
Abstract
Purpose
Pathological complete response (pCR) after neoadjuvant chemotherapy (NACT) for breast cancer predicts the risk of recurrence and increasingly may indicate the need for additional therapy postoperatively.
Methods
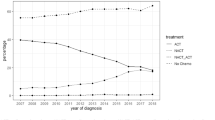
We identified non-metastatic breast cancer patients receiving NACT during 2013–2017. Patients’ and disease characteristics, rates of pCR (ypT0-is ypN0), toxicities, dose delays and reductions, and survival outcomes were recorded.
Results
789 patients had median age of 50 years. 67.8% had stage II disease, 71.1% had grade 3 , and 91.8% had ductal histopathology. 32.8% had estrogen receptor (ER)-positive/human epidermal growth factor receptor 2 (HER2)-negative, 25.5% had triple-negative (TN), and 38.0% HER2-positive disease. 6.8% received platinum. 48.2% of the HER2-positive patients received trastuzumab and pertuzumab and 51.8% received trastuzumab. Overall pCR rate was 33.5% and differed according to disease subtype, receptor status, grade, histology, and early discontinuation, but not according to age, dose reductions/delays, or year of treatment. The addition of pertuzumab to trastuzumab marginally improved the pCR rates. Survival outcomes were better following pCR.
Conclusions
In our analysis, pCR rates are consistent with the published data. Even with contemporary therapies, many patients have residual disease following NACT, suggesting a significant risk of recurrence, and may benefit from additional postoperative systemic therapy.


Similar content being viewed by others


Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Gralow JR, Burstein HJ, Wood W, Hortobagyi GN, Gianni L, von Minckwitz G et al (2008) Preoperative therapy in invasive breast cancer: pathologic assessment and systemic therapy issues in operable disease. J Clin Oncol 26(5):814–819
Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N et al (2014) Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet (London, England). 384(9938):164–172
Symmans WF, Wei C, Gould R, Yu X, Zhang Y, Liu M et al (2017) Long-term prognostic risk after neoadjuvant chemotherapy associated with residual cancer burden and breast cancer subtype. J Clin Oncol 35(10):1049–1060
Rastogi P, Anderson SJ, Bear HD, Geyer CE, Kahlenberg MS, Robidoux A et al (2008) Preoperative chemotherapy: updates of National Surgical Adjuvant Breast and Bowel Project Protocols B-18 and B-27. J Clin Oncol 26(5):778–785
Smith IC, Heys SD, Hutcheon AW, Miller ID, Payne S, Gilbert FJ et al (2002) Neoadjuvant chemotherapy in breast cancer: significantly enhanced response with docetaxel. J Clin Oncol 20(6):1456–1466
Untch M, Jackisch C, Schneeweiss A, Conrad B, Aktas B, Denkert C et al (2016) Nab-paclitaxel versus solvent-based paclitaxel in neoadjuvant chemotherapy for early breast cancer (GeparSepto-GBG 69): a randomised, phase 3 trial. Lancet Oncol 17(3):345–356
Loibl S, O’Shaughnessy J, Untch M, Sikov WM, Rugo HS, McKee MD et al (2018) Addition of the PARP inhibitor veliparib plus carboplatin or carboplatin alone to standard neoadjuvant chemotherapy in triple-negative breast cancer (BrighTNess): a randomised, phase 3 trial. Lancet Oncol 19(4):497–509
Sikov WM, Berry DA, Perou CM, Singh B, Cirrincione CT, Tolaney SM et al (2015) Impact of the addition of carboplatin and/or bevacizumab to neoadjuvant once-per-week paclitaxel followed by dose-dense doxorubicin and cyclophosphamide on pathologic complete response rates in stage II to III triple-negative breast cancer: CALGB 40603 (Alliance). J Clin Oncol 33(1):13–21
von Minckwitz G, Schneeweiss A, Loibl S, Salat C, Denkert C, Rezai M et al (2014) Neoadjuvant carboplatin in patients with triple-negative and HER2-positive early breast cancer (GeparSixto; GBG 66): a randomised phase 2 trial. Lancet Oncol 15(7):747–756
Gianni L, Pienkowski T, Im YH, Roman L, Tseng LM, Liu MC et al (2012) Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, phase 2 trial. Lancet Oncol 13(1):25–32
Gianni L, Pienkowski T, Im YH, Tseng LM, Liu MC, Lluch A et al (2016) 5-year analysis of neoadjuvant pertuzumab and trastuzumab in patients with locally advanced, inflammatory, or early-stage HER2-positive breast cancer (NeoSphere): a multicentre, open-label, phase 2 randomised trial. Lancet Oncol 17(6):791–800
Schneeweiss A, Chia S, Hickish T, Harvey V, Eniu A, Hegg R et al (2013) Pertuzumab plus trastuzumab in combination with standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer: a randomized phase II cardiac safety study (TRYPHAENA). Ann Oncol 24(9):2278–2284
Masuda N, Lee S-J, Ohtani S, Im Y-H, Lee E-S, Yokota I et al (2017) Adjuvant capecitabine for breast cancer after preoperative chemotherapy. N Engl J Med 376(22):2147–2159
von Minckwitz G, Huang C-S, Mano MS, Loibl S, Mamounas EP, Untch M et al (2019) Trastuzumab emtansine for residual invasive HER2-positive breast cancer. N Engl J Med 380(7):617–628
Hammond ME, Hayes DF, Dowsett M, Allred DC, Hagerty KL, Badve S et al (2010) American Society of Clinical Oncology/College Of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J Clin Oncol 28(16):2784–2795
Wolff AC, Hammond ME, Hicks DG, Dowsett M, McShane LM, Allison KH et al (2013) Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J Clin Oncol 31(31):3997–4013
Administration FaD (2007) Guidance for Industry Clinical Trial Endpoints for the Approval of Cancer Drugs and Biologics
Mieog JS, van der Hage JA, van de Velde CJ (2007) Preoperative chemotherapy for women with operable breast cancer. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD005002.pub2
Acknowledgements
The authors wish to acknowledge the support of The Royal Marsden NIHR Biomedical Research Centre for Cancer.
Funding
The authors have no funding to report.
Author information
Authors and Affiliations
Contributions
NMLB and AR conceived and designed the analysis. NMLB, VT, NaC, NeC, KL, SS, TSR, RJ collected the data. NMLB and KM performed the analysis. NMLB, AR, VT, NaC, NeC, KL, SS, TSR, RJ, NT, SM, MP, KM, MA, and SJ wrote the paper.
Corresponding author
Ethics declarations
Conflict of interest
Dr Battisti has received travel grants from Genomic Health and Pfizer and speaker fees from Pfizer. Dr Ring has received advisory board fees from Roche, Novartis, Pfizer, and Lilly; and speaker fees from Novartis and Pfizer. Prof Johnston has received consulting and advisory board fees from Eli Lilly, AstraZeneca, Puma Biotechnology Pfizer, and Novartis; and speaker fees from Pfizer, Novartis, and Eisai; and research funding from Pfizer and Puma Biotechnology. Prof Turner has received research funding from Merck Sharp & Dohme, Pfizer, AstraZeneca, Clovis, Roches, Tesaro, and Novartis. Dr Okines has received research funding from Pfizer and speaker fees from Roche. Dr McGrath has received travel grants from Genomic Health. Dr Parton, Dr Allen, Dr True, Dr Chaabouni, Dr Chopra, Dr Lee, Dr Shepherd, Dr Shapira-Rotenberg, Dr Joshi, and Mr Mohammed have no conflict of interest.
Ethical approval
This analysis was approved as a Service Evaluation by The Committee for Clinical Review of The Royal Marsden NHS Foundation Trust.
Informed consent
No individual person’s data are included in the manuscript in any form and therefore no consents for publication were required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Battisti, N.M.L., True, V., Chaabouni, N. et al. Pathological complete response to neoadjuvant systemic therapy in 789 early and locally advanced breast cancer patients: The Royal Marsden experience. Breast Cancer Res Treat 179, 101–111 (2020). https://doi.org/10.1007/s10549-019-05444-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-019-05444-0