
Abstract
To investigate the effect of psychosocial interventions on emotion regulation outcomes in children and youth (0–23 years). We conducted a meta-analysis using a three-level modeling approach extracting multiple effect-sizes from experimental and quasi-experimental studies. We included 40 interventions from 35 publications involving 3,891 participants and extracted 258 posttreatment effect sizes. Analyses were performed to assess intervention effects on emotion regulation, moderating effects of inclusion of acceptance focus and other potential moderators. Additionally, we examined intervention effects on mental health outcomes. Interventions showed a significant small-to-medium effect on emotion regulation (d = 0.37, 95% CI [0.22, 0.51], p < .001). Similar effects on were found regardless of acceptance-focus. Interventions significantly associated with a higher level of effect (p ≤ 0.045) included ACT, DBT, CBT and behavior parent training interventions. Significant small-to-medium effects were found for mental health outcomes (d = 0.39, 95% CI [0.25, 0.53], p < .001), with a correlation of .56 between overall outcomes across domains. Meta-regression results indicated that psychosocial interventions are moderately effective in improving emotion regulation, with no significant difference in inclusion of acceptance-focus. Findings suggest that emotion regulation is a transdiagnostic process that may inform the development of more beneficial interventions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
In recent years, emotion regulation has been theorized as a transdiagnostic construct that underlies the development and maintenance of diverse forms of psychopathology; consequently, emotion regulation has been framed as a central target of interventions for a range of clinical difficulties across children, adolescents, and adult populations (e.g., Aldao et al., 2016; Compas et al., 2017; Gratz et al., 2015). In this meta-analysis we test how effective psychosocial interventions are at improving child and adolescent emotion regulation outcomes.
Emotion regulation can be broadly defined as the capacity to manage one’s own emotional responses (Young et al., 2019), and more specifically, as goal-directed behaviors to control or modulate emotions, where both automatic and deliberate emotional processes are influenced by the use of strategies (Gross, 2015). Adaptive regulation is understood as context-dependent use of strategies to up-and down-regulate both positive and negative emotions (McRae & Gross, 2020). Expanding the conceptualization of emotion regulation with an clinical-contextual emphasis on the ability to experience a full range of emotional content, Gratz and Roemer (2004) included a focus on emotional awareness, understanding, and acceptance of emotional content, in addition to the ability to engage in goal directed behavior, refrain from impulsive behavior, and access effective regulatory strategies when needed. Thus, a hallmark of adaptive emotion regulation is successfully applying regulating strategies to respond flexibly to changes in one’s external and internal situational demands (Aldao et al., 2015). Conversely, the related concept of emotion dysregulation is reflected in generalized difficulties in these skills, resulting from a failure to regulate emotions when needed or choosing to implement poorly matched strategies (Gross, 2013). In the current review, emotion regulation will refer to abilities or skills in experiencing or modulating emotions, whereas emotion dysregulation will refer to aforementioned difficulties in these domains. Scholars have argued that emotion regulation is a core developmental aspect of human maturation (Cole et al., 2004) and is essential to the development of social competence, academic achievement, and psychological well-being (e.g., Eisenberg et al., 2010; Gross & Muñoz, 1995).
Emotion regulation strategies play a key role in mental health symptoms in both child and adult populations (Aldao et al., 2010; Bender et al., 2012; Nolen-Hoeksema et al., 2008), and has been examined in systematic reviews and meta-analyses (e.g., Aldao et al., 2010; Daros et al., 2021; Moltrecht et al., 2020; Schäfer et al., 2017; Sloan et al., 2017) and across psychopathology categories and comorbidities (McLaughlin et al., 2011, 2014). Different classifications (e.g., Aldao et al., 2010; Daros et al., 2021) distinguishes the strategies into 1) adaptive and/or engagement strategies, involving active engagement with an emotional experience, and 2) maladaptive and/or disengagement strategies, involving attempts to disengage from an emotional experience (see Table S1 in Supplementary materials for details). Adaptive emotion regulation strategies found to buffer against psychopathology include the engagement skills reappraisal, problem solving, and acceptance (Aldao et al., 2010). Conversely, maladaptive strategies linked to increases in overall mental health difficulties, include the disengagement regulation skills avoidance, suppression, and rumination (Aldao et al., 2010).
The use of emotion regulation strategies to modulate emotions has clear developmental shifts, starting from external parental regulation in early childhood, transitioning to a gradual increased reliance on more complex and flexible internal regulation strategies in adolescence and young adulthood (Compas et al., 2017; Weissman et al., 2019). Deficits in emotion regulation during these formative years are associated with a higher probability of developing anxiety and depressive symptoms and an overall risk of comorbid psychopathology (Young et al., 2019). Furthermore, the relation between childhood maltreatment and later psychopathology can in part be explained by increases in emotional reactivity and engagement in maladaptive emotion regulation strategies (Heleniak et al., 2016; Weissman et al., 2019). This aligns with research highlighting that individuals who, by disposition, are highly reactive to emotions, are also more vulnerable to developing a range of mental health problems (Carver et al., 2017; Caspi & Moffitt, 2018), Specifically, emotional dysregulation has been recognized in youth depression (Silk et al., 2003; Young et al., 2019), anxiety disorders (Schneider et al., 2018), deliberate self-harm (Wolff et al., 2019), the development of personality disorders (Matusiewicz et al., 2014), as well as broader internalizing and externalizing problems (Compas et al., 2017).
Emotion Regulation as a Transdiagnostic Target
There is seemingly a mismatch between the high instance of youth comorbidity and diagnostical complexity and the single-problem focus many existing treatment interventions employ (Weisz et al., 2017a, b). Therefore, an increased interest in transdiagnostic treatment approaches that focus on shared pathological processes has emerged (Barlow et al., 2013; Norton & Paulus, 2016), suggesting that targeting emotion regulation may lead to beneficial outcomes across mental health symptoms. A number of children and youth psychotherapies have incorporated treatment elements that explicitly teach emotion regulation skills. Nevertheless, different modalities focus on different skill sets; while traditional Cognitive Behavioral Therapy (CBT) interventions may emphasize elements of cognitive reappraisal and restructuring, ‘third wave’ psychotherapies have an added emphasis on acceptance-based skills (Young et al., 2019). ‘Third wave’ child and youth interventions include: Dialectical Behavior Therapy for children (DBT-C; Perepletchikova et al. 2017) and adolescents (DBT-A; Rathus & Miller, 2002), acceptance and commitment therapy for adolescents (ACT; Halliburton & Cooper, 2015; Hayes et al., 1999), and the unified protocol for youth (UP; Barlow et al., 2004; Ehrenreich-May et al., 2017). Such acceptance-focused approaches may be of special interest when examining the effects of emotion regulation interventions, as mindfulness and acceptance involve the non-judgmental acceptance of emotions, thoughts, and sensations as they are (Segal et al., 2018), and a willingness to experience troublesome thoughts and feelings without striving to alter, avoid, or control them (Biglan et al., 2008). Nevertheless, there is substantial variability among these interventions in terms of underlying principles and specific techniques employed. By way of illustration, DBT (Linehan, 1993) considers emotion dysregulation as a core dysfunction which is targeted through carefully balancing both acceptance-focused and cognitive behavioral techniques and skills delivered through multiple treatment modes such as skills training groups, individual sessions and telephone consultations. In contrast, ACT (Hayes et al., 1999) places a greater emphasis on aligning personal values and behavior through promoting psychological flexibility and acceptance of unwanted emotional or cognitive content. Interventions are more commonly delivered through individual sessions and do not incorporate a specific skills training component. Furthermore, while both treatments incorporates mindfulness-practices, ACT views guided mindfulness as one of several processes aimed at facilitating psychological flexibility, whereas DBT considers mindfulness a core component highlighted across skills modules (e.g. increasing awareness of emotions and behavioral tendencies to reduce impulsive behavior). Additionally, DBT includes specific acceptance-skills in the Emotion Regulation-module (Linehan, 2015b), such as the concept of “radical acceptance”, which teaches clients to accept emotions, thoughts, or circumstances regardless of their painful content (Linehan & Wilks, 2015a).
Despite the aforementioned differences between interventions, all include concepts such as mindfulness and acceptance which are viewed as antithetical to the aforementioned maladaptive strategies (Chambers et al., 2009), and therefore may address clients’ deficits in emotion regulation skills in a new way.
A recent systematic review has both included younger samples along with adult samples (Sloan et al., 2017), and two meta-analyses especially examined emotion regulation outcomes for children and adolescent populations (Daros et al., 2021; Moltrecht et al., 2020). However, none have included participants younger than 6 years, leaving the possible effects for the younger children unexplored. Furthermore, none have included an extended range of mental health difficulties such as externalizing symptoms or behavioral disorders, even though emotion regulation has also been applied to externalizing disorders (see Aldao et al., 2010; McLaughlin et al., 2014; Nolen-Hoeksema et al., 2008,). Additionally, thus far, none have explored multiple effects for both emotion regulation and mental health outcomes utilizing a three-level approach (Assink & Wibbelink, 2016) integrating all calculable effects sizes from multiple levels.
Review Aims
Although some aspects regarding the usefulness of psychosocial interventions for emotion regulation are known, several limitations in the literature should be addressed. Firstly, there is limited knowledge regarding the interventions’ effectiveness on emotion regulation treatment targets, especially for younger populations. Secondly, despite the purported intention behind acceptance-focused treatment elements, their specific effect is less explored. Therefore, efforts should be made to elucidate the effects in general, and of acceptance-focused treatment elements in particular, on children and youth emotion regulation outcomes. Also, one would assume that if emotion dysregulation is a transdiagnostic dimension of relevance across mental health disorders, then interventions addressing emotion dysregulation would also promote a decrease in related mental health symptoms.
We address these assumptions in the current meta-analysis by 1) examining whether psychosocial interventions for children and youth, regardless of whether they explicitly claim to target emotion regulation, improve emotion regulation outcomes, 2) exploring whether interventions that focus explicitly on acceptance-focused elements are more effective in improving emotion regulation, and 3) examining whether the interventions improve mental health outcomes for children and youths. Additionally, given a substantial amount of heterogeneity in the estimated effects, we 4) explore candidate moderators based on prior meta-analyses (e.g., De Los Reyes et al., 2015; Moltrecht et al., 2020; Schäfer et al., 2017; Weisz et al., 2017b) including participants’ age and gender, outcome measures type, intervention type, informant type, active vs. passive control condition, and incomplete outcome data bias.
Method
Publications were included if they had outcome measures for both emotion regulation and mental health. We included both experimental and quasi-experimental studies, to cover as much of the literature as possible. In line with the exploratory aim of this study, we included both interventions with and without an explicit focus on emotion regulation, because if emotion regulation is a transdiagnostic factor, we would expect effects in both emotion regulation and related mental health domains regardless of intervention focus. Following from Sloan et al.’s (2017) meta-analysis, we acknowledged the multi-faceted nature of emotion regulation and chose to use an emotion regulation definition which includes the awareness and understanding of emotions (Gratz & Roemer, 2004), in addition to the adaptive and maladaptive emotion regulation strategies, as described by Aldao et al. (2010). Additionally, we based our understanding of emotion regulation measures on Adrian et al. (2011) review of emotion regulation measures, as well as the aforementioned reviews (Aldao et al., 2010; Sloan et al., 2017). This means we included measures of emotion regulation as a) dysregulation (e.g., affect lability) or maladaptive use of strategies (e.g., rumination, worry), and b) an ability for emotional awareness and understanding (e.g. emotion observation) and use of adaptive strategies, including acceptance or mindfulness concepts. We followed PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines for conducting and reporting this study (Page et al., 2021). In addition, we developed and registered a review protocol in PROSPERO prior to our search following the procedures outlined in the Cochrane Handbook for Systematic Reviews (Higgins et al., 2023).
Inclusion and Exclusion Criteria
We screened for eligible studies in our search results, and identified relevant studies in other reviews based on the following inclusion criteria:
-
a)
Population: children and youths (0–23 years mean age) with either clinical levels (i.e., either meeting the criteria of the Diagnostic Statistical Manual of Mental Disorders (APA, 2022), or subclinical symptoms (i.e., defined as indicative of treatment in the present study) of mental health problems. The decision to set the upper mean age cut-off was informed by the United Nations Department of Economic and Social Affairs (2018) definition of youth, which encompasses individuals between the ages of 15 and 24.
-
b)
Interventions: psychosocial interventions intended to address psychological symptoms and/or diagnoses. As noted, although our search aimed at emotion regulation interventions, we included studies with or without an explicit focus on emotion regulation, if they included both emotion regulation and mental health outcomes. We searched for references in which emotion regulation terms were specifically mentioned in the title, abstract and/or controlled vocabulary.
-
c)
Comparison: all active or passive control or comparison conditions in experimental and quasi-experimental studies, including treatment as usual (TAU) or other active comparators.
-
d)
Outcomes: at least one measure of emotion regulation (e.g. Difficulties in Emotion Regulation Scale, DERS), and one symptom measure related to mental health disorders (e.g. Child Behavior Checklist, CBCL). We included self, parental, teacher, and clinician reported outcomes, as well as task-based scores.
We excluded studies that:
-
a)
Included special populations (e.g. autism spectrum disorder, intellectual impairment, psychosis).
-
b)
Lacked a control or comparison group.
-
c)
Included pharmacological treatment only.
We did not exclude studies based on language or publication status.
Information Sources
A comprehensive literature search was conducted in PsycINFO (Ovid, 1806 – to Present), Medline (Ovid, 1946 – to Present), and the Cochrane Library (start date not specified). The search strategies included both controlled vocabulary and free-text terms related to psychopathology, emotion regulation, and relevant interventions, and were adapted to each database (see Supplemental Materials).
All references were downloaded to the Covidence systematic review software (Covidence Software, Veritas Health Innovation, Melbourne, Australia, available at www.covidence.org) for pairwise abstract and full-text screening, and Risk of Bias (RoB) assessments. The review team screened abstracts and full-texts independently, and when the reviewers were uncertain about an article's eligibility, the full report was obtained, and discrepancies were discussed. If consensus was not reached, authors KE and KR consulted the wider team.
Study Selection
To ensure that the intervention and control conditions were distinct, we excluded three studies (Bass & Apsche, 2013; Talley, 2013; Suveg et al., 2018) with control interventions that overlapped with treatment conditions in the other included studies. We are aware of the potential overlap between emotion regulation measures and measures assessing psychopathological symptoms, as well as concerns around emotion regulation measures psychometric properties (Mazefsky et al., 2021). We address these challenges in the discussion.
Data Extraction
After screening for eligibility, study characteristics such as sample size, age, gender, and control and treatment conditions were entered into a data extraction form by two independent reviewers. All data extraction and RoB assessments, including the incomplete outcome data bias rating, were performed in collaboration with Helland et al. (2022). Five of the authors, in addition to two graduate-students identified relevant abstracts in initial searches. The first author reviewed all abstracts included from the search. No indicators of agreement were tracked. Where there was a disagreement regarding the inclusion of a study, the two researchers reviewed the article and discussed its eligibility until an agreement was achieved. Data extraction and Risk of Bias analyses was done independently by two researchers, along with two graduate students trained in meta‐analytic methodology who also coded each study. All data was manually reviewed by the first author and one additional author to check for data entry errors. No indicators of intercoder reliability or agreement were tracked.
The primary moderator examined was the inclusion of an acceptance or mindfulness component (yes or no), as defined by the intervention features readily available in the primary articles. Interventions were classified as acceptance/non-acceptance focused based on whether they included treatment elements related to acceptance and/or mindfulness. Examples include explicit mindfulness practices (e.g., MBCT-C, Unified Protocol and Rumination-focused CBTs inclusion of mindfulness skills to increase present-moment awareness), in addition to other acceptance-focused elements (e.g. ACT and DBT focus on increased acceptance of emotions and thoughts). We additionally explored several other moderating effect variables. Moderating variables were clustered into intervention, study, outcome, and sample characteristics, and all studies were coded by twelve intervention characteristics (see Tables 1, 2, 3, 4) and distinctions were made between a range of described treatment approaches (e.g. CBT, ACT) to illuminate possible moderating effects related to type of intervention. Variables regarding study characteristics were coded by type of control condition and informant, as well as incomplete outcome data bias score from Risk of Bias assessments, as attrition rates may introduce bias if drop-out participants characteristics are different than those remaining. We coded all variations of treatment as usual (e.g. TAU, enhanced TAU) and other treatment interventions as active conditions, and all types of waitlist conditions (e.g. waiting list, assessment only) as passive. We coded informants as either self-report, parental report, clinician report, or other (e.g. teacher/external observer). Regarding outcome measures, all were coded as follows: emotion regulation, externalizing difficulties, internalizing difficulties, other symptom measures (e.g., CGI-S Clinical Global Severity) and general mental health (e.g., Q-LES-Q Quality of life enjoyment and satisfaction questionnaire). Furthermore, all measures except emotion regulation measures were grouped together as a collective outcome category termed ‘mental-health measures.’
Methods for Assessing Internal Validity Risk
Risk of Bias in this review was assessed independently by the authors and research assistants. A third senior researcher was consulted when there was a lack of consensus. For randomized controlled trials (RCTs), the Cochrane Collaboration’s Risk of Bias Tool was utilized; for quasi-experimental designs, we used the Cochrane Effective Practice and Organization of Practice (EPOC) Risk of Bias Tool. Risk of Bias for each domain was rated as high (seriously weakens confidence in the effect estimate), low (unlikely to seriously alter the effect estimate), or unclear.
Effect Measures
We specified the effect measure as Cohen’s d for differences between intervention and control conditions posttreatment. This measure presupposes that the number of participants together with means and standard deviations in the intervention and control conditions were available posttreatment; only these studies were included in subsequent analyses. The variance of Cohen’s d was estimated by formula 3 in Marfo and Okyere (2019). To ensure that a positive effect measure signified that the intervention was more favorable than the control condition, the Cohen’s d sign was flipped if the outcome measure was in the opposite direction.
Statistical Analysis
As a preparatory analysis, the cases with the information necessary for computing Cohen’s d (n = 258) were compared with cases where this information was not available (n = 46). The dependent variable in these analyses was whether this information and relations with the variables were available for the whole data set, and were investigated by logistic regressions using generalized estimating equations (gee) to take clustering within studies into account. Wherever necessary information was unavailable, we used alternative summary statistics to calculate Cohen’s d values (e.g. p values and sample sizes, or t-test statistics).
Since there were multiple effects within studies, the data were analyzed by the three-level procedure implemented in the function rma.mv in the R package metafor (A Meta-Analysis Package for R; Viechtbauer, 2010), following the detailed procedure described in Assink and Wibbelink (2016). Separate effect estimates for emotion regulation and mental health outcomes were computed through a moderator analysis where the different types of outcomes were used as a dichotomous moderator, together with a test for heterogeneity. Three levels of random variation were included: between studies, between effects within studies, and between participants for each effect measure. The last, innermost, level was represented by the variance measures of Cohen’s d for each effect. Standard deviations for random variation between and within studies were also estimated, together with percentages of random variation in each of the three levels (Cheung, 2014). For each categorical moderator, an overall effect for each category was estimated together with differences in effects between categories. For continuous moderators, an effect for a chosen reference value and a slope was calculated. A test of residual heterogeneity was also included. We additionally included an overall Wald Test for each multi-category categorical moderator. The following moderators were included in the analyses: acceptance-focus, outcome measures, intervention type, informant type, control condition type, participants’ age and gender, and the incomplete outcome data bias score. We additionally investigated whether interventions are more likely to yield stronger effects on mental health when they yield stronger effects on emotion regulation. To this end, we estimated the correlation between overall effect sizes for mental health and emotion regulation, based on estimated variances and covariances between the overall effect sizes.
Logistic regressions for whether information necessary to compute Cohen’s d was available, were performed used the R (The R Foundation for Statistical Computing, Vienna, Austria) package gee (Vincent J. Carey, Ported to R by Thomas Lumley, Brian Ripley). For main analyses, a shiny app (Chang et al., 2020) was developed for the procedure described by Assink and Wibbelink (2016). R code for the shiny app is available in the GitHub repository: (Edited for anonymity).
Additionally, we included in the app Marengo and Montag’s (2020) approach for detecting possible publication bias in a three-level model through examining 1) the funnel plot illustrating the correlations between all observed and predicted scores in each study plotted against their standard error and 2) the significance of a modified Egger’s Regression Test (Egger et al., 1997; Marengo & Montag, 2020) computed by including the standard error as a predictor of effect sizes. Thus, the modified Egger’s Regression Test provides an assessment of the asymmetry of the funnel plot and gives an indication of publication bias if less precise studies show higher effect sizes than more precise studies.
Results
Study Selection
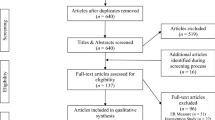
The PRISMA flow diagram is shown in Fig. 1. An initial literature search was carried out July 6, 2018 and updated May 8, 2020. The two searches produced a total of 1,355 references, where 105 duplicates were removed. Following title and abstract screening, 163 full-text papers were retrieved for further considerations. The first author manually examined all identified review articles for relevant studies, and an additional seven full-text articles were added to full-text screening. After examining the full-texts, 129 articles were excluded. After author correspondence, all included studies provided the data necessary for estimating the effect and variance measures.

PRISMA flow chart
Study, Sample, and Intervention Characteristics
In total, 40 interventions from 35 separate publications (N = 3,891 participants) and 258 effect-sizes, whereas 102 reported on emotion regulation outcomes, were included in the final meta-analysis. Included study characteristics were: author(s), publication year, study design, age (mean and range), gender composition, intervention and control condition, emotion regulation or mental health measure, and the Incomplete outcome data Bias Assessment.
The coded articles were published from 2002 to 2020. The majority of the primary studies included participants between 3 and 23 years old (M = 15.5 years), though three studies included some participants older than 25 (Olson, 2018; Lee et al., 2020; Whiteside, 2010). In all studies the sample mean age was below 23 years. Sample sizes ranged from 19 to 436 participants. Thirty-one studies (88%) were conducted using an RCT design, one of the RCTs also implemented a mixed randomized-quasi-randomized design, two studies had a quasi-randomized design, and two other studies were non-randomized controlled trials. For studies with multiple treatment conditions where both treatment conditions were assumed to address emotion regulation, both groups were coded and included in the analysis. Twenty studies (56%) used an active control design (i.e. TAU); 15 studies (44%) used a passive control design (i.e. waitlist control). The most commonly employed interventions were variations of CBT (n = 8; 24%). Thirty studies included both genders in the treatment samples (82%), four studies included only girls, and one study included only boys.
Risk of Bias Assessment Within and Across Studies
Figures 2 and 3 illustrate the overall risk of bias within and across studies. All 43 interventions evaluations fulfilling the search criteria were assessed, including interventions with control conditions that overlapped with treatment conditions in the other included interventions. Allocation concealment was not sufficiently described in three studies (Cotton et al., 2020; Idsoe et al., 2019; Wineman, 2009), 26 studies were unclear, and the remaining 12 studies were deemed as low risk of bias. Two studies did not report on sequence generation (Cotton et al., 2020; Wineman, 2009), 19 studies had an unclear sequence generation, and the remaining 20 studies were deemed as low risk of bias. Only two studies (Whiteside, 2011; Yang et al., 2016) reported blinding of participants and personnel, 10 studies were deemed as high risk, and the remaining 29 studies unclear risk of bias. Nineteen studies reported that the outcome assessor was blinded, three studies were high (Idsoe et al., 2019; Wilkinson & Goodyer, 2008; Cotton et al., 2020), and 19 studies were unclear risk of bias. As for the incomplete outcome assessment, only three studies (Bentley et al., 2017; Payne, 2019; Schuppert et al., 2009) were assessed as high risk due to a high dropout-rate and missing data; 19 studies were assessed as low, and 18 as unclear risk of bias. Selective outcome reporting of outcome measures was detected in only one study (Payne, 2009), three studies were unclear, and 37 were assessed as low risk of bias. No high risks in other sources of bias were detected.

Risk of bias assessment within studies

Risk of bias assessment across studies
A summation of the overall risk of bias across studies (Fig. 3) shows that the majority of information came from trials with low or unclear risk of bias. An exception was the blinding of participants and personnel where a higher proportion of information (about 20%) was assessed as high risk of bias.
Synthesis Results
There was significant heterogeneity (Q = 1201.588, df = 257, p < 0.001) among the overall effect sizes in the full dataset when we compared study interventions with any control condition. Furthermore, the Likelihood Ratio Test, where we distinguished between 258 unique effect sizes (level 2) clustered in 40 interventions in 35 studies (level 3), showed that significant variance was present at both the within (level 2: SE = 0.42, p < 0.001) and between study level (level 3: SE = 0.30, p < 0.001). This suggest that there is room for within-and between-study characteristics that may impact on the overall effect.
Meta-Analysis
Emotion Regulation
We examined the intervention effect on emotion regulation outcomes (nemotion regulation = 102, see Table 2) through a moderation analysis with a dichotomous moderator for emotion regulation versus mental health outcomes, and found a significant posttreatment effect size of Cohen’s d = 0.37, 95% CI [0.22, 0.51], p < 0.001 which suggests that the interventions improve emotion regulation when compared to control conditions. The test for heterogeneity on the dataset including only emotion regulation outcomes revealed a reduced, but still significant value (Q = 301.232, df = 101, p < 0.001), with significant variance between studies (level 3: SE = 0.33, p < 0.001), but not at the within study level (level 2: SE = 0.15, p < 0.001).
Emotion Regulation and Acceptance-Focused Interventions
We furthermore used the reduced dataset with only the emotion regulation effects sizes to examine whether acceptance-focused interventions were more effective in improving emotion regulation than non-acceptance focused interventions (nacceptance = 44; nnon-acceptance = 58). Cohen’s d for acceptance-focused interventions was d = 0.39, 95% CI [0.20, 0.58], p < 0.001, and for non-acceptance focused a Cohen’s d = 0.33, 95% CI [0.16, 0.50], p < 0.001, which gives an estimated difference in Cohen’s d for non-acceptance versus acceptance focused interventions of -0.06 95% CI [-0.30, 0.18], p = 0.621. The result is consistent with an effect on emotion regulation outcomes of similar magnitude regardless of acceptance-focus.
Mental Health
Furthermore, we examined intervention effects on the collective mental health domain (nmental health = 156) through a moderation analysis with a dichotomous moderator for emotion regulation versus mental health outcomes and found a significant effect size of Cohen’s d = 0.39, 95% CI [0.25, 0.53], p < 0.001, suggesting an intervention effect on mental health symptoms of similar magnitude to the effect on emotion regulation. Indeed, the estimated difference for mental health versus emotion regulation measures when examining the overall dataset was negligible with a Cohen’s d difference of 0.022, 95% CI [-0.11, 0.16], p = 0.746. We additionally examined the intervention effects for the specific types of outcome measures, and found significant effects which were slightly higher for externalizing difficulties (d = 0.56, 95% CI [0.26, 0.87], p < 0.001) and general mental health measures (d = 0.50, 95% CI [0.22, 0.79], p < 0.001), than for internalizing difficulties (d = 0.34, 95% CI [0.18, 0.50], p < 0.001) and other symptom measures (d = 0.39, 95% CI [0.16, 0.61], p < 0.001). These results may suggest that intervention effects are stronger for externalizing and general mental health outcomes, and to a lesser extent, internalizing symptoms.
Correlations between Emotion Regulation and Mental Health
We used all eligible studies with emotion regulation and mental health outcomes (32 studies; nemotion regulation = 98, nmental health = 156) to investigate whether interventions are more likely to yield stronger effects on mental health when they yield stronger effects on emotion regulation. We found that a correlation of 0.56, indicating that a high overall effect of emotion regulation is related to a high overall effect in mental health.
Other Moderator Analyses
As there was a substantial amount of heterogeneity in the estimated effect sizes, analyses were performed to identify the potential impact of prespecified moderators on emotion regulation outcomes. Results are presented in Table 4.
We examined the moderators of sample, study and intervention effect. Findings indicated that the following moderators were significantly associated with a higher level of effect on emotion regulation posttreatment (p ≤ 0.045): ACT, DBT, CBT and behavior parent training interventions, youth or parent informant, active and passive control condition, samples including both genders, and low and unclear risk of incomplete outcome data bias. Other intervention types (i.e. rumination focused, psychodynamic, cognitive training), samples restricted to either boys or girls, and high risk of incomplete outcome data bias were not significant associated with higher levels of effect on emotion regulation posttreatment (p ≥ 0.444). All moderators showed a residual heterogeneity with p < 0.001, indicating heterogeneity in the data even after taking each moderator into account.
Publication Bias
The investigation of publication bias was completed via funnel plot visualization (see Fig. 4) and a modified Egger’s Test (Egger et al., 1997; Marengo & Montag, 2020). The distribution of effect sizes was mostly symmetrical with only a few effects sizes in the outer range, which suggests no substantial publication bias. However, the modified Egger’s Test pointed to a significant positive relationship of the effect size with the standard error (B = 3.82, 95% CI [2.67, 4.97], p < 0.001). An additional sensitivity analysis was conducted where two parental report measure effects from Webster-Stratton et al. (2011) were excluded. This analysis demonstrated a high p value (p = 0.182), indicating that these two effects substantially contributed to the perceived publication bias.

Publication bias funnel plot
Discussion
This comprehensive systematic review and three-level meta-analysis examined the effectiveness of psychosocial interventions on emotion regulation outcomes among children and youth. In line with the existing literature (Daros et al., 2021; Moltrecht et al., 2020; Sloan et al., 2017), we found a significant small-to-medium effect size on child and youth emotion regulation (d = 0.37). Combined with previous findings showing that targeting emotion regulation processes in treatment produces beneficial outcomes across mental health difficulties (e.g., Linehan, 1993; Hayes et al., 1999; Barlow et al., 2010), the findings supports the notion that emotion regulation is an underlying transdiagnostic process. Furthermore, with the advancing addition of acceptance and mindfulness treatment elements in ‘third-wave interventions’ to enhance treatment effects (Chambers et al., 2009), we examined whether this was reflected in different moderating effects on emotion regulation. We found a significant small-to-medium effect size regardless of acceptance-focus (d = 0.33 and 0.39), with no significant difference between them. One possible interpretation could be that interventions derived from more traditional models without an explicit focus on acceptance may also effectively address emotion regulation, albeit with a difference in semantics, as they may explicitly aim to reduce the use of maladaptive strategies (Chambers et al., 2009). If so, this may in part explain the lack of significant effect differences between acceptance-focused and other interventions included in the current review.
Furthermore, since emotion regulation processes cut across symptom categories, and are considered a predictor of various forms of psychopathology (e.g., McLaughlin et al., 2011) we expected to see this reflected in concomitant improvement in mental health outcomes (see Aldao et al., 2016). We found a significant small-to-medium overall effect size indicating that the interventions effectively improved mental health outcomes (d = 0.39). Although the similarity of the emotion regulation and the mental health estimates could be interpreted as questioning whether these constructs are truly different, we would argue that the confidence interval for this difference (CI [-0.11, 0.16]), indicate that a substantial difference cannot be excluded either. Additionally, similar to previous studies (Moltrecht et al., 2020) we found a strong correlation between high overall effects of emotion regulation and high overall effects in mental health. Following from the literature on regulation difficulties as a predictor for a wide range of psychopathology (e.g., McLaughlin et al., 2014; Young et al., 2019), we suggest that due to its transdiagnostic nature, emotion regulation is potentially a more proximal outcome than mental health (Aldao et al., 2016). Thus, interventions would be expected to produce recognizable effects across outcome domains.
Conceptual and Clinical Implications
This review has several conceptual and clinical implications. While emotion regulation processes in child and youth samples have been previously examined (Sloan et al., 2010; Moltrecht et al., 2020; Daros et al., 2021), this review fills an important literature gap by reporting on multiple posttreatment effects for emotion regulation, as well as on a broader range of mental health symptoms, and including younger samples (under 6 years old). Although there are similarities between the current review and existing literature, there is limited overlap in of included studies across the three meta-analyses (31.43% overlap with Daros et al., 2021; 11.43% overlap with Moltrecht et al., 2020; 19.05% overlap between Daros et al., 2021 and Moltrecht et al., 2020). One single study (Jacobs et al., 2021) was included in all three meta-analyses. This may be a reflection of minor disparities in specific search criteria and inclusion criteria employed in the respective studies. The search criteria for the current review requested that emotion regulation terms were explicitly included in the title, abstract and/or controlled vocabulary, thus somewhat limiting the scope of the search (1257 studies). Daros et al. (2021) conducted a two-part, broader search, resulting in the inclusion of 88 studies and 385 effect sizes, which is a substantial number. Conversely, but similarly to the current review, Moltrecht et al. (2020) based the search on criteria outlined in Sloan et al., (2017), resulting in a more limited number of studies (21). Moreover, it is noteworthy that the inclusion criteria of Daros et al. (2021) focused on youth and young adults (14–24 years), whereas Moltrecht et al. (2020) included child populations (6–23 years) but excluded younger populations (0–6 years) which diverges from our study. Additionally, similar to our review, Daros et al. (2021) included subclinical populations, while Moltrecht et al. (2020) used diagnostic criteria and symptoms which may have limited their search results. Furthermore, we would argue that the conceptualization of emotion regulation and dysregulation exhibits sufficient similarities, thus the current review did not distinguish between emotion regulation and dysregulation measures in our analyses.
As the aforementioned reviews, we argue that this meta-analysis supports the notion of emotion regulation as a transdiagnostic treatment construct. This is partly due to our finding that interventions had a positive effect on not just emotion regulation, but also mental health outcomes, indicating that changes occur in both constructs following treatment. Additionally, the interventions found in our search that did not explicitly include acceptance-based strategies (e.g., CBT, behavioral parent training), but still utilized emotion regulation outcome measures, also reported beneficial outcomes. Moving forward, research should further examine correlations between changes in emotion regulation and mental health outcomes, and whether emotion regulation mediates effects on mental health outcomes (Heleniak et al., 2016; Weissman et al., 2019). This may be especially crucial for comorbid populations, as further intervention development and refinement may provide improvement across symptoms. To date, this has been minimally explored and research is too scarce to provide clarity (see Moltrecht et al., 2020).
While this study could not ascertain whether or not an explicit focus on acceptance yielded different effects, it is noteworthy that the state of research pertaining to interventions for children and youths is still in its infancy. Currently, there is a dearth of knowledge regarding which treatment elements are most effective, or the appropriate developmental stages for their implementation. Notably, moderator analyses suggested that certain “third wave” interventions such as ACT and DBT were associated with a high level of effect on emotion regulation outcomes, which may imply that they contain elements especially relevant for emotion regulation targets.. Moving forward, the further integration of carefully selected effective elements from traditional CBT-interventions (e.g. cognitive reappraisal) and ‘third wave’ acceptance-focused elements (e.g. radical acceptance) might result in more effective interventions.
Limitations
Our limitations naturally reflect dilemmas associated with the meta-analytic process (e.g. creating comparison groups by collapsing categories), and the broad range of interventions and outcomes in our included studies. This calls for caution when interpreting our results. Firstly, our estimates and inferences are limited by the studies sampled, despite our three-level approach that enabled the inclusion of multiple outcomes, which would have otherwise been discarded using traditional meta-analytic procedures. Still, the results were based on a relatively limited number of studies because of the scarcity of existing research that has included measures addressing both emotion regulation and mental health difficulties for younger populations. Additionally, limitations related to our search strategy could have affected the number of identified relevant studies. Given the vast array of potential search terms that could have been included, the decision to adhere to a focused search strategy may have resulted in the omission of relevant literature, thereby impacting the comprehensiveness of our review. Further exploration into a wider selection of search terms, such as those aimed at infant or young child populations (e.g., temperament), or expanding the scope to more explicitly encompass constructs such as emotion lability and understanding of emotions could have enhanced the inclusivity of our study and provided a more comprehensive understanding of the research landscape. Regarding study samples, although studies with small sample sizes are fairly common in meta-analyses, more restricted samples can lead to more uncertainty in result interpretation. Overall, this highlights the need for more robust study designs with larger samples.
Furthermore, despite the advantages of close collaboration in this study, the lack of a standardized coding framework may have resulted in variability in how coders interpreted and categorized intervention characteristics, particularly in distinguishing between acceptance and non-acceptance interventions. This variability could potentially raise concerns regarding the reliability and validity of the study's findings, for example the lack of significant effect differences between acceptance-focused and other interventions.
An additional central limitation lies in the diversity of terminologies employed for the emotion regulation construct. Consequently, research has found varying psychometric properties of emotion regulation measures (Mazefsky et al., 2021), implying discrepancies in what underlying concept is being measured. An additional limitation stems from the potential overlap between assessment measure items for emotion regulation strategies and psychopathology, especially since affective facets may be captured in both constructs (Aldao et al., 2010). Even though some relations between emotion regulation strategies and specific psychopathology (e.g. between rumination and depression; Nolen-Hoeksema et al., 2008) have been investigated, further research should continue to explore potential confounding relations.
Lastly, the Risk of bias assessments suggest that, although the number of included studies characterized by high risk of bias was small, a great proportion were associated with unclear risk of bias partly due to poor reporting. In our study, the risk of bias in domains such as incomplete outcome data and sequence generation was considerable. Additionally, it is important to acknowledge the lack of inter-rater reliability coefficients for included moderators, which serves as a significant limitation when interpreting the findings.
Suggestions for Future Research
It is essential that future effectiveness studies include emotion regulation outcome measures, so research can further explore how emotion regulation is related to mental health difficulties, both in studies of traditional CBT-interventions and especially in ‘third wave’ interventions that claim to target emotion regulation. Furthermore, as Sloan et al. (2017) highlights, it is not clear whether interventions that improve emotion regulation simultaneously produce reductions in numerous comorbid symptoms as too few effectiveness studies have examined outcome measures for multiple psychological disorders. Future research should include controlled study designs with various diagnostic groups where changes in emotion regulation and mental health are examined across time points during treatment to more precisely define when changes occur. In summation, the transdiagnostic quality and mediating capabilities of emotion regulation is still to be determined (Aldao et al., 2016).
Furthermore, we argue that emotion regulation lacks conceptual clarity, reflected in the need for refinement of the vast array of measures used to examine emotion regulation in younger populations (Adrian et al., 2011) as wells as concerns of the psychometrics properties of emotion regulation measures (Mazefsky et al., 2021). Future research should allow for a more precise differentiation between emotion regulation aspects, as well as a discernment of related emotion regulation and psychopathology constructs.
To our knowledge, an overarching protocol on how to effectively target emotion regulation during treatment does not yet exist; therefore, each treatment element’s effectiveness across age groups, clinical populations and treatment criteria is still undetermined. In extension, more knowledge is needed regarding how elements work for different age groups, especially considering the developmental shifts that occur in managing emotional responses and using concrete emotion regulation strategies (Adrian et al., 2011). This calls for future research that utilizes experimental designs to identify change processes that assess the effects of explicit treatment elements on specific outcomes, as well as its optimal dosage. Through dismantling trials, along with factorial or time series experiments, it may be possible to identify the active elements in existing treatment protocols. This knowledge may be helpful in optimizing existing interventions and tailoring individual treatment courses based on the optimal combination and dosage of effective elements.
Conclusion
We extend the emotion regulation and psychopathology literature by providing, to our knowledge, the first three-level meta-analysis that reports psychosocial interventions to have meaningful effects on emotion regulation and mental health outcomes in children and youths. Our findings additionally expand on previous meta-analyses and existing literature (e.g. Daros et al., 2021; Moltrecht et al., 2020; Sloan et al., 2017), by including younger participants and examining outcomes in a broader range of mental health difficulties. Although research is expanding our understanding on the role of emotional processes across psychopathology, there is still an essential need to improve clinical care for children and their families. More research on emotion regulation as a transdiagnostic process may help optimize future interventions.
Data Availability
A semicolon-separated csv file for the data on which the three-level analyses were based is available on GitHub: https://github.com/ToreWentzel-Larsen/threelevel.
References
Adrian, M., Zeman, J., & Veits, G. (2011). Methodological implications of the affect revolution: A 35-year review of emotion regulation assessment in children. Journal of Experimental Child Psychology, 110(2), 171–197. https://doi.org/10.1016/j.jecp.2011.03.009
Aldao, A., Gee, D. G., De Los Reyes, A., & Seager, I. (2016). Emotion regulation as a transdiagnostic factor in the development of internalizing and externalizing psychopathology: Current and future directions. Dev Psychopathol, 28(4pt1), 927–946. https://doi.org/10.1017/s0954579416000638
Aldao, A., Nolen-Hoeksema, S., & Schweizer, S. (2010). Emotion-regulation strategies across psychopathology: A meta-analytic review. Clinical Psychology Review, 30(2), 217–237. https://doi.org/10.1016/j.cpr.2009.11.004
Aldao, A., Sheppes, G., & Gross, J. J. (2015). Emotion regulation flexibility. Cognitive Therapy and Research, 39(3), 263–278. https://doi.org/10.1007/s10608-014-9662-4
American Psychological Association. (2022). Diagnostic and statistical manual of mental disorders In (5th ed., text rev.). American Psychiatric Publishing. https://doi.org/10.1176/appi.books.9780890425787
Assink, M., & Wibbelink, C. (2016). Fitting three-level meta-analytic models in R: A step-by-step tutorial. The Quantitative Methods for Psychology, 12. https://doi.org/10.20982/tqmp.12.3.p154
Barlow, D. H., Allen, L. B., & Choate, M. L. (2004). Toward a unified treatment for emotional disorders. Behavior Therapy, 35(2), 205–230. https://doi.org/10.1016/S0005-7894(04)80036-4
Barlow, D. H., Bullis, J. R., Comer, J. S., & Ametaj, A. A. (2013). Evidence-based psychological treatments: An update and a way forward. Annual Review of Clinical Psychology, 9, 1–27. https://doi.org/10.1146/annurev-clinpsy-050212-185629
Bender, P. K., Reinholdt-Dunne, M. L., Esbjørn, B. H., & Pons, F. (2012). Emotion dysregulation and anxiety in children and adolescents: Gender differences. Personality and Individual Differences, 53(3), 284–288. https://doi.org/10.1016/j.paid.2012.03.027
Biglan, A., Hayes, S. C., & Pistorello, J. (2008). Acceptance and commitment: Implications for prevention science. Prevention Science, 9(3), 139–152. https://doi.org/10.1007/s11121-008-0099-4
Carver, C. S., Johnson, S. L., & Timpano, K. R. (2017). Toward a functional view of the p factor in psychopathology. Clinical Psychological Science, 5(5), 880–889. https://doi.org/10.1177/2167702617710037
Caspi, A., & Moffitt, T. E. (2018). All for one and one for all: Mental disorders in one dimension. American Journal of Psychiatry, 175(9), 831–844. https://doi.org/10.1176/appi.ajp.2018.17121383
Chambers, R., Gullone, E., & Allen, N. B. (2009). Mindful emotion regulation: An integrative review. Clinical Psychology Review, 29(6), 560–572. https://doi.org/10.1016/j.cpr.2009.06.005
Chang, W., Cheng, J., Allaire, J., Xie, Y., & McPherson, J. (2020). Package ‘shiny’: Web application framework for R. R Foundation for Statistical Computing, 238.
Cheung, M. W. L. (2014). Modeling dependent effect sizes with three-level meta-analyses: A structural equation modeling approach. Psychological Methods, 19(2), 211–229. https://doi.org/10.1037/a0032968
Cole, P., Martiin, S., & Dennis, T. (2004). Emotion regulation as a scientific construct: Methodological challenges and directions for child development research. Child Development, 75, 317–333. https://doi.org/10.1111/j.1467-8624.2004.00673.x
Compas, B. E., Jaser, S. S., Bettis, A. H., Watson, K. H., Gruhn, M. A., Dunbar, J. P., . . . Thigpen, J. C. (2017). Coping, emotion regulation, and psychopathology in childhood and adolescence: A meta-analysis and narrative review. Psychological Bulletin, 143(9), 939–991. https://doi.org/10.1037/bul0000110
Daros, A. R., Haefner, S. A., Asadi, S., Kazi, S., Rodak, T., & Quilty, L. C. (2021). A meta-analysis of emotional regulation outcomes in psychological interventions for youth with depression and anxiety. Nature Human Behaviour, 5(10), 1443–1457. https://doi.org/10.1038/s41562-021-01191-9
De Los Reyes, A., Augenstein, T. M., Wang, M., Thomas, S. A., Drabick, D. A. G., Burgers, D. E., & Rabinowitz, J. (2015). The validity of the multi-informant approach to assessing child and adolescent mental health. Psychological Bulletin, 141(4), 858–900. https://doi.org/10.1037/a0038498
Egger, M., Smith, G. D., Schneider, M., & Minder, C. (1997). Bias in meta-analysis detected by a simple, graphical test. BMJ, 315(7109), 629–634.
Ehrenreich-May, J., Rosenfield, D., Queen, A. H., Kennedy, S. M., Remmes, C. S., & Barlow, D. H. (2017). An initial waitlist-controlled trial of the unified protocol for the treatment of emotional disorders in adolescents. Journal of Anxiety Disorders, 46, 46–55. https://doi.org/10.1016/j.janxdis.2016.10.006
Eisenberg, N., Spinrad, T., & Eggum-Wilkens, N. (2010). Emotion-related self-regulation and its relation to children’s maladjustment. Annual Review of Clinical Psychology, 6, 495–525. https://doi.org/10.1146/annurev.clinpsy.121208.131208
Gratz, K., Weiss, N., & Tull, M. (2015). Examining emotion regulation as an outcome, mechanism, or target of psychological treatments. Current Opinion in Psychology, 3. https://doi.org/10.1016/j.copsyc.2015.02.010
Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the difficulties in emotion regulation scale. Journal of Psychopathology and Behavioral Assessment, 26(41). https://doi.org/10.1023/B:JOBA.0000007455.08539.94
Gross, J. J. (2013). Emotion regulation: Taking stock and moving forward. Emotion, 13(3), 359–365. https://doi.org/10.1037/a0032135
Gross, J. J. (2015). Emotion regulation: Current status and future prospects. Psychological Inquiry, 26(1), 1–26. https://doi.org/10.1080/1047840X.2014.940781
Gross, J. J., & Muñoz, R. F. (1995). Emotion regulation and mental health. Clinical Psychology: Science and Practice, 2(2), 151–164. https://doi.org/10.1111/j.1468-2850.1995.tb00036.x
Halliburton, A., & Cooper, L. (2015). Applications and adaptations of Acceptance and Commitment Therapy (ACT) for adolescents. Journal of Contextual Behavioral Science, 4. https://doi.org/10.1016/j.jcbs.2015.01.002
Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (1999). Acceptance and commitment therapy: Guilford Press
Heleniak, C., Jenness, J. L., Stoep, A. V., McCauley, E., & McLaughlin, K. A. (2016). Childhood maltreatment exposure and disruptions in emotion regulation: A transdiagnostic pathway to adolescent internalizing and externalizing psychopathology. Cognitive Therapy and Research, 40(3), 394–415. https://doi.org/10.1007/s10608-015-9735-z
Helland, S. S., Mellblom, A. V., Kjøbli, J., Wentzel-Larsen, T., Espenes, K., Engell., T., & Kirkøen, B. (2022) Elements in mental health interventions associated with effects on emotion regulation in adolescents: A meta-analysis. Administration and Policy in Mental Health, 49, 1004–1018.https://doi.org/10.1007/s10488-022-01213-2
Higgins, J. P. T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M. J., Welch, V. A. (Eds.), (2023). Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023). Cochrane. Retrieved from www.training.cochrane.org/handbook
Linehan, M. (1993). Cognitive-behavioral treatment of borderline personality disorder. Guilford Press.
Linehan, M. M., & Wilks, C. R. (2015a). The course and evolution of dialectical behavior therapy. American Journal of Psychotherapy, 69(2), 97–110. https://doi.org/10.1176/appi.psychotherapy.2015.69.2.97
Linehan, M. M. (2015b). DBT® skills training manual (2nd ed.). Guilford Press.
Mazefsky, C. A., Conner, C. M., Breitenfeldt, K., Leezenbaum, N., Chen, Q., Bylsma, L. M., & Pilkonis, P. (2021). Evidence base update for questionnaires of emotion regulation and reactivity for children and adolescents. Journal of Clinical Child & Adolescent Psychology, 50(6), 683–707.
Marengo, D., & Montag, C. (2020). Digital phenotyping of big five personality via facebook data mining: A meta-analysis. Digital Psychology, 1(1), 52–64. https://doi.org/10.24989/dp.v1i1.1823
Marfo, P., & Okyere, G. A. (2019). The accuracy of effect-size estimates under normals and contaminated normals in meta-analysis. Heliyon, 5(6), e01838. https://doi.org/10.1016/j.heliyon.2019.e01838
Matusiewicz, A., Weaverling, G., & Lejuez, C. W. (2014). Emotion dysregulation among adolescents with borderline personality disorder. In C. Sharp & J. L. Tackett (Eds.), Handbook of Borderline personality disorder in children and adolescents (pp. 177–194). Springer.
McLaughlin, K. A., Aldao, A., Wisco, B. E., & Hilt, L. M. (2014). Rumination as a transdiagnostic factor underlying transitions between internalizing symptoms and aggressive behavior in early adolescents. Journal of Abnormal Psychology, 123(1), 13–23. https://doi.org/10.1037/a0035358
McLaughlin, K. A., Hatzenbuehler, M. L., Mennin, D. S., & Nolen-Hoeksema, S. (2011). Emotion dysregulation and adolescent psychopathology: A prospective study. Behaviour Research and Therapy, 49(9), 544–554. https://doi.org/10.1016/j.brat.2011.06.003
McRae, K., & Gross, J. J. (2020). Emotion regulation. Emotion (Washington, D.C.), 20(1), 1–9. https://doi.org/10.1037/emo0000703
Moltrecht, B., Deighton, J., Patalay, P., & Edbrooke-Childs, J. (2020). Effectiveness of current psychological interventions to improve emotion regulation in youth: A meta-analysis. European Child & Adolescent Psychiatry. https://doi.org/10.1007/s00787-020-01498-4
Nolen-Hoeksema, S., Wisco, B. E., & Lyubomirsky, S. (2008). Rethinking rumination. Perspectives on Psychological Science, 3(5), 400–424. https://doi.org/10.1111/j.1745-6924.2008.00088.x
Norton, P. J., & Paulus, D. J. (2016). Toward a unified treatment for emotional disorders: Update on the science and practice. Behavior Therapy, 47(6), 854–868. https://doi.org/10.1016/j.beth.2015.07.002
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., McGuinness, L. A., … Moher, D. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (Clinical Research Ed.), 372(71). https://doi.org/10.1136/bmj.n71
Perepletchikova, F., Nathanson, D., Axelrod, S. R., Merrill, C., Walker, A., Grossman, M., Rebeta, J., Scahill, L., Kaufman, J., Flye, B., Mauer, E., & Walkup, J. (2017). Randomized clinical trial of dialectical behavior therapy for preadolescent children with disruptive mood dysregulation disorder: Feasibility and outcomes. Journal of the American Academy of Child and Adolescent Psychiatry, 56(10), 832–840. https://doi.org/10.1016/j.jaac.2017.07.789
Rathus, J. H., & Miller, A. L. (2002). Dialectical behavior therapy adapted for suicidal adolescents. Suicide and Life-Threatening Behavior, 32(2), 146–157. https://doi.org/10.1521/suli.32.2.146.24399
Schneider, R. L., Arch, J. J., Landy, L. N., & Hankin, B. L. (2018). The longitudinal effect of emotion regulation strategies on anxiety levels in children and adolescents. Journal of Clinical Child & Adolescent Psychology, 47(6), 978–991. https://doi.org/10.1080/15374416.2016.1157757
Schäfer, J., Naumann, E., Holmes, E. A., Tuschen-Caffier, B., & Samson, A. C. (2017). Emotion regulation strategies in depressive and anxiety symptoms in youth: A meta-analytic review. Journal of Youth and Adolescence, 46(2), 261–276. https://doi.org/10.1007/s10964-016-0585-0
Segal, Z. V., Williams, M., & Teasdale, J. (2018). Mindfulness-based cognitive therapy for depression. Guilford Publications.
Silk, J. S., Steinberg, L., & Morris, A. S. (2003). Adolescents’ emotion regulation in daily life: Links to depressive symptoms and problem behavior. Child Development, 74(6), 1869–1880. https://doi.org/10.1046/j.1467-8624.2003.00643.x
Sloan, E., Hall, K., Moulding, R., Bryce, S., Mildred, H., & Staiger, P. K. (2017). Emotion regulation as a transdiagnostic treatment construct across anxiety, depression, substance, eating and borderline personality disorders: A systematic review. Clinical Psychology Review, 57, 141–163.
United Nations Department of Economic and Social Affairs. (2018). World youth report: Youth and the 2030 agenda for sustainable development. United Nations Publications.
Viechtbauer, W. (2010). Conducting meta-analyses in R with the metafor package. Journal of Statistical Software, 36(3), 1–48. https://doi.org/10.18637/jss.v036.i03
Weissman, D. G., Bitran, D., Miller, A. B., Schaefer, J. D., Sheridan, M. A., & McLaughlin, K. A. (2019). Difficulties with emotion regulation as a transdiagnostic mechanism linking child maltreatment with the emergence of psychopathology. Development and Psychopathology, 31(3), 899–915. https://doi.org/10.1017/s0954579419000348
Weisz, J., Bearman, S. K., Santucci, L. C., & Jensen-Doss, A. (2017a). Initial test of a principle-guided approach to transdiagnostic psychotherapy with children and adolescents. Journal of Clinical Child and Adolescent Psychology, 46(1), 44–58. https://doi.org/10.1080/15374416.2016.1163708
Weisz, J. R., Kuppens, S., Ng, M. Y., Eckshtain, D., Ugueto, A. M., Vaughn-Coaxum, R., Jensen-Doss, A., Hawley, K. M., KrumholzMarchette, L. S., Chu, B. C., Weersing, V. R., & Fordwood, S. R. (2017b). What five decades of research tells us about the effects of youth psychological therapy: A multilevel meta-analysis and implications for science and practice. The American Psychologist, 72(2), 79–117. https://doi.org/10.1037/a0040360
Wolff, J. C., Thompson, E., Thomas, S. A., Nesi, J., Bettis, A. H., Ransford, B., Scopelliti, K., Frazier, E. A., & Liu, R. T. (2019). Emotion dysregulation and non-suicidal self-injury: A systematic review and meta-analysis. European Psychiatry: The Journal of the Association of European Psychiatrists, 59, 25–36. https://doi.org/10.1016/j.eurpsy.2019.03.004
Young, K. S., Sandman, C. F., & Craske, M. G. (2019). Positive and negative emotion regulation in adolescence: Links to anxiety and depression. Brain Sciences, 9(4). https://doi.org/10.3390/brainsci9040076
Acknowledgements
The authors would like to thank Agathe Backer-Grøndahl, Siv Linnerud, Josefine Bergseth, Thale Holtan, Erik Frogner, and Melvin Treider who contributed to data handling and assessments. We would like to thank Siri Haugestad-Helland, Hans B. Bergsund, and associate professors Serap Keles, University of Stavanger and Patty Leijten, University of Amsterdam for manuscript edits.
Funding
Open access funding provided by University of Oslo (incl Oslo University Hospital).
Author information
Authors and Affiliations
Contributions
Author JK had the original idea of the paper. All authors except TWL contributed to forming the research questions, inclusion and exclusion criteria. KHN conducted the literature search. Authors KE, KR, KHN, JK and PW, along with research assistants read abstracts and full-text articles. Authors KE and PW were responsible for the data extraction and Risk of Bias analyses, along with research assistants. TWL analyzed and interpreted the data together with KE. All authors wrote, read, and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical Approval
No ethical approval was necessary for this review article.
Competing of Interest
The authors declare they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Espenes, K., Tørmoen, A.J., Rognstad, K. et al. Effect of Psychosocial Interventions on Children and Youth Emotion Regulation: A Meta-Analysis. Adm Policy Ment Health (2024). https://doi.org/10.1007/s10488-024-01373-3
Accepted:
Published:
DOI: https://doi.org/10.1007/s10488-024-01373-3