
Abstract
One of the most known gaps between genders relate to survival prospects. The longer life expectancy of women implies greater longevity and morbidity risks and thus involves different needs between genders in silver ages, e.g., health care costs. In this paper, we uncover stylized evidence about the age pattern of the gender gap in mortality, by showing “facts” that are consistently verified in both COVID-19 and non-COVID-19 situations. We thus capture the general shape of the relationship between male and female mortality rates as it evolves with age. We target the ratio of male to female mortality rates, namely the Gender Gap Ratio (GGR). By means of a graduation technique, we show that the GGR evolution over age follows, for all the nations under study, the same pattern, consisting in a systematic interchange between increasing and decreasing trends within specific age intervals. In other terms, the GGR has an almost stylized shape, with distinct age-specific components, in terms of its slope and curvature.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
1 Introduction
The gender gap in longevity has significant implications for the management of the demographic transition and the construction of a culture of healthy ageing. The longer life expectancy of women implies greater longevity and morbidity risks and thus involves different needs between genders in silver ages, e.g., dissimilar health-care costs and a different exposition to the mental and cognitive burden arising from social isolation and loneliness (Chen et al., 2021). Countries should be well prepared to address the health, social and economic challenges posed by the gender gap in the population ageing.
As stressed by Bambra et al. (2021), the gender patterning of COVID-19 pandemic may reinforce what is known as “gender health paradox”, consisting in higher rates of morbidity and lower rates of mortality for women compared to men. Furthermore, the post-COVID-19 global economic fall is likely to exacerbate the economic and health inequalities between men and women, with cross-country differences stemming from diverse public policies and socio-economic conditions (Simba & Ngcobo, 2020; Franklin et al., 2021).
Some papers have focused on the mapping and impact assessment of the gender gap in longevity, to extrapolate the peculiar characteristics of such a phenomenon, to explain its evolution and to measure its consequences (e.g., Sundberg et al. 2018; Zarulli et al. 2021; Zarulli et al. 2022). Furthermore, several studies describe mortality curves by means of simple biologically interpretable mathematical models allowing to reproduce the peculiar age pattern of human mortality (see, e.g., Forfar (2006) for a review). In this respect, mortality laws are used to graduate raw mortality rates as resulting from statistical observation. Such observed mortality rates, indeed, may show an erratic behaviour that may be not justifiable based on past experience or intuition. Graduation procedures, instead, allow to obtain a progressive change of period mortality rates over age, while preserving the underlying pattern. Other than parametric approaches to graduation, involving the choice of mortality laws, non-parametric graduation methods are often adopted, e.g., methods based on spline functions to capture mortality patterns over age of a single population or mortality differentials (e.g., inter alia, McCutcheon 1985; van der Linde et al. 1995; Currie et al. 2004; Luoma et al. 2012; Dodd et al. 2018; Atance et al. 2020; Tang et al. 2023).
In this paper, we uncover stylized evidence about the age pattern of the gender gap in mortality, by showing “facts” that are consistently verified in both COVID-19 and non-COVID-19 situations. In other terms, our target are the gender mortality gap patterns, being characterized not only by their magnitude, but also by the age shape of the curves representing them. We thus capture the general shape of the relationship between male and female mortality rates as it evolves with age.
Such a study involves the choice of: (i) a graduation technique allowing to smooth raw mortality rates, namely to obtain rates progressing smoothly along ages while preserving the essential underlying mortality pattern, (ii) a reliable dataset of sex-specific mortality data, (iii) a proper measure of the gender gap in mortality.
The graduation method applied in this study has been previously validated (Navarro & Requena, 2023). It consists in fitting a cubic spline function to the logarithm of the sex-specific crude mortality rates for the age interval [1, 99] and the periods 2018–19, 2020, and 2021.
We use the data available in the Eurostat database concerning the male and female resident populations, by age, of France, Italy and Spain (i.e., census on January 1 of calendar years 2018, 2019, 2020, 2021 and 2022), as in Eurostat (2022a), and the data for the number of deaths occurred from 2018 to 2021 for these three populations, as in Eurostat (2022b). France, Italy and Spain are neighboring European countries, sharing similarities in many respects, when compared both at national and regional levels.Footnote 1 In light of their geographical proximity, the three countries under study, share similarities in environmental health, including climate, sanitation and hygiene conditions, and, as also stressed by Hettinger (2008), analogous historical experience, cultural heritages, religious values and lifestyles. Furthermore, their membership in the European Union ensures free movement of goods, services, capital and persons in a single EU internal market.Footnote 2 Sharing similarities in relation to important drivers of mortality, such nations may experience similarities in the age pattern of the gender gap in mortality likewise. We thus analyze empirically the distribution by age of the gender gap in mortality in calendar years with, and without, COVID-19 pandemic, to discuss possible stylized facts.
Our chosen measure of the gender gap in mortality is the ratio of graduated male to female mortality rates (“Gender Gap Ratio”, as in, e.g., Apicella et al. 2023), GGR from here onwards. Sex mortality ratios are widely studied across disciplines such as demography, social science and medicine (e.g., in Keyfitz 1985; Waldron 1993; Verbrugge et al. 2008; Costa and Victora 2021; Zarulli et al. 2021) and are simple to be interpreted. Quite simply, a GGR higher (lower) than 1 expresses a higher (lower) mortality for men than for women. If the GGR is equal to 1, this means perfect gender parity with respect to these probabilities.
Our paper adds to the existing literature by sheding light on the fundamental age pattern of the gender gap in mortality, smoothing out the irregularities arising from random variation, as revealed by continuous curves of the GGR.
We identify both stylized features and differences in the GGR behaviour by age across countries before and during the calendar years where the short-term implications on mortality of the COVID-19 pandemic were tangible, along with the enormous disruption that the pandemic have caused on many levels on human life and behaviours. In addition, it emerges an interesting aspect that in our opinion needs to be particularly highlighted: the GGR curve, entailing the underlying age pattern of the GGR, preserves its stilyzed shape, as observed in 2018–2019, also in the periods impacted by the COVID-19 pandemic. Our evidence shows important regularities by isolating age groups in which the GGR behaves absolutely similarly across the considered countries and periods.
2 Methods
2.1 Data
We use the data publicly available in the Eurostat database. In particular, we take the data, by age, on the male and female resident populations of France, Italy and Spain from “Population on 1 January by age and sex”, as in Eurostat (2022a). These data refer to the population censuses on 1 January 2018, 2019, 2020, 2021 and 2022. Furthermore, we use the data, by age, for the number of deaths that occurred from 2018 to 2021 for France, Italy and Spain, from “Deaths by age and sex”, as in Eurostat (2022b).
2.2 Crude mortality rates
The first step in this analysis is to calculate via standard actuarial techniques (see, e.g., Pitacco et al. 2009) the crude mortality rate for age x and period t, \({\hat{q}}_{x,t}\), for each population under study.
We denote by:
-
\(E_{x,t}\), time potentially lived by the resident population with age x last birthday during period t. It is the initial risk exposure, with \(x=\{1,\ldots ,99\}\) and \(t=2018-2019,2020,2021\),
-
\(\theta _{x,t}\), the number of deaths among the individuals, aged x last birthday in calendar year t, who reside in a given country,
-
\(P_{x,t^*}\), the population aged x last birthday on January 1, of year t (\(t^*\)=1st of January 2018,2019,2020,2021,2022), and residing in a given country.
If we assume that the deaths of the individuals aged x last birthday are uniformly distributed, the value of \(E_{x,t}\) can be approximated for 2018–19 as follows:
Similarly, for \(t=2020\) and \(t=2021\):
We assume that the total number of deaths of individuals aged x last birthday during observed period t is a random variable, \(\Theta _{x,t}\), distributed according to a binomial distribution of parameters \(E_{x,t}\) and \(q_{x,t}\), with \(q_{x,t}\) the unknown probability of dying before reaching age \(x+1\) for an individual of exact age x at period t:
Then \({\hat{q}}_{x,t}\), the crude mortality rate,
is an unbiased estimate of the probability \(q_{x,t}\), that is the actual mortality rate at age x and period t. In terms of its expected value it is equal to \(q_{x,t}\):
The variance of \({\hat{q}}_{x,t}\) is:
which depends on the unknown probability \(q_{x,t}\).
As in Forfar et al. (1988), we can approximate the variance of \({\hat{q}}_{x,t}\) by:
If \(E_{x,t}\) is sufficiently large, by the Central Limit Theorem we will assume that the distribution of \(\Theta _{x,t}\) can be approximated by a Normal random variable with mean \(E_{x,t} \cdot q_{x,t}\) and variance \(E_{x,t} \cdot q_{x,t}(1-q_{x,t})\).
Under the assumption that the observed crude mortality rate is one value from a Normal distribution with known variance given exactly by equation (7) (Forfar et al., 1988), we can approximate the confidence intervals for \(q_{x,t}\) as follows:
with \(z_\alpha =1.960\) for a confidence level of 95% and \(z_\alpha =2.576\) if the confidence interval is 99%.
2.3 Graduated mortality rates
The crude mortality rates are affected by the randomness of a stochastic phenomenon such as mortality, so they provide an irregular pattern of the actual mortality rates, which are assumed to vary smoothly with age. In order to eliminate part of the randomness of crude mortality rates as estimators of the actual probabilities of death, we proceed to the graduation of the mortality curve, which is a representation of mortality rates as a function of age. As mortality is considered a regular and continuous phenomenon in relation to age, we assume that the mortality curve should be a smooth function without significant deviations from the observed values.
Let \(y_{x,t}\) be the transformed crude mortality rates for ages \(x={1, \dots , 99}\) and calendar year t:
It can be assumed (see Forfar et al. 1988; Kaishev et al. 2016) that there is an unknown functional relationship between the mortality rates at each age (response variable \(y_{x,t}\)) and the age x, for each fixed calendar year t:
where \(\epsilon \) is a random error variable, with zero mean and \(\sigma ^2\) variance, and \(s_t(x)\) is an unknown function called mortality model. The \(s_t(x)\) function could be a formula such as Gompertz and Makeham laws (Forfar et al. 1988). Alternatively, it could be based on splines.
A spline function can be defined as a piecewise polynomial function (Forfar et al., 1988; McCutcheon, 1979; Pitacco et al., 2009). Let [a, b] an interval of real numbers and \(\xi _0,\xi _1,\dots ,\xi _m, \xi _{m+1}\) real numbers such that:
If we denote with \(s_t(x)\) the spline function, and \(p_0,p_1,\dots ,p_m\) the polynomials, the spline function is defined as follows:
The \(m+2\) numbers \(\xi _0, \xi _1, \dots , \xi _{m+1}\) are called the knots. In particular, \(\xi _1, \dots , \xi _{m}\) are the internal knots and \(\xi _0\) and \(\xi _{m+1}\) the boundary knots.
As regards the behaviour of \(s_t(x)\) in a neighbourhood of the generic knot \(\xi _h,h=1,\dots ,m\), a measure of smoothness is provided by the maximum order of the derivative of the polynomials such that the polynomials \(p_{h-1}\) and \(p_h\) have common derivative values at \(\xi _h\).
When all polynomials have degree at most r, the spline is of degree r. A spline of degree 3 is a cubic spline. It can be proved that, for a given interval [a, b] and a given set of internal knots, the set of splines of degree r constitutes a vector space of dimension \(d=m+r+1\). Then any basis for this space consists of d elements.
We denote by \(B_1^r, B_2^r, \dots , B_d^r\) a basis of degree r. Hence, any spline \(s_t(x)\) in this vector space can be represented as a linear combination of these functions,
where the coefficients \(\beta =(\beta _1, \dots , \beta _d)\) are uniquely determined by the function s.
The spline function \(s_t(x)\) is a flexible smooth function. There is a trade-off between fit and roughness of the function. Accordingly, increasing the number of knots may overfit the data and increase the variance (the graduated function follows the data randomness and not the underlying tendency), whilst decreasing the number of knots may result in a rigid and restrictive function that has more bias. The high flexibility of spline modelling comes at the price of a few tuning parameters like the degree r of the underlying polynomials, the choice of the basis functions and the number of spacing of the knots.
For futher details about spline functions and their properties see (de Boor, 1978; Wold, 1974; Wand, 2000; Dodd et al., 2018; Perperoglou et al., 2019).
In this research, we use cubic splines, that is, the polynomials are of degree 3. They must be functions of class \(C^2\) at all knots, that is twice differentiable at \(\xi _h\), with \(h=1,\dots ,m\). The option chosen for the basis functions \(B_i^r(x)\) is the B-Spline basis of degree 3 because of its numerical advantages and stability. The algorithm for the construction of the basis functions is from de Boor (1978). It is included in the R (https://www.r-project.org/) package “splines” from Bates and Venables (Bates & Venables, 2016) and in the R package “splines2” as in Wang and Yan (2021). For our application, we use package “splines”.
The knots are points where the function makes a transformation. The number of internal knots of the spline suggested by McCulloch (1971) is \(\sqrt{N}-2\), with N being the number of available observations which in this case is 99. Our statistical analysis on cubic splines with different internal knots leads to the choice of 9 internal knots plus two boundary knots. Given the irregular behaviour of the mortality curve at the beginning and at the end of the curve, the number of observations to the left of \(\xi _1\) and to the right of \(\xi _9\) will be half that between the rest of the inner knots. We set inner knots at ages 5.56, 16.67, 27.78, 38.89, 50, 61.11, 72.22, 83.33, 94.44 and the boundary knots at ages 1 and 99.
For each period t, the coefficients of the spline function minimize the objective function:
For each period t, the number of parameters for estimating is \(d=9+3+1\). We do not apply any penalty about the variability of the coefficients \(\beta _i, i=1,\dots ,13\) because we are more interested in the fidelity of the graduated values to the observed ones, as opposed to the smooth behaviour of the graduated values.
The results of the parameter estimates of spline functions used for the graduation of mortality rates of French, Italian and Spanish male and female populations, and the periods 2018–19, 2020 and 2021, are presented in the Appendix, in Table 2.
We denote by \({\tilde{y}}_{x,t}\) the logarithmic death rate resulting from the graduation, as follows:
Accordingly, it holds that:
In the Appendix, in Figs. 3, 4 and 5, we compare graduated log mortality rates \({\tilde{y}}_{x,t}\) against crude log mortality rates \(y_{x,t}\), for the populations of France, Italy and Spain, respectively. In all Figures, the left panel refers to females for the periods 2018–2019, 2020 and 2021 (from top to bottom). The right panel refers to males with respect to the same country and time period.
To assess whether the graduated mortality rates are a reasonable representation of the mortality model of each population, we evaluate the goodness of fit at individual ages by a battery of tests. Following Macdonald et al. (2018), for testing the overall fit of the mortality model we use the standardised deviations test, which tests the normality and independence of the residuals; for testing the bias of the model (balance between positive and negative values of the residuals) we use the bias or signs test. Furthermore, for testing the under or overestimation of mortality rates over ranges of ages we use the runs test. The null hypothesis is the adequacy of the model, that is, the model captures the structure of the population mortality. We select a test statistic whose behaviour is known. When it has a p-value greater than the significance level \(\alpha \), the null hypothesis is accepted because the data do not contradict the null hypothesis. In Table 3 in the Appendix, we report the p-values for countries, male and female population and period. From a statistical point of view, the results we obtain from the tests (p-values greater than 0.05 or 0.01) support the acceptance of the model as representing the underlying mortality of the different populations.
2.4 Gender gap ratio
For a given population, let \({\tilde{q}}^{F}_{x,t}\) be the graduated female mortality rate for age x and year t and \({\tilde{q}}^{M}_{x,t}\) the graduated male mortality rate for the same age and year. The Gender Gap Ratio for age x and year t, i.e., \(GGR_{x,t}\) is defined as follows:

Age patterns of the Gender Gap Ratio in 2018–2019, 2020 and 2021. We display a total of three GGR curves, one for time period, for France (top), Italy (middle) and Spain (bottom). Each curve associates a GGR value to an age in the interval [1, 99]
3 Results
In this Section, we show graphical evidence about the age pattern of the GGR, that is obtained as the ratio of male to female graduated mortality rates.
In Fig. 1, we show the age patterns of the Gender Gap Ratio in 2018/2019, 2020 and 2021, for France (top), Italy (middle) and Spain (bottom). We remark that we aggregate the mortality data relative to calendar years 2018 and 2019; accordingly, one estimate of the GGR summarizes the sex mortality ratio experienced by a given age over the two years. For each country, we display a total of three curves of the GGR, i.e., one per year, each associating a GGR value to an age in the interval [1, 99].
Figure 1 allows cross-country comparisons across two dimensions: (i) magnitude of the GGR and its change during the two different COVID-19 calendar years; (ii) stylized shape of the GGR curve, namely the distinctive age pattern of the GGR being consistently verified across countries and time. In this respect, in each panel, the orange area, encompassing the GGR curves in the calendar years under investigation, ideally portrays a unifying curve of the GGR’s behaviour and describes, under a novel perspective, the peculiar age profile of the gender gap in mortality.

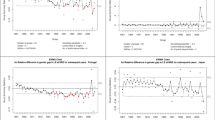
Percent change experienced by the Gender Gap Ratio between 2018/2019 and 2020 (Panel A) and between 2020 and 2021 (Panel B). Integer ages in the range [1, 99] (x-axis). France, Italy and Spain
The magnitude of the GGR differs by country, although there is no a sharp and consistent dominance, over all ages, of a nation over the others. This evidence is summarized by Table 1, where we report the GGR, relative to our benchmark time period 2018/2019, averaged over the nine 10-years age intervals between ages 1 and 90, and the 9-years age range [91, 99]. The cross-country difference in the magnitude of the GGR, the age interval being equal, ranges between \(3\%\) (age range [1, 10]) and \(27\%\) (age range [61, 70]). Among the three countries, while France has experienced the highest GGR, on average, for the ages between 21 and 50 and for post-80 ages, Spain has been characterized by the largest GGR in between.
This paper uncovers novel evidence about the existence of a consistent age profile of the gender gap in mortality. Capturing the age pattern of the gender gap in mortality represents a significant step for a proper quantitative description of such a phenomenon and has important implications for scientists in many fields, e.g., in the context of social insurance and health public policy. For instance, detecting the stylized dynamics of the gender gap in mortality over age is a significant step toward the construction and interpretability of mathematical models for the projection of this phenomenon into the future.
In our opinion, one of the most relevant and interesting evidence we uncover in this paper is that the GGR’s evolution over age follows, for all the nations under study, the same pattern, consisting in a systematic interchange between increasing and decreasing trends within specific age intervals. In other terms, the GGR has an almost stylized shape, with distinct age-specific components, in terms of its slope and curvature.
Indeed, when we focus on the GGR as a continuous age-dependent curve, in Fig. 1, we notice that, in the benchmark time period, the GGR attains its highest and lowest values, graphically appearing as local maximizers and minimizers, at ages being remarkably close to each other for the countries under study. The ages marking the points of largest magnitude in the GGR curve are in the ranges [2, 3], [24, 27], and [65, 69]. The ages connoting the points of smallest magnitude in the GGR curve are in the ranges [7, 8] and [42, 47], and at age 98 for France.
The COVID-19 pandemic disease in years 2020 and 2021 has only mildly changed the described shape, through either very moderate shifts, backward or forward in age, of the detected local maximizers and minimizers, or by restricting the age intervals at which these extreme points occur. For instance, in 2020 the GGR attained its highest values in the three countries within the age ranges [24, 25] and [66, 69], and, in France and Spain, also in [3, 4]. In 2021, in all the countries under study, the GGR’s highest values occurred in the age intervals [3, 4], [24, 27] and [66].
Furthermore, the GGR curve declines almost linearly toward the value of 1 with advancing age. Such characteristic is preserved despite the pandemic.
4 Discussion
The COVID-19 pandemic caused a remarkable rise in mortality implying life expectancy losses worldwide, with very few exceptions. Several studies have quantified the mortality burden of COVID-19 under a cross-national perspective and with a focus on the age profile of such a pandemic. COVID-19 mortality reveals stylized features and its age patterns exemplify such a systematic behaviour. For instance, in Goldstein and Lee (2020) it is shown that the age pattern of deaths, when appropriately adjusted, is analogous across a wide variety of countries and resembles the age pattern of all-cause mortality. Furthermore, empirical research has addressed the COVID-19 mortality at different stages of the epidemic, e.g., in 2020 and in 2021. For instance, Schöley et al. (2022) show that although younger age groups in 2021 contributed more largely to excess mortality than in 2020, increased mortality in ages 60+ kept representing the major contributor to life expectancy losses compared with pre-pandemic levels in 19 out of the 28 countries under study. It is also well-established that males were overall more affected by excess deaths than women.
Our research question addresses if and to which extent the gendered and age-dependent pattern of COVID-19 mortality have induced an enduring and structural change in the age-dependent shape of the GGR curve, despite shocks impacting on its slope and curvature during the pandemic.
In Panel A of Fig. 2, we display, on the y-axis, the percent change experienced by the GGR in 2020 with respect to its magnitude in 2018/2019, for each integer age in the range [1, 99] (x-axis), for France (red), Italy (green) and Spain (light blue). The age-dependent pattern of COVID-19 mortality reverberates on the gender gap, thus implying age-specific effects on the GGR. The heterogeneity over age is remarkably large for Spain, being characterized by the highest dispersion around the average percent change recorded for this nation (i.e. around 112% variance against around 30% for France).
A systematic GGR’s behaviour across countries cannot be observed, in terms of both the magnitude and the direction of its change in 2020. In this respect, only the age intervals [38, 47] and [77, 88] are consistently characterized by an increase of the GGR, with differences in the magnitude of such a positive change. Instead, the ages 1 and 99 and the age interval [28, 33] are systematically characterized by a fall in the GGR in 2020. At age 30, we observe the smallest between-country difference in the amplitude of the GGR’s decrease (i.e., downward changes ranging from \(-\)3.2% to \(-\)4.4%). At age 86, we see the smallest between-country discrepancy in the magnitude of the GGR’s increase (i.e., upward changes ranging from 0.5% to 1.7%).
Out of the mentioned age ranges, especially below age 40, countries differ up to 65 percent points (i.e., age 3) in the experienced GGR’s variation.
On January 30, 2020 the WHO Director General declared that the outbreak of novel coronavirus constituted a Public Health Emergency of International Concern (WHO & Global Research Collaboration for Infectious Disease Preparedness, 2020). Governments across the world played a major role in responding to the COVID-19 by implementing measures to contain the spread of the novel coronavirus and to prepare for future outbreaks, e.g. strict isolation and lockdown protocols (Colfer, 2020). Such measures had effects on several risk factors associated with mortality (e.g., treatment of chronic diseases, air quality, nutrition security). Furthermore the preventive and containment measures differed by the inception time and the duration of their implementation and by their severity, also based on the country-specific political attitudes and risk perception (e.g., Legido-Quigley et al. 2020; Sebastiani et al. 2020; Roux et al. 2023). The heterogeneous age effects of the COVID-19 on the GGR may arise from the diverse governments policies being implemented throughout 2020, whereas the systematicity of the increase (decrease) of the GGR over specific age intervals may reveal a more structural COVID-19 effect on the age profile of the gender gap in mortality. Consistent empirical evidence documents gender differences in mortality and vulnerability due to the COVID-19 disease, with a higher number of COVID-19-related deaths being reported for males than for females worldwide. Nevertheless, as stressed by Nielsen et al. (2021), the resulting sex-difference in all-cause mortality may not represent a peculiar feature of the COVID-19 pandemic, but it may otherwise reflect a general sex-disparity in excess mortality, being verified in none-COVID-19 situations likewise. For instance, greater excess mortality for males than for females was also observed in season 2017/18 because of influenza and was comparable to the cumulated sex-difference in excess mortality during the COVID-19 pandemic, in terms of magnitude. We thus investigate the GGR changes occurred between 2020 and 2021. We deem this further study particularly relevant for the age intervals where the GGR experienced a rise in 2020, due to the effects on retirement planning and on cross-subsidisation within pension schemes. As stressed by Barigozzi et al. (2023), the gender issues underlying the ongoing debates about pension reforms still lack a strong attention and a proper understanding. For instance, areas where a more extensive guidance would be needed relate to the “direction” and extent of redistribution between men and women and to the consequences of the gender neutrality rules of pension schemes for pension design, retirement ages and cross-subsidisation. Furthermore, current debates argue that more attention should be also placed on the gender dimensions of disease outbreaks (Smith, 2019), e.g., in response to the coronavirus disease 2019 (COVID-19), as an important step to assess the effects of health emergencies and inform equitable policies and interventions (e.g., Wenham et al. 2020, Flor et al. 2022).
In Panel B of Fig. 2, we display, on the y-axis, the percent change experienced by the GGR in 2021 with respect to its magnitude in 2020, for each integer age in the range [1, 99] (x-axis), for France (red), Italy (green) and Spain (light blue). We observe that in 2021 the GGR consistently increased, across countries, throughout the age intervals [24, 42] and [90, 95]. We remind that, for the ages between 28 and 33, the GGR suffered, instead, from a downward change in the previous year. Furthermore, in 2021 the GGR related to the age interval [68, 79] has consistently decreased in all the countries under study. Almost the same age interval, instead, in 2020 experienced a rise in the GGR in France and Italy, and a mild negative change (\(-\)0.28% on average) for Spain. Accordingly, for some age ranges, upward (downward) COVID-19 effects in 2020 were counterbalanced, at least partially, by GGR’s changes in the opposite direction in 2021. If, for instance, we focus on the age interval [68, 79], we notice that, on average over age and country, the GGR increased by 2.24% in 2020 and decreased by 2.70% in 2021.
Although the COVID-19 has triggered changes in the magnitude of the GGR in 2020 and in 2021, we conclude that the age profile of the gender gap in mortality, i.e., how the GGR evolves over age, has not been overall impacted. Indeed, in Fig. 1, we see how the GGR curve in 2021, entailing the underlying age pattern of the GGR, preserved its stilyzed shape, as observed in 2019. This is a further very relevant result in our paper, corroborating the findings about the age pattern of the gender gap in mortality shown in the previous Section. Furthermore, such an evidence is novel, since previous literature mainly focuses on the systematic age pattern of mortality rates, rather than of a sex ratio. Indeed, the attention of scientists in many fields has focused on the relationship between mortality and age. Several attempts have been made to describe mortality curves by means of simple biologically interpretable mathematical models allowing to reproduce the peculiar age pattern of human mortality (see, e.g., Gompertz 1825; Makeham 1867; Heligman and Pollard 1980, and Forfar 2006 for a review). Following the progress in medicine and science during the 20th century, further contributions have developed realistic models to properly describe the shape of the human mortality curve and thus the overall mortality behaviour by age ranges (e.g., Lai 2012; Weon and Je 2012; da Rocha and Espíndola 2020), especially in relation to the mortality data of developed countries, that have more dramatically entered an era of demographic transition intersecting with various aspects of economic activity (Papapetrou & Tsalaporta, 2020). Such models aim to capture some stylized features of mortality behaviour being verified, across countries and time, net of the variation due to the global increase in life expectancy. Our paper, instead, captures stylized features of the gender mortality gap behaviour over age being verified, across countries, net of the variations caused by the COVID-19 impact.
References
Apicella, G., De Giorgi, E.G., Di Lorenzo, E., & Sibillo, M. (2023). Gender-Inclusive Financial and Demographic Literacy: Lessons from the Empirical Evidence. Swiss Finance Institute Research Paper No. 23-02. https://doi.org/10.2139/ssrn.4331841.
Atance, D., Balbás, A., & Navarro, E. (2020). Constructing dynamic life tables with a single-factor model. Decisions in Economics and Finance, 43(2), 787–825. https://doi.org/10.1007/s10203-020-00308-5
Bambra, C., Albani, V., & Franklin, P. (2021). Covid-19 and the gender health paradox. Scandinavian Journal of Public Health, 49(1), 17–26. https://doi.org/10.1177/1403494820975604
Barigozzi, F., Cremer, H., & Lozachmeur, J.-M. (2023). Gender wage and longevity gaps and the design of retirement systems. Journal of Economic Behavior & Organization, 209, 263–287. https://doi.org/10.1016/j.jebo.2023.03.007
Bates, D.M., & Venables, W.N. (2016). Regression spline functions and classes. R Package splines.
Chen, C., Maung, K., & Rowe, J. W. (2021). Gender differences in countries’ adaptation to societal ageing: an international cross-sectional comparison. The Lancet Healthy Longevity, 2(8), E460–E469. https://doi.org/10.1016/S2666-7568(21)00121-5
Colfer, B. (2020). Public policy responses to COVID-19 in Europe. European Policy Analysis, 6(2), 126–137. https://doi.org/10.1002/epa2.1097
Costa, J. C., & Victora, C. G. (2021). A scoping review of methods for assessment of sex differentials in early childhood mortality. BMC Pediatrics 21(55). https://doi.org/10.1186/s12887-021-02503-8
Currie, I. D., Durban, M., & Eilers, P. H. (2004). Smoothing and forecasting mortality rates. Statistical Modelling, 4(4), 279–298. https://doi.org/10.1191/1471082X04st080oa
da Rocha, A. M., & Espíndola, A. L. (2020). Mortality curves using a bit-string aging model. Physica A: Statistical Mechanics and its Applications, 560, 125134. https://doi.org/10.1016/j.physa.2020.125134
de Boor, C. (1978). A practical guide to splines. Springer.
Dodd, E., Forster, J., Bijak, J., & Smith, P. (2018). Smoothing mortality data: the English Life Tables, 2010–2012. J. R. Statist. Soc. A, 181(3), 717–735.
Eurostat. (2022a). Population on 1 January by age and sex. URL https://ec.europa.eu/eurostat/databrowser/view/DEMO_PJAN/default/table?lang=en.
Eurostat. (2022b). Deaths by age and sex. URL https://ec.europa.eu/eurostat/databrowser/view/DEMO_MAGEC/default/table?lang=en.
Feraldi, A., & Zarulli, V. (2022). Patterns in age and cause of death contribution to the sex gap in life expectancy: A comparison among ten countries. Genus. https://doi.org/10.1186/s41118-022-00171-9
Flor, L. S., Friedman, J., Spencer, C. N., Cagney, J., Arrieta, A., Herbert, M. E., Stein, C., Mullany, E. C., Hon, J., Patwardhan, V., Barber, R. M., Collins, J. K., Hay, S. I., Lim, S. S., Lozano, R., Mokdad, A. H., Murray, C. J. L., Reiner, R. C., Sorensen, R. J. D., Haakenstad, A., Pigott, D. M., & Gakidou, E. (2022). Quantifying the effects of the COVID-19 pandemic on gender equality on health, social, and economic indicators: A comprehensive review of data from March, 2020, to September, 2021. The Lancet, 399(10344), 2381–2397. https://doi.org/10.1016/S0140-6736(22)00008-3
Forfar, D. O. (2006). Mortality laws. Wiley. https://doi.org/10.1002/9780470012505.tam029
Forfar, D. O., McCutcheon, J. J., & Wilkie, A. D. (1988). On graduation by mathematical formula. Journal of the Institute of Actuaries (1886-1994), 115(1), 1–149. http://www.jstor.org/stable/41140871.
Franklin, P., Bambra, C., & Albani, V. (2021). Gender equality and health in the EU. in European Commission, Directorate-General for Justice and Consumers, Publications Office, https://doi.org/10.2838/991480.
Goldstein, J. R., & Lee, R. D. (2020). Demographic perspectives on the mortality of COVID-19 and other epidemics. PNAS, 117(36), 22035–22041. https://doi.org/10.1073/pnas.2006392117
Gompertz, B. (1825). On the nature of the function expressive of the law of human mortality, and on a new mode of determining the value of life contingencies. Philosophical Transactions of Royal Society of London, 115, 513–583.
Heligman, L., & Pollard, J. H. (1980). The age pattern of mortality. Journal of the Institute of Actuaries (1886-1994), 107(1), 49–80.
Hettinger, L. (2008). France, Italy, and Spain: Culturally Similar Nations, Yet Drastically Different In Their Roles as European Union Nations. Honors Scholar Theses. 52. https://opencommons.uconn.edu/srhonors_theses/52.
Kaishev, V. K., Dimitrova, D. S., Haberman, S., & Verrall, R. J. (2016). Geometrically designed, variable knot regression splines. Computational Statistics, 31, 1079–1105. https://doi.org/10.1007/s00180-015-0621-7
Keyfitz, N. (1985). Applied Mathematical Demography, chapter Mortality Comparisons; The male-female ratio. Springer, https://doi.org/10.1007/978-1-4757-1879-9_3.
Lai, C. D. (2012). Human mortality curves that decelerate to a plateau. Mathematical and Computer Modelling, 55(3–4), 1118–1128. https://doi.org/10.1016/j.mcm.2011.09.036
Legido-Quigley, H., Mateos-García, J. T., Campos, V. R., & Gea-Sánchez, M. (2020). The resilience of the Spanish health system against the COVID-19 pandemic. The Lancet Public Health, 5(5), E251–E252. https://doi.org/10.1016/S2468-2667(20)30060-8
Luoma, A., Puustelli, A., & Koskinen, L. (2012). A Bayesian smoothing spline method for mortality modelling. Annals of Actuarial Science, 6(2), 284–306. https://doi.org/10.1017/S174849951200005X
Macdonald, A.S., Richards, S.J., & Currie, I. (2018). Modelling mortality with actuarial applications. International Series on Actuarial Science. Cambridge University Press, https://doi.org/10.1017/9781107051386.
Makeham, W. M. (1867). On the Law of Mortality. Journal of the Institute of Actuaries, 13(6), 325–358.
McCulloch, J. H. (1971). Measuring the term structure of interest rates. The Journal of Business, 44(1), 19–31.
McCutcheon, J. J. (1979). Some remarks on splines. Transactions of the Faculty of Actuaries, 37, 421–438. https://doi.org/10.1017/S0071368600008727
McCutcheon, J. J. (1985). Experiments in graduating the data for the English life tables (No.14). Transactions of the Faculty of Actuaries, 40, 135–147. http://www.jstor.org/stable/41218919.
Navarro, E., & Requena, P. (2023). Impact of COVID-19 on Spanish mortality rates in 2020 by age and sex. Journal of Public Health, 45(3), 577–583. https://doi.org/10.1093/pubmed/fdad023
Nielsen, J., Nørgaard, S. K., Lanzieri, G., Vestergaard, L. S., & Moelbak, K. (2021). Sex-differences in COVID-19 associated excess mortality is not exceptional for the COVID-19 pandemic. Scientific Reports 11(20815). https://doi.org/10.1038/s41598-021-00213-w
Papapetrou, E., & Tsalaporta, P. (2020). The impact of population aging in rich countries: What’s the future? Journal of Policy Modeling, 42(1), 77–95. https://doi.org/10.1016/j.jpolmod.2019.12.002
Perperoglou, A., Sauerbrei, W., Abrahamowicz, M., & Schmid, M. (2019). A review of spline function procedures in R. BMC Medical Research Methodology 19(46). https://doi.org/10.1186/s12874-019-0666-3
Pitacco, E., Denuit, M., Haberman, S., & Olivieri, A. (2009). Modeling longevity dynamics for pensions and annuities. Oxford University Press.
Roux, J., Massonnaud, C. R., Colizza, V., Cauchemez, S., & Crépey, P. (2023). Modeling the impact of national and regional lockdowns on the 2020 spring wave of COVID-19 in France. Scientific Reports, 13 (1834), 2023. https://doi.org/10.1038/s41598-023-28687-w
Schöley, J., Aburto, J. M., Kashnitsky, I., Kniffka, M. S., Zhang, L., Jaadla, H., Dowd, J. B., & Kashyap, R. (2022). Life expectancy changes since COVID-19. Nature Human Behaviour, 6, 1649–1659. https://doi.org/10.1038/s41562-022-01450-3
Sebastiani, G., Massa, M., & Riboli, E. (2020). COVID-19 epidemic in Italy: Evolution, projections and impact of government measures. European Journal of Epidemiology, 35, 341–345. https://doi.org/10.1007/s10654-020-00631-6
Simba, H., & Ngcobo, S. (2020). Are pandemics gender neutral? Women’s health and COVID-19. Frontiers in Global Women’s Health 1(570666). https://doi.org/10.3389/fgwh.2020.570666
Smith, J. (2019). Overcoming the ‘tyranny of the urgent’: Integrating gender into disease outbreak preaparedness and response. Gender & Development, 27(2), 355–369. https://doi.org/10.1080/13552074.2019.1615288
Sundberg, L., Agahi, N., Fritzell, J., & Fors, S. (2018). Why is the gender gap in life expectancy decreasing? the impact of age-and cause-specific mortality in Sweden 1997–2014. International Journal of Public Health, 63, 673–681.
Tang, S., Li, J., & Tickle, L. (2023). A Hermite spline approach for modelling population mortality. Annals of Actuarial Science, 17(2), 243–284. https://doi.org/10.1017/S1748499522000173
van der Linde, A., Witzko, K.-H., & Jockel, K.-H. (1995). Spatial-Temporal Analysis of Mortality Using Splines. Biometrics, 51(4), 1352–1360. https://doi.org/10.2307/2533266
Verbrugge, L. M., Wingard, D. L., & Features Submission, H. C. (2008). Sex differentials in health and mortality. Women & Health, 12(2), 103–145. https://doi.org/10.1300/J013v12n02_07
Waldron, I. (1993). Recent trends in sex mortality ratios for adults in developed countries. Social Science & Medicine, 36(4), 451–462. https://doi.org/10.1016/0277-9536(93)90407-U
Wand, M. P. (2000). A comparison of regression spline smoothing procedures. Computational Statistics, 15, 443–462.
Wang, W., & Yan, J. (2021). Shape-restricted regression splines with R package splines2. Journal of Data Science, 19(3), 498–517.
Wenham, C., Smith, J., & Morgan, R. (2020). COVID-19: The gendered impacts of the outbreak. The Lancet, 395(10227), 846–848. https://doi.org/10.1016/S0140-6736(20)30526-2
Weon, B. M., & Je, J. H. (2012). Trends in scale and shape of survival curves. Scientific Reports 2 (504). https://doi.org/10.1038/srep00504
WHO and Global Research Collaboration for Infectious Disease Preparedness. COVID-19 Public Halth Emergency of International Concern (PHEIC). Global research and innovation forum: towards a research roadmap, (2020). URL https://www.who.int/publications/m/item/covid-19-public-health-emergency-of-international-concern-(pheic)-global-research-and-innovation-forum.
Wold, S. (1974). Spline functions in data analysis. Technometrics, 16(1), 1–11.
Zarulli, V., Kashnitsky, I., & Vaupel, J. W. (2021). Death rates at specific life stages mold the sex gap in life expectancy. PNAS, 118(20), e2010588118.
Funding
Open access funding provided by Università degli Studi di Udine within the CRUI-CARE Agreement.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix A: Additional notes on the numerical results from graduation
Appendix A: Additional notes on the numerical results from graduation

Crude (red dots) and graduated (blue lines) log mortality rates for French females and males in the periods 2018/19, 2020 and 2021 (displayed from top to bottom, respectively). Left Panel: females, right panel: males. The vertical dashed lines indicate the internal knots of the cubic splines
In this Section, in Figs. 3, 4 and 5, we compare graduated mortality rates (blue lines) against crude mortality rates (red dots), for the populations of France, Italy and Spain, respectively. In all Figures, the left panel refers to females for the periods 2018–2019, 2020 and 2021 (from top to bottom). The right panel refers to males with respect to the same country and time period.
Furthermore, in Table 2, we report the results of the parameter estimates of spline functions used for the graduation of mortality rates.
To assess whether the graduated mortality rates are a reasonable representation of the mortality model of each population, we evaluate the goodness of fit at individual ages by a battery of tests. Following Macdonald et al. (2018), for testing the overall fit of the mortality model we use the standardised deviations test, which tests the normality and independence of the residuals; for testing the bias of the model (balance between positive and negative values of the residuals) we use the bias or signs test. Furthermore, for testing the under or overestimation of mortality rates over ranges of ages we use the runs test. In Table 3, we report the p-values for the countries we consider, the male and female populations and the time periods under study. From a statistical point of view, the results we obtain from the tests (p-values greater than 0.05 or 0.01) support the acceptance of the model as representing the underlying mortality of the different populations.

Crude (red dots) and graduated (blue lines) log mortality rates for Italian females and males in the periods 2018/19, 2020 and 2021 (displayed from top to bottom, respectively). Left Panel: females, right panel: males. The vertical dashed lines indicate the internal knots of the cubic splines

Crude (red dots) and graduated (blue lines) log mortality rates for Spanish females and males in the periods 2018/19, 2020 and 2021 (displayed from top to bottom, respectively). Left panel: females, right panel: males. The vertical dashed lines indicate the internal knots of the cubic splines
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Apicella, G., Navarro, E., Requena, P. et al. The age pattern of the gender gap in mortality: stylized evidence across COVID-19 pandemic times. Ann Oper Res (2024). https://doi.org/10.1007/s10479-024-06068-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10479-024-06068-4