateur marathon runners, the results of the correlation analysis are shown in Table 4 and Fig. 3. RV ESV (r = − 0.670, P < 0.001), RV GLS (r = − 0.485, P = 0.007) and RV FLS (r = − 0.505, P = 0.004) were negatively correlated with RVEF, while RV FAC-3D (r = 0.841, P < 0.001) was positively correlated with RVEF. RV EDV (r = 0.736, P < 0.001) and RV ESV (r = 0.638, P < 0.001) were positively correlated with the average training volume. Multiple linear regression analysis showed that the average training volume was an independent predictor of RV EDV in amateur marathon runners (β = 0.642, P < 0.001), as shown in Table 5.

Correlation of RVEF and the average training volume with the 3D-STE parameters.Associations between RV EDV and the average training volume (A). Associations between RVEF and RV FAC (B); RV FLS (C); and RV GLS (D). RV EDV, right ventricular end-diastolic volume; RVEF, right ventricular ejection fraction; RV FAC, right ventricular fractional area change; RV FLS, right ventricular septal wall longitudinal strain; RV GLS, right ventricular global longitudinal strain
Reproducibility test
The RV 3D-STE parameters were highly reproducible at both the interobserver and intraobserver levels. Interobservation measurements showed an interclass correlation of 0.82 for RV EDV, 0.89 for RVEF, 0.82 for RV FLS and 0.80 for RV SLS. Similarly, intraobservation measurements showed an intraclass correlation of 0.81 for RV EDV, 0.93 for RVEF, 0.91 for RV FLS and 0.84 for RV SLS, as shown in Fig. 4.

Bland–Altman analysis of RVEF and RV FLS. RVEF, right ventricular ejection fraction; RV FLS, right ventricular freewall longitudinal strain
Discussion
In this study, we performed a comprehensive and quantitative assessment of RV structure and systolic function in early amateur marathoners using 3D-STE. The main findings are as follows: (i). Amateur marathon runners have a higher early RV volume and better systolic function than the sedentary control group; (ii). The RV systolic function of amateur marathon runners may decrease transiently within 1 h post-marathon and would return to the baseline level 4 days post-marathon. 3D-STE is able to accurately identify this subtle change; (iii).RV volume was significantly associated with mean training volume in early amateur marathon runners, which has rarely been mentioned in previous studies.
We observed that the heart rate of amateur marathon runners was significantly lower than that of sedentary control. This lower heart rate in the resting state is likely due to long-term high-intensity endurance exercise increasing the vagal nerve tone of marathon runners and decreasing their sympathetic nerve tone [16], suggesting good cardiac reserve in the non-exercise state [17]. High-intensity endurance exercise will cause volume overload and increased atrial pressure [18]. In this study, the 3D-STE results showed that RV EDV, RVEF, TAPSE-3D, RV FAC-3D, RV FLS, RV SLS, and RV GLS of amateur marathon runners were higher than those of the control group. This result indicates that, to meet the body's demand for hyper ejection, the RV cavity is enlarged and the RV systolic function is enhanced in early amateur marathon runners [19]. Vitarelli et al. found [20] that patients with atrial septal defect also had enhanced right ventricular systolic function caused by chronic RV volume overload, and Esposito R et al. found [21] that the association between the longitudinal deformation of the free ventricle wall and the preload of rowers was independent of the effect induced by changes in afterload. These previous studies indicated that when the RV preload increased, the wall stress is maintained by the expansion of the chamber. Furthermore, the end-systolic volume is maintained at an early stage, while systolic function is enhanced through the Frank-starling law, which effectively compensates for changes in hemodynamic conditions [19, 22]. Studies have shown that the atrial pressure of professional athletes will be 7 ml/m2 higher than that of the general population [23]. Lewicka-Potocka et al. also found [4] that the left and right atrial sizes of recreational athletes were larger than those of a sedentary control group and were associated with the distance to training. In the present study, RAD1 and RAD2 also increased in amateur marathon runners compared to the control group, indicating that the size of RA would be compensated for with increased RV preload to allow greater volume delivery and increased cardiac output [24].
Our results showed that TAPSE-3D, RV FAC-3D, RV FLS, RV SLS, and RV GLS of amateur marathon runners were significantly lower within 1 h post-marathon, suggesting that under different load conditions, different changes in RV systolic function would lead to. During high-intensity endurance exercise, cardiac output is 7 times higher than in a normal resting state, which will inevitably lead to an increase in pulmonary vascular pressure and an increase in RV wall stress [9, 11]. Additionally, increased oxidative stress and myocardial damage together will cause transient RV systolic dysfunction [25]. However, there was no significant decrease in RVEF, which may be due to the compensatory increase in RV myocardium in other motor components, which allows RVEF to be within the normal range [26]. It is also further confirmed that 3D-STE can more sensitively recognize subtle damages to the RV myocardium.
In this study, we found that the 3D-STE parameters RV FLS, RV GLS, and RV FAC-3D of amateur marathon runners were significantly correlated with RVEF. Therefore, 3D-STE is a more accurate and reliable technique. We also found that RV EDV and RV ESV of amateur marathon runners were significantly correlated with the average training volume, suggesting that the early RV volume and RV systolic function of amateur marathon runners increased with the average training volume to meet the phenomenon of ventricular adaptation induced by endurance exercise [27]. This result fully reflects the intrinsic physiological characteristics of RV remodeling in amateur marathon runners [28]. The results of multivariate linear regression showed that the average training volume was an independent factor associated with the increase in RV EDV in amateur marathon runners. Recent data indicate that RV systolic function is impaired under high training load, suggesting the non-linear relationship between training volume and the incidence of cardiovascular complications [26]. We speculate that RV systolic function in the early stages may be manifested primarily by an increase in EDV, and when EDV reaches a certain threshold, RV systolic dysfunction occurs due to excessive volume, increased wall stress, and myocardial fibrosis [29]. Therefore, with the change in training volume in the early stage of amateur marathon runners, the RV of the body will produce adaptive remodeling but not intrinsic dysfunction.
Limitations
This study only assessed amateur marathon runners in the early stages and the number of cases was limited, and professional marathon runners were not included for comparison. The index of cardiopulmonary function, such as maximum oxygen consumption (VO2 max), was not obtained. RV afterload parameters such as pulmonary artery pressure were not analyzed due to small tricuspid regurgitation. The statistical analysis of the parameters of each segment of 3D-STE longitudinal strain in amateur marathon runners has not been carried out, which will be further studied in the follow-up study.
Conclusions
The longitudinal systolic function of RV of amateur marathon runners increases in the early stage, which is a good adaptation to endurance exercise. There are transient subclinical changes but no dysfunction in RV systolic function after high-intensity endurance exercise. 3D-STE is a practical and feasible echocardiographic technique to evaluate the dynamics of myocardial deformation, which is capable of identifying subtle changes in the myocardium comprehensively.
Data availability
The data in the current study are available from the corresponding author upon reasonable request.
References
D’Silva A, Bhuva AN, van Zalen J, Bastiaenen R, Abdel-Gadir A, Jones S, Nadarajan N, Medina M, Katia D, Ye Y, Augusto J, Treibel TA, Rosmini S, Ramlall M, Scully PR, Torlasco C, Willis J, Finocchiaro G, Papatheodorou E, Dhutia H, Cole D, Ster C, Irina H, Alun D, Sharma R, Manisty C, Lloyd G, Moon JC, Sharma S (2020) Cardiovascular remodeling experienced by real-world, unsupervised. Young Novice Marathon Runners Front Physiol 11:232. https://doi.org/10.3389/fphys.2020.00232
Pelliccia A, Sharma S, Gati S, Bäck M, Börjesson M, Caselli S, Collet J-P, Corrado D, Drezner JA, Halle M, Hansen D, Heidbuchel H, Myers J, Niebauer J, Papadakis M, Piepoli MF, Prescott E, Roos-Hesselink JW, Graham Stuart A, Taylor RS, Thompson PD, Tiberi M, Vanhees L, Wilhelm M (2021) 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur Heart J 42:17–96. https://doi.org/10.1093/eurheartj/ehaa605
Nystoriak MA, Bhatnagar A (2018) Cardiovascular Effects and Benefits of Exercise. Front Cardiovasc Med 5:135. https://doi.org/10.3389/fcvm.2018.00135
Lewicka-Potocka Z, Dąbrowska-Kugacka A, Lewicka E, Kaleta AM, Dorniak K, Daniłowicz-Szymanowicz L, Fijałkowski M, Nabiałek-Trojanowska I, Ratkowski W, Potocki W, Raczak G (2021) The “athlete’s heart” features in amateur male marathon runners. Cardiol J 28:707–715. https://doi.org/10.5603/CJ.a2019.0110
La Gerche A, Burns AT, D’Hooge J, Macisaac AI, Heidbüchel H, Prior DL (2012) Exercise strain rate imaging demonstrates normal right ventricular contractile reserve and clarifies ambiguous resting measures in endurance athletes. J Am Soc Echocardiogr 25:253-262.e1. https://doi.org/10.1016/j.echo.2011.11.023
Lord RN, Utomi V, Oxborough DL, Curry BA, Brown M, George KP (2018) Left ventricular function and mechanics following prolonged endurance exercise: an update and meta-analysis with insights from novel techniques. Eur J Appl Physiol 118:1291–1299. https://doi.org/10.1007/s00421-018-3906-z
Roeh A, Schuster T, Jung P, Schneider J, Halle M, Scherr J (2019) Two dimensional and real-time three dimensional ultrasound measurements of left ventricular diastolic function after marathon running: results from a substudy of the BeMaGIC trial. Int J Cardiovasc Imaging 35:1861–1869. https://doi.org/10.1007/s10554-019-01634-5
Rothwell O, George K, Somauroo J, Lord R, Stembridge M, Shave R, Hoffman MD, Wilson M, Ashley E, Haddad F, Eijsvogels TMH, Oxborough D (2018) Right Ventricular Structure and Function in the Veteran Ultramarathon Runner: Is There Evidence for Chronic Maladaptation? J Am Soc Echocardiogr 31:598-605.e1. https://doi.org/10.1016/j.echo.2017.11.021
La Gerche A, Roberts T, Claessen G (2014) The response of the pulmonary circulation and right ventricle to exercise: exercise-induced right ventricular dysfunction and structural remodeling in endurance athletes (2013 Grover Conference series). Pulm Circ 4:407–416. https://doi.org/10.1086/677355
Leischik R, Dworrak B, Strauss M, Horlitz M, Pareja-Galeano H, La Guía-Galipienso FL, Giuseppe L, Carl J, Perez MV, Sanchis-Gomar F (2020) Special Article: exercise-induced right ventricular injury or arrhythmogenic cardiomyopathy (ACM): the bright side and the dark side of the moon. Progr Cardiovasc Dis 63:671–681. https://doi.org/10.1016/j.pcad.2020.03.015
Heidbüchel H, La Gerche A (2012) The right heart in athletes. Evidence for exercise-induced arrhythmogenic right ventricular cardiomyopathy. Herzschrittmacherther Elektrophysiol 23:82–86. https://doi.org/10.1007/s00399-012-0180-3
Churchill TW, Baggish AL (2017) The Right Heart: Acute and Chronic Issues. Curr Treat Options Cardiovasc Med 19:83. https://doi.org/10.1007/s11936-017-0581-z
Plášek J, Rychlý T, Drieniková D, Cisovský O, Grézl T, Homza M, Václavík J (2022) The agreement of a two- and a three-dimensional speckle-tracking global longitudinal strain. J Clin Med. https://doi.org/10.3390/jcm11092402
Li Y, Wan X, Xiao Q, Zhang Y, Sun W, Xie Y, Zeng Q, Sun Z, Yang Y, Wang J, Lv Q, Shi H, Zhang Li, Xie M (2020) Value of 3D versus 2D speckle-tracking echocardiography for RV strain measurement: validation with cardiac magnetic resonance. JACC Cardiovasc Imaging 13:2056–2058. https://doi.org/10.1016/j.jcmg.2020.04.016
Li Y, Zhang Li, Gao Y, Wan X, Xiao Q, Zhang Y, Sun W, Xie Y, Zeng Q, Chen Y, Jin Q, Wu W, Yang Y, Wang J, Lv Q, Shi H, Xie M (2021) Comprehensive assessment of right ventricular function by three-dimensional speckle-tracking echocardiography: comparisons with cardiac magnetic resonance imaging. J Am Soc Echocardiogr 34:472–482. https://doi.org/10.1016/j.echo.2020.12.013
Imai K, Sato H, Hori M, Kusuoka H, Ozaki H, Yokoyama H, Takeda H, Inoue M, Kamada T (1994) Vagally mediated heart rate recovery after exercise is accelerated in athletes but blunted in patients with chronic heart failure. J Am Coll Cardiol 24:1529–1535. https://doi.org/10.1016/0735-1097(94)90150-3
Stewart GM, Yamada A, Haseler LJ, Kavanagh JJ, Koerbin G, Chan J, Sabapathy S (2015) Altered ventricular mechanics after 60 min of high-intensity endurance exercise: insights from exercise speckle-tracking echocardiography. Am J Physiol Heart Circ Physiol 308:H875–H883. https://doi.org/10.1152/ajpheart.00917.2014
Sitges M, Merino B, Butakoff C, Garza L, De MS, Paré C, Montserrat S, Vidal B, Azqueta M, Sarquella G, Gutierrez JA, Canal R, Brugada J, Bijnens BH (2017) Characterizing the spectrum of right ventricular remodeling in response to chronic training. Int J Cardiovasc Imaging 33:331–339. https://doi.org/10.1007/s10554-016-1014-x
Voigt J-U, Cvijic M (2019) 2- and 3-Dimensional Myocardial Strain in Cardiac Health and Disease. JACC Cardiovasc Imaging 12:1849–1863. https://doi.org/10.1016/j.jcmg.2019.01.044
Vitarelli A, Sardella G, Roma D, Angelo C, Lidia C, De G, Dorazio S, Cicconetti P, Battaglia D, Caranci F, de Maio M, Bruno P, Vitarelli M, de Chiara S, Dascanio M (2012) Assessment of right ventricular function by three-dimensional echocardiography and myocardial strain imaging in adult atrial septal defect before and after percutaneous closure. Int J Cardiovasc Imaging 28:1905–1916. https://doi.org/10.1007/s10554-012-0022-8
Esposito R, Galderisi M, Schiano-Lomoriello V, Santoro A, de Palma D, Ippolito R, Muscariello R, Santoro C, Guerra G, Cameli M, Mondillo S, de Simone G (2014) Nonsymmetric myocardial contribution to supranormal right ventricular function in the athlete’s heart: combined assessment by speckle tracking and real time three-dimensional echocardiography. Echocardiography 31:996–1004. https://doi.org/10.1111/echo.12499
Kovács A, Lakatos B, Tokodi M, Merkely B (2019) Right ventricular mechanical pattern in health and disease: beyond longitudinal shortening. Heart Fail Rev 24:511–520. https://doi.org/10.1007/s10741-019-09778-1
Sanchis-Gomar F, Garatachea N, Catalán P, López-Ramón M, Lucia A, Serrano-Ostáriz E (2016) LA Size in Former Elite Athletes. JACC Cardiovasc Imaging 9:630–632. https://doi.org/10.1016/j.jcmg.2015.08.023
Ujka K, Bastiani L, D’Angelo G, Catuzzo B, Tonacci A, Mrakic-Sposta S, Vezzoli A, Giardini G, Pratali L (2017) Enhanced Right-Chamber Remodeling in Endurance Ultra-Trail Athletes Compared to Marathon Runners Detected by Standard and Speckle-Tracking Echocardiography. Front Physiol 8:527. https://doi.org/10.3389/fphys.2017.00527
Bernat-Adell MD, Collado-Boira EJ, Moles-Julio P, Panizo-González N, Martínez-Navarro I, Hernando-Fuster B, Hernando-Domingo C (2021) Recovery of inflammation, cardiac, and muscle damage biomarkers after running a marathon. J Strength Cond Res 35:626–632. https://doi.org/10.1519/JSC.0000000000003167
Lewicka-Potocka Z, Kaleta-Duss AM, Lewicka E, Kubik M, Faran A, Szymeczko P, Ska G, Rafał R, Grzegorz DB-K, Alicja (2021) Post-marathon decline in right ventricular radial motion component among amateur sportsmen. Front Physiol. https://doi.org/10.3389/fphys.2021.811764
Popple E, George K, Somauroo J, Sharma S, Utomi V, Lord R, Cooper R, Malhotra A, Forster J, Oxborough D (2018) Right ventricular structure and function in senior and academy elite footballers. Scand J Med Sci Sports 28:2617–2624. https://doi.org/10.1111/sms.13272
D’Ascenzi F, Pisicchio C, Caselli S, Paolo Di, Fernando M, Spataro A, Pelliccia A (2017) RV Remodeling in Olympic Athletes. JACC Cardiovasc Imaging 10:385–393. https://doi.org/10.1016/j.jcmg.2016.03.017
La Sanz-de GM, Rubies C, Batlle M, Bijnens BH, Mont L, Sitges M, Guasch E (2017) Severity of structural and functional right ventricular remodeling depends on training load in an experimental model of endurance exercise. Am J Physiol Heart Circ Physiol 313:H459–H468. https://doi.org/10.1152/ajpheart.00763.2016
Funding
This study was supported by Zhejiang Province Medical and Health Research Project (Grant Number 2022KY971).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study design and interpretation of the results. FG and HZ proposed the experimental design of the article. SH performed the statistical analysis and drafted the manuscript. HM performed data analysis. CY and PH were responsible for image acquisition. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interests
The authors have no relevant financial or non-financial interests to disclose.
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the Affiliated Hospital of Hangzhou Normal University.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent to publish
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hu, S., Zhang, H., Ma, H. et al. Assessment of right ventricular structure and systolic function in amateur marathon runners using three-dimensional speckle tracking echocardiography. Int J Cardiovasc Imaging 39, 1473–1482 (2023). https://doi.org/10.1007/s10554-023-02869-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-023-02869-z