
Abstract
The assessment of heart rate variability (HRV) upon waking has been proposed as a method to evaluate mental health; however, owing to large individual differences among athletes, it is unclear whether HRV is adequate to predict mental health decline. In this study, we sought to establish this by evaluating HRV upon awakening in one athlete over 20 months. We assessed mental health once a month by calculating the depression index. In addition, self-reported training load and psychological fatigue index were assessed as psychological indices for athletes. Heart rate and HRV were each measured three days per week in both resting (supine) and standing (upright) positions. The results showed that orthostatic HRV upon waking had moderate linear relationships with the scores on the depression index and psychological fatigue index. By contrast, self-reported training load, a measure of physical stressor, was not associated with HRV. The findings suggest that the repeated assessment of HRV upon waking and mental health indicators may be useful in preventing mental health decline in athletes.
Similar content being viewed by others
Introduction
The intense mental and physical demands placed on elite athletes may increase their susceptibility to decreasing mental health and risk-taking behaviors (Hughes & Leavey, 2012), leading to low performance and physical health problems. In addition to physical and competitive stress, elite athletes face unique stressors. These include public pressure on mainstream and social media, mental strain from non-competitive environments (such as academics or work), and fear of early career termination due to injury or demotivation (Bruner et al., 2008; Fletcher & Wagstaff, 2009; Hanton et al., 2005; Noblet & Gifford, 2002; Woodman & Hardy, 2001). Assessing these physical and mental stressors may help prevent low performance, decreased mental health, burn-out, and drop-outs. However, these assessments vary widely among individuals, and stressors and influencing factors vary among individual athletes, indicating that the optimal assessment index has not yet been established.
The main tool used to assess mental health and stress is a questionnaire-based method to evaluate the degree of congruence with one’s own psychological state. The advantage of this method is that it provides information quickly. Conversely, psychological indicators are influenced by events at the time of measurement (e.g., diet and training), and thus transient mood can affect the results. In addition, athletes may not accurately complete the questionnaire as the results of mental health and stress measures may affect their evaluation by their supervisors and coaches. Therefore, the questionnaire-based evaluation alone may not accurately assess an athlete’s state of stress. Furthermore, the degree of stress is influenced by many individual differences, including gender (Kaiseler et al., 2012; Nicholls et al., 2009), personality traits (Kaiseler et al., 2012), and mental toughness (Kaiseler et al., 2009). To assess the impact of stress on athletes, longitudinal tracking of changes in their mental health and additional non-psychological evaluation measures are required.
Heart rate variability (HRV) assessment may be useful in assessing the balance between physical and mental stress, such as training load, to which athletes are subjected. HRV is a physiological indicator of emotional regulation related to mental health (Thayer et al., 2012). It can be measured noninvasively using a heart rate monitor, which minimizes the burden on the athlete and is effective for long-term monitoring of stress (Föhr et al., 2017). HRV refers to the variability of the interval between heartbeats and reflects the autonomic regulation of the heart. Healthy individuals are characterized by efficient autonomic mechanisms, high adaptive capacity, and high HRV, while low HRV indicates an abnormal autonomic nervous system and poor adaptation, thus expressing physiological malfunction (Porges, 1992, 1995; Pumprla et al., 2002; Vanderlei et al., 2009). Previous studies suggest that it is possible to predict declining mental health based on declining HRV (Chalmers et al., 2014; Zou et al., 2018). Several studies have already examined the usefulness of HRV-based monitoring for athletes (Egan-Shuttler et al., 2020; Morales et al., 2014; Rodrigues et al., 2021), but most have used HRV as an indicator of the amount of mental and physical stress on athletes. However, there is little evidence that it is useful in predicting mental health decline.
Therefore, the present study filled this gap in the literature by clarifying whether combining psychological indices and HRV measurements upon waking could assess athletes’ mental health conditions. We examined whether HRV is related to psychological and physical stressors such as training load. A case study of one top athlete was employed to leave aside individual differences in stress factors, athletic performance, and athletic events.
Methods
Participant
An elite international-level female wheel gymnastics athlete (31 years old in 2022; competing for 13 years and has competed in 10 World Championships, including one championship and five prizes) participated in this project. She reported being a non-smoker and declared no chronic physical or mental health problems at the start of the study. All procedures were approved by the Institutional Ethics Committee of Utsunomiya University and were conducted in accordance with the latest version of the Declaration of Helsinki. The participant provided written informed consent and approved the final version of this manuscript.
Procedures
Data were collected throughout 20 months (January 2021 to July 2022), covering competitive (two national wheel gymnastics competitions), intense training, and predominantly resting phases. Psychological scales assessing mental health were applied every month. Heart rate and HRV upon waking were measured three times each week.
HRV Measurements
Waking HRV was measured by Recovery Pro software using the Polar H10 sensor and a Vantage V watch (Polar Electro Oy, Kempele, Finland). Recovery Pro is a program that measures heart rate and the root mean square of successive differences (RMSSD) three times a week at rest and standing up upon waking up. The average of the three data sets was used for analysis as the measured heart rate and RMSSD. The athlete went to bed wearing H10 on the chest starting the night before the measurement day. Upon waking, she followed the expound instructions provided by Vantage V to perform the measurement. The data thus collected were stored in Polar Flow from Vantage V. Polar Flow stores average heart rate per minute and RMSSD, which were retrieved and used for analysis in this study.
Psychological Measurements
As psychological scales, the participant completed the Profile of Mood States 2nd Edition (POMS2), the Kessler Psychological Distress Scale-6 (K6), the Baron Depression Screener for Athletes (BDSA), the Sense of Coherence (SOC) Scale, self-reported training load, and the Competition Stressor Scale.
POMS2
The POMS2 (Yokoyama & Watanabe, 2015) contains 35 items and evaluates seven mood states (anger-hostility, confusion-bewilderment, depression-ejection, fatigue-inertia, tension-anxiety, vigor-activity, and friendliness). In this study, only the 10-item subset on vigor-activity and fatigue-inertia was used to reduce the participant’s psychological burden.
K6
The Japanese version of the K6 scale was used (Furukawa et al., 2008). This is a powerful screening scale for psychological distress (Kessler et al., 2002). The respondent answered six items rated on a five-point Likert scale, and responses were scored from 0 to 4. A higher total score corresponded to worse mental health conditions.
SOC
The 13-item seven-point version of the SOC Scale (Antonovsky, 1987) was employed. Each question was rated on a scale from 1 (lowest) to 7 (highest), and the coding for items 1, 2, 3, 7, and 10 was reversed. SOC total scores ranged from 13 to 91, with higher ones indicating a greater SOC.
Self-Reported Training Load
Additionally, the self-reported training load was calculated as the product of monthly training hours and training intensity. An 11-point scale, starting from 0 to 10, was used to measure the rate of perceived exertion (RPE) (Foster et al., 2001). The adequacy of the self-reported training load was confirmed by training time and training volume measured with a heart rate monitor.
Competition Stressor Scale
To measure competitive stress, we used the Competition Stressor Scale (Asanuma et al., 2015). This scale is composed of 28 questions that record the frequency of stressors over the past month, and each item is rated on a four-point scale from 0 (“not at all”) to 3 (“very often”). It comprises five factors, and the score range for each is as follows: “interpersonal relationships,” 0–24 points; “competition results,” 0–9 points; “expectation and pressure from others,” 0–15 points; and “motivation loss,” 0–21 points. Higher scores indicate higher stress levels.
BDSA
The BDSA is a 10-question self-report questionnaire that addresses mood, sports-related anhedonia, weight loss, fatigue, self-image, substance abuse, suicidality, and other parameters over the past two weeks, and has been validated against the Beck Depressive Inventory (Baron et al., 2013; Polat et al., 2015). The scale has no cut-off scores that automatically suggest a diagnosis of major depressive disorder. The items are scored on a three-point Likert scale (total score ranges from 0 to 20, with a higher score representing more severe depressive symptoms). In this study, we used the Japanese translation developed by a previous study (Ojio et al., 2020).
Training Time and Volume
Training time and volume were measured using the Polar H10 sensor and a Vantage V watch (Polar Electro Oy, Kempele, Finland). Training volume was calculated by the Polar flow web service based on training session intensity measured using heart rate and training time.
Statistical Analysis
All analyses were performed using R software (4.1.2) and EZR (Easy R) on the R Commander package (Kanda, 2013). To clarify the expected relationships between all parameters, we measured the Pearson correlation coefficient. Correlation coefficients were interpreted based on the following criteria: r values between 0 and 0.3 indicated a weak linear relationship, r values between 0.3 and 0.7 indicated a moderate linear relationship, and r values between 0.7 and 1.0 indicated a strong linear relationship (Ratner, 2009).
Results
Training Load
The training time and training volume (calories) measured with the heart rate monitor and the self-reported training load during the measurement period are shown in Fig. 1. Similar changes and strong positive linear relationships were observed between them (training time and training calories: r = .97; training time and self-reported training load: r = .88; training calories and self-reported training load: r = .91).

Training Load
[A] Training time and training volume as measured by heart rate monitor [B] Voluntary training volume (product of subjective exercise intensity and time).
Psychological Parameters
Figure 2 displays the results for BDSA and K6, indices of depression, POMS2, an index of vigor-activity and fatigue-inertia, and SOC.

Psychological parameters
Time series data of depression index ([A]BDSA [B]K6), [C] mood index (vigor-activity, fatigue-inertia of POMS2), and [D] sense of coherence.
Figure 3 exhibits the results of stressors measured by the Competition Stressor Scale; Expectations and pressure, and Competition results were higher for each competition entered.

Stressors measured by the Competition Stressor Scale
Time series data for the Competition Stressor Scale ([A] Motivation loss [B] Competition results [C] Evaluation from one’s surroundings [D] Interpersonal relationships [E] Expectations and pressure from others).
Waking Heart Rate and HRV
Figure 4 presents the results of waking heart rate and RMSSD. The waking lying-down heart rate and RMSSD showed a strong negative linear relationship (r = − .71), while the waking standing heart rate and RMSSD showed a weak negative linear relationship (r = − .27).

Waking heart rate and heart rate variability
[A] Heart rate variability and [B] heart rate at rest (supine position) and while standing (upright position) during waking and time series data.
Heart Rate Index and Psychological Performance
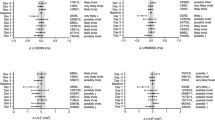
Heart rate upon waking had a weak negative linear relationship with any psychological performance [waking resting HR and K6 (r = − .02), fatigue-Inertia of POMS2 (r = − .07) and vigor-activity of POMS2 (r = .09); waking standing HR and K6 (r = .02), fatigue-Inertia of POMS2 (r = .14) and vigor-activity of POMS2 (r = .05)]. However, waking standing RMSSD had a moderate negative linear relationship with K6 (r = − .54) and a moderate negative linear relationship with fatigue-Inertia of POMS2 (r = − .61) (Fig. 5). Waking standing RMSSD had a weak negative linear relationship with vigor-activity of POMS2 (r = − .07). Waking resting RMSSD had a weak negative linear relationship with K6 (r = − .17) and fatigue-Inertia of POMS2 (r = − .10).

Relationship between waking heart rate variability and mental health
Waking standing heart rate variability was negatively correlated with [A] K6, a depression index, and [B] POMS2, a fatigue index.
Discussion
Athletes are required to perform at a high level, and they need to maintain athletic function as well as sound mental health. However, most condition assessments focus only on athletic performance and neglect mental health. This may be because stressors and their effects on mental health are greatly influenced by individuals’ athletic characteristics and differences, making it difficult to reach a unanimous view on an accurate evaluation index for mental health. Therefore, in this study, we conducted a 20-month condition assessment of one top wheel gymnastics athlete to clarify whether such evaluation, combining HRV and psychological measures, can predict mental health decline in athletes. The results showed that orthostatic HRV upon waking had moderate negative linear relationships with the results of K6, a mental health index used to diagnose depression, and with the fatigue index of POMS2; thus, it may be effective in making predictions regarding mental health status. By contrast, HRV only showed weak linear relationships with the Competition Stressor Scale and self-reported training load, and we did not find a stressor for HRV decline.
In the present study, waking standing RMSSD had a moderate negative linear relationship with K6 and a moderate negative linear relationship with fatigue-Inertia of POMS2. Previous studies have reported that RMSSD decreases during transient anxiety induction (Ritsert et al., 2022). The moderate negative linear relationship between K6 and RMSSD in the present study aligns with previous studies. Notably, K6, which is used to screen for mental disorders such as depression and anxiety disorders, showed the highest score of six points immediately after the World Championships (individual) in Time 19. The cut-off value of K6 was five points, and scores above five indicated “psychological distress” (when used for mood and anxiety disorders screening, detection sensitivity was 100.0%, and specificity was 68.7%; Sakurai et al., 2010). Therefore, a decline in mental health was suspected before and after the World Championships (individual). In the POMS2, which confirmed mood fluctuation, both vigor-activity and fatigue-inertia (POMS2) showed fluctuation from Time 1 to 10 but were relatively stable from Time 11 to 18 in the latter half of the month and were stable for the World Championships held from Time 18 to 19. Although high scores on K6 were recorded at Time 19, vigor activity on POMS2 was also high. Only a weak linear relationship was found between fatigue-inertia on POMS2 and training load (r = − .20), suggesting that fatigue-inertia represents mental fatigue or malaise.
Subsequently, we examined whether HRV is related to physical and mental stressors. The training load assessed subjectively by the athlete showed a strong positive linear relationship with the training time and calorie expenditure measured with a heart rate monitor, confirming that their subjective load and the actual training load were almost identical. In addition, the training load increased in accordance with the preparation for the World Championships (individual) at Time 19. The results of this study, which showed similar changes in objective and subjective training workload using heart rate monitors, suggest that the athlete in this study could assess her training workload accurately. However, the relationship between training load and waking RMSSD [standing (r = .17)/resting (r = − .30)] was shown to be a weak linear relationship. Regarding psychological stressors, only Competition Results showed a large change, suggesting that it was the main stressor for this athlete. Conversely, Competition Results were relatively low immediately before the competition and increased rapidly afterward, suggesting that this stressor fluctuated in response to the results of a competition. However, this psychological stressor showed only a weak linear relationship with waking HRV [resting (r = .07)/standing (r = − .16)]. In addition, Competition Results showed only a weak linear relationship with BDSA (r = .10), K6 (r = − .04), suggesting that it is unlikely that this stressor itself had a direct effect on match performance or mental health. Although previous studies have suggested that HRV is useful for quantifying training load, such as a decrease in sleep after high-intensity exercise (Hynynen et al., 2010), only a weak linear relationship was found in the present study. HRV may also be influenced by factors other than training. For example, it is known to be influenced by a wide range of physiological, pathological, neuropsychological, lifestyle, and environmental factors (Fatisson et al., 2016). A study on athletes suggests that daily stress outside training may have affected RMSSD, especially in those who failed to predict HRV variability due to training stimuli (Williams et al., 2018). The management of training load in athletes does not consider the amount of training itself but rather the load during sports activity as “a stimulus to a biological system composed of a complex combination of physiological, psychological, and mechanical stresses” (Soligard et al., 2016). These results suggest that RMSSD during arousal may comprehensively indicate training load (physical stressor) and mental stressor.
Finally, SOC only had a weak linear relationship with waking RMSSD and mental health index [K6 (r = .02) and fatigue (POMS2)(r = − .20)]. Previous cross-sectional studies examining the relationship between SOC and HRV have reported significant positive correlations (Nasermoaddeli et al., 2004). However, no study has examined the relationship between SOC and HRV variation within individuals as in this study, and this is the first finding of its kind. In addition, higher SOC was reported to have a higher subjective quality of life, health, and well-being (Eriksson & Lindström, 2007), but no relationship was found for intraindividual change in this study. The mean score for SOC was 72 points (SD = 5.21) and remained high throughout the 20 months, although some fluctuations were observed. The score was nearly 20 points higher than the baseline value of 54 points (SD = 12.2) for Japanese women aged 25–34 (Togari et al., 2015), indicating that this athlete had a high stress-coping ability. These results suggest that evaluating athletes’ mental health and its influential factors is challenging using a single psychological measure.
It is known that the stress response is largely regulated by the autonomic nervous system and can be assessed by measuring HRV (McEwen, 2007). It has been reported that a decrease in HRV occurs in many psychiatric disorders (Kemp & Quintana, 2013). Furthermore, meta-analyses have reported that HRV can predict mortality and negative physical and mental states, albeit in non-athletes (Jarczok et al., 2022). These results suggest that HRV decline is associated with mental health decline, suggesting that HRV measurement in athletes may be useful in predicting mental health decline that occurs during training. Notably, waking HRV was differentially associated with lower mental health depending on how it was measured. Only a weak linear relationship was found between RMSSD during rest upon waking and RMSSD while standing upon waking, suggesting that they are distinct condition indices. Although the former showed only a weak linear relationship with psychological indices, the latter showed moderate linear relationships with K6 and POMS2 Fatigue scores, which are used to diagnose depression, suggesting that the awake-standing HRV may be useful in predicting mental health decline.
One limitation of this study is that it is a single case study of one top wheel gymnastics athlete, so it is impossible to say whether similar trends would be observed in all athletes. In this study, we were concerned that individual differences in the psychological index and HRV could lead to the discovery of a false relationship between HRV and mental health, and we sought to address this through a single long-term case study of one top wheel gymnastics athlete. However, for example, in the case of endurance events, which have been studied extensively and have different competition characteristics, the evaluation indices reflected by the HRV may differ. Therefore, studies that consider the characteristics of the events are necessary. In addition, although it was shown that resting HRV and standing HRV may reflect different physiological responses, the difference between the two indices has not yet been examined in practice and should be studied in the future. Furthermore, although this study was conducted during the coronavirus disease 2019 (COVID-19) pandemic, it did not account for the impact of the pandemic. It has been suggested (World Health Organization, n.d.) that the COVID-19 pandemic may have had a detrimental effect on mental health, including anxiety and stress; however, higher SOC may have helped reduce the degree of distress and stress during this period (Kase et al., 2023). The SOC of the athlete in this study did not change significantly during the measurement period, suggesting that the impact of the pandemic was small and did not affect the study results.
Conclusions
This study revealed that awake-standing HRV is related to depression and fatigue indices in athletes. The significance of this study is that, over 20 months during the COVID-19 pandemic period, we continuously measured HRV and applied psychological scales to assess mental health in one athlete. Although there have been many studies on condition assessment using waking HRV methods in endurance events, few have reported scoring events, which is significant. This study’s findings, including the POMS2 and K6 scores, which were found to be related to HRV in this study, can be useful biomarkers for the prediction of precarious mental health.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
References
Antonovsky, A. (1987). Unraveling the mystery of health: How people manage stress and stay well (p. 218). San Francisco, CA: Jossey-Bass.
Asanuma, T., Takeda, F., Monma, T., & Hotoge, S. (2015). Relationship between mental health and competitive stressor among collegiate athletes–differences in the level of sense of coherence (japanese). Japanese Journal of Health Promotion and Physical Therapy, 17(1), 7–14.
Baron, D. A., Baron, S. H., Tompkins, J., & Polat, A. (2013). Assessing and treating depression in athletes. In D. A. Baron, C. Reardon, & S. H. Baron (Eds.), Clinical sports psychiatry: An international perspective (pp. 65–78). Chichester, West Sussex: Wiley. https://doi.org/10.1002/9781118404904.ch7.
Bruner, M. W., Munroe-Chandler, K. J., & Spink, K. S. (2008). Entry into elite sport: A preliminary investigation into the transition experiences of rookie athletes. Journal of Applied Sport Psychology, 20(2), 236–252. https://doi.org/10.1080/10413200701867745.
Chalmers, J. A., Quintana, D. S., Abbott, M. J. A., & Kemp, A. H. (2014). Anxiety disorders are associated with reduced heart rate variability: A meta-analysis. Frontiers in Psychiatry, 5, 80. https://doi.org/10.3389/fpsyt.2014.00080.
Egan-Shuttler, J. D., Edmonds, R., & Ives, S. J. (2020). The efficacy of heart rate variability in tracking travel and training stress in youth female rowers: A preliminary study. Journal of Strength and Conditioning Research, 34(11), 3293–3300. https://doi.org/10.1519/JSC.0000000000002499.
Eriksson, M., & Lindström, B. (2007). Antonovsky’s sense of coherence scale and its relation with quality of life: A systematic review. Journal of Epidemiology and Community Health, 61(11), 938–944. https://doi.org/10.1136/jech.2006.056028.
Fatisson, J., Oswald, V., & Lalonde, F. (2016). Influence diagram of physiological and environmental factors affecting heart rate variability: An extended literature overview. Heart International, 11(1), e32–e40. https://doi.org/10.5301/heartint.5000232.
Fletcher, D., & Wagstaff, C. R. D. (2009). Organizational psychology in elite sport: Its emergence, application and future. Psychology of Sport and Exercise, 10(4), 427–434. https://doi.org/10.1016/j.psychsport.2009.03.009.
Föhr, T., Tolvanen, A., Myllymäki, T., Järvelä-Reijonen, E., Peuhkuri, K., Rantala, S., Kolehmainen, M., Korpela, R., Lappalainen, R., Ermes, M., Puttonen, S., Rusko, H., & Kujala, U. M. (2017). Physical activity, heart rate variability-based stress and recovery, and subjective stress during a 9-month study period. Scandinavian Journal of Medicine & Science in Sports, 27(6), 612–621. https://doi.org/10.1111/sms.12683.
Foster, C., Florhaug, J. A., Franklin, J., Gottschall, L., Hrovatin, L. A., Parker, S., Doleshal, P., & Dodge, C. (2001). A new approach to monitoring exercise training. Journal of Strength and Conditioning Research, 15(1), 109–115.
Furukawa, T. A., Kawakami, N., Saitoh, M., Ono, Y., Nakane, Y., Nakamura, Y., Tachimori, H., Iwata, N., Uda, H., Nakane, H., Watanabe, M., Naganuma, Y., Hata, Y., Kobayashi, M., Miyake, Y., Takeshima, T., & Kikkawa, T. (2008). The performance of the japanese version of the K6 and K10 in the World Mental Health Survey Japan. International Journal of Methods in Psychiatric Research, 17(3), 152–158. https://doi.org/10.1002/mpr.257.
Hanton, S., Fletcher, D., & Coughlan, G. (2005). Stress in elite sport performers: A comparative study of competitive and organizational stressors. Journal of Sports Sciences, 23(10), 1129–1141. https://doi.org/10.1080/02640410500131480.
Hughes, L., & Leavey, G. (2012). Setting the bar: Athletes and vulnerability to mental illness. The British Journal of Psychiatry, 200(2), 95–96. https://doi.org/10.1192/bjp.bp.111.095976.
Hynynen, E., Vesterinen, V., Rusko, H., & Nummela, A. (2010). Effects of moderate and heavy endurance exercise on nocturnal HRV. International Journal of Sports Medicine, 31(6), 428–432. https://doi.org/10.1055/s-0030-1249625.
Jarczok, M. N., Weimer, K., Braun, C., Williams, D. P., Thayer, J. F., Gündel, H. O., & Balint, E. M. (2022). Heart rate variability in the prediction of mortality: A systematic review and meta-analysis of healthy and patient populations. Neuroscience and Biobehavioral Reviews, 143, 104907. https://doi.org/10.1016/j.neubiorev.2022.104907.
Kase, T., Ueno, Y., & Endo, S. (2023). Association of sense of coherence and resilience with distress and infection prevention behaviors during the coronavirus disease pandemic. Current Psychology. https://doi.org/10.1007/s12144-023-04359-w.
Kaiseler, M., Polman, R. C. J., & Nicholls, A. R. (2012). Gender differences in appraisal and coping: An examination of the situational and dispositional hypothesis. International Journal of Sport Psychology, 43(1), 1–14. https://doi.org/10.7352/IJSP.2012.43.001.
Kaiseler, M., Polman, R. C. J., & Nicholls, A. R. (2012). Effects of the big five personality dimensions on appraisal coping, and coping effectiveness in sport. European Journal of Sport Science, 12(1), 62–72. https://doi.org/10.1080/17461391.2010.551410.
Kaiseler, M., Polman, R., & Nicholls, A. (2009). Mental toughness, stress, stress appraisal, coping and coping effectiveness in sport. Personality and Individual Differences, 47(7), 728–733. https://doi.org/10.1016/j.paid.2009.06.012.
Kanda, Y. (2013). Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplantation, 48(3), 452–458. https://doi.org/10.1038/bmt.2012.244.
Kemp, A. H., & Quintana, D. S. (2013). The relationship between mental and physical health: Insights from the study of heart rate variability. International Journal of Psychophysiology, 89(3), 288–296. https://doi.org/10.1016/j.ijpsycho.2013.06.018.
Kessler, R. C., Andrews, G., Colpe, L. J., Hiripi, E., Mroczek, D. K., Normand, S. L. T., Walters, E. E., & Zaslavsky, A. M. (2002). Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychological Medicine, 32(6), 959–976. https://doi.org/10.1017/s0033291702006074.
McEwen, B. S. (2007). Physiology and neurobiology of stress and adaptation: Central role of the brain. Physiological Reviews, 87(3), 873–904. https://doi.org/10.1152/physrev.00041.2006.
Morales, J., Alamo, J. M., García-Massó, X., Buscà, B., López, J. L., Serra-Añó, P., & González, L. M. (2014). Use of heart rate variability in monitoring stress and recovery in judo athletes. Journal of Strength and Conditioning Research, 28(7), 1896–1905. https://doi.org/10.1519/JSC.0000000000000328.
Nasermoaddeli, A., Sekine, M., & Kagamimori, S. (2004). Association between sense of coherence and heart rate variability in healthy subjects. Environmental Health and Preventive Medicine, 9(6), 272–274. https://doi.org/10.1007/BF02898142.
Nicholls, A., Polman, R., Morley, D., & Taylor, N. J. (2009). Coping and coping effectiveness in relation to a competitive sport event: Pubertal status, chronological age, and gender among adolescent athletes. Journal of Sport & Exercise Psychology, 31(3), 299–317. https://doi.org/10.1123/jsep.31.3.299.
Noblet, A. J., & Gifford, S. M. (2002). The sources of stress experienced by professional australian footballers. Journal of Applied Sport Psychology, 14(1), 1–13. https://doi.org/10.1080/10413200209339007.
Ojio, Y., Matsunaga, A., Hatakeyama, K., Kawamura, S., Horiguchi, M., Baron, D., & Fujii, C. (2020). Developing a japanese version of the Baron Depression Screener for athletes among male professional rugby players. International Journal of Environmental Research and Public Health, 17(15), 5533. https://doi.org/10.3390/ijerph17155533.
Polat, A., Cakir, U., Karabulut, U., Tural, U., & Baron, D. (2015). Reliability and validity of turkish form of Baron Depression Screener for athletes. Bulletin of Clinical Psychopharmacology, 25(Suppl. 1), S134.
Porges, S. W. (1992). Vagal tone: A physiologic marker of stress vulnerability. Pediatrics, 90(3), 498–504. https://doi.org/10.1542/peds.90.3.498.
Porges, S. W. (1995). Cardiac vagal tone: A physiological index of stress. Neuroscience and Biobehavioral Reviews, 19(2), 225–233. https://doi.org/10.1016/0149-7634(94)00066-a.
Pumprla, J., Howorka, K., Groves, D., Chester, M., & Nolan, J. (2002). Functional assessment of heart rate variability: Physiological basis and practical applications. International Journal of Cardiology, 84(1), 1–14. https://doi.org/10.1016/s0167-5273(02)00057-8.
Ratner, B. (2009). The correlation coefficient: Its values range between + 1/–1, or do they? Journal of Targeting Measurement and Analysis for Marketing, 17, 139–142. https://doi.org/10.1057/jt.2009.5.
Ritsert, F., Elgendi, M., Galli, V., & Menon, C. (2022). Heart and breathing rate variations as biomarkers for anxiety detection. Bioengineering, 9(11), 711. https://doi.org/10.3390/bioengineering9110711.
Rodrigues, G. D., Gurgel, J. L., Gonçalves, T. R., & Soares, P. P. D. S. (2021). The physical capacity of rowing athletes cannot reverse the influence of age on heart rate variability during orthostatic stress. Anais da Academia Brasileira de Ciencias, 93(suppl 3), e20201677. https://doi.org/10.1590/0001-3765202120201677.
Sakurai, K., Kawakami, N., Yamaoka, K., Ishikawa, H., & Hashimoto, H. (2010). The impact of subjective and objective social status on psychological distress among men and women in Japan. Social Science & Medicine, 70(11), 1832–1839. https://doi.org/10.1016/j.socscimed.2010.01.019.
Soligard, T., Schwellnus, M., Alonso, J. M., Bahr, R., Clarsen, B., Dijkstra, H. P., Gabbett, T., Gleeson, M., Hägglund, M., Hutchinson, M. R., van Janse, C., Khan, K. M., Meeusen, R., Orchard, J. W., Pluim, B. M., Raftery, M., Budgett, R., & Engebretsen, L. (2016). How much is too much? (part 1) International Olympic Committee consensus statement on load in sport and risk of injury. British Journal of Sports Medicine, 50(17), 1030–1041. https://doi.org/10.1136/bjsports-2016-096581.
Thayer, J. F., Ahs, F., Fredrikson, M., Sollers, J. J. 3rd, & Wager, T. D. (2012). A meta-analysis of heart rate variability and neuroimaging studies: Implications for heart rate variability as a marker of stress and health. Neuroscience and Biobehavioral Reviews, 36(2), 747–756. https://doi.org/10.1016/j.neubiorev.2011.11.009.
Togari, T., Yamazaki, Y., Nakayama, K., Yokoyama, Y., Yonekura, Y., & Takeuchi, T. (2015). Nationally representative score of the japanese language version of the 13-item 7-point sense of coherence scale (japanese). Nihon Koshu Eisei Zasshi (Japanese Journal of Public Health), 62(5), 232–237. https://doi.org/10.11236/jph.62.5_232.
Vanderlei, L. C. M., Pastre, C. M., Hoshi, R. A., de Carvalho, T. D., & de Godoy, M. F. (2009). Basic notions of heart rate variability and its clinical applicability. Revista Brasileira de Cirurgia Cardiovascular (Brazilian Journal of Cardiovascular Surgery), 24(2), 205–217. https://doi.org/10.1590/s0102-76382009000200018.
Williams, S., West, S., Howells, D., Kemp, S. P. T., Flatt, A. A., & Stokes, K. (2018). Modelling the HRV response to training loads in elite rugby sevens players. Journal of Sports Science and Medicine, 17(3), 402–408.
Woodman, T., & Hardy, L. (2001). A case study of organizational stress in elite sport. Journal of Applied Sport Psychology, 13(2), 207–238. https://doi.org/10.1080/104132001753149892.
World Health Organization. (n.d.). The impact of COVID-19 on mental health cannot be made light of. World Health Organization. https://www.who.int/news-room/feature-stories/detail/the-impact-of-covid-19-on-mental-health-cannot-be-made-light-of
Yokoyama, K., & Watanabe, K. (2015). Japanese translation of POMS 2: Profile of Mood States (2nd ed.). Tokyo: Kaneko Shobo.
Zou, L., Sasaki, J. E., Wei, G. X., Huang, T., Yeung, A. S., Neto, O. B., Chen, K. W., & Hui, S. S. C. (2018). Effects of mind-body exercises (Tai Chi/Yoga) on heart rate variability parameters and perceived stress: A systematic review with meta-analysis of randomized controlled trials. Journal of Clinical Medicine, 7(11), 404. https://doi.org/10.3390/jcm7110404.
Acknowledgements
This work was supported in part by the Cooperative Research Grant of Niigata University of Health and Welfare. We are grateful to H. Matsuoka (University of Tsukuba, Japan) and T. Shimokubo (Niigata University of Health and Welfare, Japan) for helping with the statistical analysis. We would like to thank Editage (www.editage.com) for English language editing.
Funding
This work was supported by the Cooperative Research Grant of Niigata University of Health and Welfare.
Author information
Authors and Affiliations
Contributions
Both authors worked on the conceptualization of this study, contributed to data collection and analysis, and wrote the manuscript.
Corresponding author
Ethics declarations
Ethics approval
Approval was obtained from the Institutional Ethics Committee of Utsunomiya University. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Competing Interests
The authors have no relevant financial or non-financial interests to disclose.
Consent to Participate
Written informed consent was obtained from the participant.
Consent to Publish
The participant has consented to the submission of the original article to the journal.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Matsuura, Y., Ochi, G. The Potential of Heart Rate Variability Monitoring for Mental Health Assessment in Top Wheel Gymnastics Athletes: A Single Case Design. Appl Psychophysiol Biofeedback 48, 335–343 (2023). https://doi.org/10.1007/s10484-023-09585-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10484-023-09585-3