
Abstract
Aim
The study was conducted to evaluate the knowledge levels of sexually active individuals about Human Papilloma Virus (HPV), HPV screening test, and HPV vaccine and raise awareness.
Subject and methods
A cross-sectional descriptive design was adopted. The data were completed with 150 sexually active participants between the ages of 18–49. The “Personal Information Form” and “HPV Knowledge Scale” were used to collect data. The data were collected on the online platform via Google Surveys using snowball sampling between September 19 and October 19, 2022.
Results
The average sexual age of the participants was 21.16 ± 2.2 years for women and 21.16 ± 2.2 years for men. The education levels of the participants were 47 (62.66%) of the women and 56 (74.66%) of the men, respectively, university graduates, and 58 (77.33%) of the women and 66 (88.00%) of the men stated that they were public employees. It was found that the average HPV Knowledge Scale (HPV-KS) score of the participants was 16.09 ± 6.11 in women and 12.26 ± 6.34 in men, respectively, and the level of HPV knowledge in women was significantly higher than in men (p = 0.017). Women were determined to be more knowledgeable about HPV vaccine administrations than men, which was statistically significant (p = 0.003). However, men were revealed to be administered more HPV vaccines than women, and the result was statistically significant (p = 0.042). The analysis revealed a statistically significant difference between knowledge scores between those who had received the vaccine and those who had not and HPV awareness (p = 0.000).
Conclusion
The results indicated that individuals who had their first sexual experience at an earlier age and possessed a higher level of education were more likely to be receptive to the HPV vaccine.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Human Papilloma Virus (HPV) is a double-stranded, non-enveloped DNA virus (Della Fera et al. 2021). There are different types of HPV, and Types 6, 11, 16, 18, 31, 33, 45, 52, and 58 lead to high rates of cervical cell abnormalities and anogenital cancers (Meites et al. 2021; Akalın 2022). In the transmission of HPV, individuals who are sexually active and individuals with polygamous sexual partnerships are at risk. Experiencing the first sexual intercourse at an early age and not knowing the contraception methods increase the likelihood of contracting the virus (Çevik and Coskun 2021). Vaccination is the most effective way to be protected against HPV (Meites et al. 2021). The United States Food and Drug Administration (FDA) has approved three HPV vaccines (Cervarix, Gardasil, and Gardasil 9), which prevent infections caused by high-risk HPV genotypes in all men and women between the ages of 9–26 (FDA 2015, 2016, 2018). Secondary protection involves protection measures such as screening and early diagnosis with HPV-DNA test and Pap test (Andiwijaya et al. 2022). In the study examining the HPV knowledge levels of midwifery and nursing undergraduate students in Turkey, it was determined that female students scored significantly higher than male students in the sub-dimensions of HPV test information questions and HPV vaccine information questions (Güllü 2023). Upon reviewing the literature, it was found that the level of knowledge about HPV, HPV screening tests, and HPV vaccine had not been examined in sexually active individuals in Turkish society. This study aimed to evaluate the knowledge levels of sexually active individuals about HPV, HPV screening test, and HPV vaccine and raise awareness. For this purpose, answers were sought to the following questions;
-
What is the level of knowledge of individuals in Turkey about HPV?
-
What is the HPV vaccination status of individuals in Turkey?
Method
Design and participants
It is a descriptive trial. The STROBE checklist was used during the writing phase of the study. The study population consisted of sexually active individuals between the ages of 18-49. The sample size was calculated with a 0.05 margin of error and 80% power using the G-Power (3.1.9.2) program. Assuming that the evaluations would have a moderate effect size, it was revealed that there should be at least 64 individuals in groups in line with the calculation made using the F test. The study was carried out with 150 participants, 75 men and 75 women, who were sexually active, had no education in the field of health, had no professional experience, had at least a primary school diploma, between the ages of 18-49 and had internet access and usage knowledge. The data were collected on the online platform via Google Surveys using snowball sampling between September 19 and October 19, 2022.
Instruments
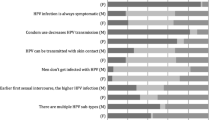
The “HPV Knowledge Scale” and the “Personal Information Form” prepared in line with the literature were used to obtain the data. A literature review was conducted to develop a Personal Information Form. This form included 12 questions about the socio-demographic characteristics and sexual histories of the participants, which were then administered (Kops et al. 2019). HPV Knowledge Scale (HPV-KS) developed by Waller et al. comprises a total of 35 items and four sub-sections that measure the level of knowledge about HPV, HPV vaccine, and screening tests (Waller et al. 2013). The Turkish validity and reliability study of the scale was performed by Demir (2019), and two items of the scale were excluded. The final version of the scale consists of 33 items and 4 sub-sections. The highest score to be obtained from the scale is 33 and the lowest score is 0. A high score indicates a high level of knowledge about HPV. There are four sub-sections in the scale. In the first section, there are sixteen questions under the preliminary question, “Have you ever heard of HPV?” In the second section, there are six questions under the preliminary question, “Have you ever heard of HPV testing?” In the third section, there are five questions under the preliminary question, “Have you ever heard of the HPV vaccine?” There are no preliminary questions to answer the questions in the independent section, which is the fourth section, there are six questions, and it is mandatory for all participants to answer them. There are a total of 33 questions on the scale. When the preliminary questions in the first, second, and third sections are answered as “Yes”, the questions under these sections are answered. When the preliminary questions in the first, second, and third sections are answered “No”, the questions under these sections are not answered, and the participants automatically proceed to the next section. Only in the fourth section, there are no preliminary questions, and it is mandatory for all participants to answer the questions. On the scale, 1 point is received for each correct answer, and 0 points are received for incorrect and “I don’t know” answers. The lowest score to be received from the scale is 0, and the highest score is 33. The increase in the score received from the scale indicates that the level of knowledge about HPV screening tests and the HPV vaccine is high. There are no reverse items in the scale (Demir 2019).
Data analysis
Quantitative analysis techniques were employed for statistical evaluation. For statistical evaluation, percentage, mean, standard deviation, the chi-square, and Mann–Whitney U test were used along with the SPSS for 24 version program. The analysis results were evaluated at a significance level of p < 0.05.
Results
Socio-demographic characteristics
Table 1 contains considering the participants’ age, it is observed that 50.7% of women and 52.0% of men are between the ages of 18–30, and the mean ages of the groups are similar (p = 0.949). The mean age at first sexual intercourse was 20.73 ± 3.83 in males and the mean age at first sexual intercourse was at least 15 years. In females, the minimum age at first sexual intercourse was 16 years, the mean age at first sexual intercourse was 24.21 ± 3.83 years and a significant difference was found between the groups (p = 0.000). Concerning educational status, 62.6% of women and 74.7% of men had bachelor’s degrees. 88.0% of male participants and 77.3% of female participants were public employees. 20% of women are housewives. 54.66% of women and 57.33% of men stated that they were protected by the barrier method. It was revealed that 3.4% of women and 13.3% of men had HPV vaccination, and there was a statistically significant difference between them (p = 0.042, p < 0.05).
HPV-KS mean scores by sex
In Table 2 upon comparing the HPV-KS sub-section mean scores, a statistically significant difference was determined between the knowledge levels of women about HPV test and HPV vaccine administrations compared to men. The mean score of the HPV test knowledge questions was 1.97 ± 1.71 for women and 0.96 ± 1.01 for men, and the difference between them was statistically significant (p = 0.017). The mean score of the HPV vaccine availability items was 0.92 ± 1.29 for women and 0.38 ± 0.80 for men, and the difference between them was statistically significant (p = 0.003). The mean score of general HPV knowledge was 8.44 ± 3.52 in women and 7.08 ± 4.27 in men; HPV vaccine knowledge questions was 2.26 ± 1.18 in women and 2.11 ± 1.45 in men; the total score was 16.09 ± 6.11 in women and 12.26 ± 6.34 in men. There was no statistical difference between them (p = 0.144; p = 0.631; p = 0.099).
Scale scores by HPV vaccination status
In Table 3 when the mean scale scores of men and women who had HPV vaccination were compared, no statistically significant difference was observed between them (p > 0.05). The mean total score was 19.00 ± 11.31 for women and 12.66 ± 2.30 for men (p = 0.554).
Vaccination status and HPV ınformation
To evaluate the relationship between HPV knowledge and vaccination status, a chi-square test of independence was performed at the p ≤ 0.05 significance level. The analysis revealed a statistically significant difference between knowledge scores between those who had received the vaccine and those who had not and HPV awareness (χ 2 = 17.106, p = 0.000) (Table 4).
Gender and HPV knowledge and vaccination status
It revealed a statistically significant difference between HPV vaccine awareness and gender among study participants (χ 2 = 10.206, p = 0.006) (Table 5). It revealed a statistically significant difference between HPV vaccination and gender among study participants (χ 2 = 5.332, p = 0.021) (Table 6).
Discussion
This study aimed to evaluate the knowledge levels of sexually active individuals about HPV, HPV screening test, and HPV vaccine and raise awareness. The results showed that having their first sexual experience at an early age and having a higher level of education made them more sensitive to the HPV vaccine. In the study, the age of the first sexual intercourse experience was found to be lower in men than in women. The low age of first sexual intercourse of men in developed countries is similar to the results of our study (Baiden et al. 2021; Flood et al. 2020). Although there was no statistically significant difference between the women and men included in the study in terms of using a barrier method in sexual intercourse, more than half of the participants expressed that they were protected by a barrier method. In the barrier method, the condom does not cover the entire region. Therefore, it does not provide full protection against HPV (Centers for Disease Control and Prevention (CDC) (CDC 2022). In this respect, it is important to mention the importance of vaccination to individuals and support them.
The fact that men’s first sexual experiences take place at an early age can be explained within the framework of hegemonic masculinity in the study (Ozansoy 2022). The high level of education and public employment of men have made men more sensitive to HPV vaccination. In their study, Tao et al. stated that 80% of men were willing to be vaccinated (Tao et al. 2022). A systematic review including twenty-nine studies showed that men’s active sex life and the HPV knowledge of their sexual partners were effective in their acceptance of the HPV vaccine (Newman et al. 2013). In their study, Gürsoy and Sagtas (2022) reported that single men had HPV vaccination more often than married men (Gürsoy and Sağtaş 2022). Agadayi et al. stated the HPV vaccination rate of women as 3.6% in their study, and the result is similar to this study (Agadayi et al. 2022). A study conducted on men in the United Arab Emirates reported that men had inadequate knowledge about HPV and vaccination (Al Shdefat et al. 2022). Upon reviewing the literature, it was found that the level of HPV knowledge was significantly lower in individuals who did not receive education in the field of health (Lee et al. 2022; Keten et al. 2021). In this sense, the study is in parallel with the literature, and it can be said that the HPV knowledge of individuals who do not have the opportunity to study or work in the field of health is adversely affected. In Turkey, HPV vaccines are not included in the national vaccination calendar and are left to the initiative of individuals. Currently, a single dose of HPV vaccine costs 2325 TL ($75) (Medication Guide 2024). Considering that the minimum wage is 17,022 TL, individuals’ access to the vaccine is restricted (Republic of Türkiye Ministry of Labour and Social Security 2024). In order to increase the HPV vaccination rate, in addition to providing information about HPV vaccination, the implementation of state-funded vaccination programs, community health centers, and school-based programs are more successful (Erol 2020).
In the study, women were found to have more knowledge about the HPV test according to the sex factor. Women are both more sensitive and knowledgeable about HPV. When the literature is reviewed, women are also seen to have knowledge about screening tests (Al Ghamdi 2022; Güllü 2023). In their study, Garg et al. reported that 62.4% of women were aware of HPV testing (Garg et al. 2022). Our study data are similar to the literature. In Turkey, cervical cancer screening tests are performed every 5 years, including women between the ages of 30–65, within the framework of the National Cancer Screening Standards (Republic of Türkiye Ministry of Health General Directorate of Public Health 2023). Physician appointments of sexually active women should be created by the Ministry of Health in order for the screening program to reach 70% (WHO 2021). Moreover, the fact that working women are considered on leave on the date of appointment will increase participation in the screening program.
In a study from 2019, 8581 women and men between the ages of 16–25 were included. According to the study results, the rate of knowledge about HPV and HPV vaccine was found to be 51.8% in young age groups, whereas the level of knowledge was found to be higher in women than in men (Kops et al. 2019). Likewise, according to a study involving men and women between the ages of 27–45, the level of knowledge was revealed to be higher in women. Accordingly, women have knowledge about HPV at a rate of 82.4% and about the HPV vaccine at a rate of 80%. The knowledge levels of men were determined to be 63.3% about HPV and 54% about the HPV vaccine (Thompson et al. 2020).
According to another study involving 6862 women and men, the rate of hearing about HPV was 74.5%, the rate of hearing about the HPV vaccine was 76.4%, and the HPV knowledge levels were found to be higher in women compared to men (Adjei Boakye et al. 2017).
According to a systematic review of 40 studies from 16 countries conducted in 2020, the rate of knowledge about HPV varies between 5.2–94.0% in European countries (López et al. 2020). In this context, according to another systematic review including 23 studies conducted in Turkey, the rate of hearing about HPV is in the range of 3.8–57.0%, and the rate of hearing about the HPV vaccine is in the range of 2.2–74.7% in Turkey. In the study by Ozdemir et al., women with high levels of education were found to have high levels of knowledge about HPV (Ozdemir et al. 2020). In conclusion, according to the literature, the level of knowledge about HPV and the HPV vaccine is higher in women than in men. In this respect, our findings are consistent with the literature.
The findings of this study demonstrated a significant association between HPV knowledge levels of people in Turkiye and vaccination rates and are consistent with previous studies (Lee et al. 2022; Keten et al. 2021; Tao et al. 2022; Al Shdefat et al. 2022). However, these findings should be interpreted cautiously as knowledge is only one of several factors that can affect vaccine uptake. One of the many priorities of Healthy People 2020 is to increase HPV vaccination. Due to the positive association between HPV knowledge and HPV vaccination, increasing HPV knowledge in this group of potential vaccine recipients is paramount to improving vaccination rates.
In addition, although women have higher levels of knowledge about HPV and vaccination compared to men, vaccination rates are low. According to 2018 Turkey Demographic and Health Survey (TDHS) data, the polygamy rate among men is 2%, while polygamy is not observed among women in Turkey (TDHS 2018). This suggests that men are more interested in vaccination. More studies are needed. The fact that men had a higher vaccination rate than women in the study can be explained by the fact that 20% of the female participants were housewives and did not have an income. To add again, HPV vaccines are not included in the national vaccination calendar in Turkey and are left to the initiative of individuals. Currently, the cost of a single dose of HPV vaccine is 2325 TL ($75). Considering that the minimum wage is 17,022 TL, it restricts the access of individuals, especially those without income, to the vaccine.
Limitations
Similar to most studies, this study has a few limitations. The study was a cross-sectional survey where participants self-selected to participate. Therefore, it is likely that participants interested in the topic of HPV opted to participate and may have skewed the findings of the study. Study results cannot be generalized to the whole population. In addition, the data analysis relied on self-reported data which may be subject to self-reported bias. The study was also conducted on people who were not healthcare professionals.
Conclusion
The present study elucidated that sexually active individuals had low levels of knowledge about HPV and very low HPV vaccination rates. According to the study results, sex was found to be an effective factor in the level of knowledge about HPV. The association between HPV knowledge and awareness and vaccination status was a significant finding. It provides support for public health professionals to continue their effort to promote and increase awareness, knowledge, and understanding of HPV.
Data Availability
The data generated and analysed during the current study are not publicly available but are available from the corresponding author on reasonable request.
References
Adjei Boakye E, Tobo BB, Rojek RP, Mohammed KA, Geneus CJ, Osazuwa-Peters N (2017) Approaching a decade since HPV vaccine licensure: racial and gender disparities in knowledge and awareness of HPV and HPV vaccine. Hum Vaccin Immunother 13(11):2713–2722. https://doi.org/10.1080/21645515.2017.1363133
Agadayi E, Karademir D, Karahan S (2022) Knowledge, attitudes and behaviors of women who have or have not had human papillomavirus vaccine in Turkey about the virus and the vaccine. J Community Health 47(4):650–657. https://doi.org/10.1007/s10900-022-01089-1
Akalın A (2022) Human Papillomavirus (HPV) infection and current approaches to HPV vaccine. Androl Bul 24(2):133–139. https://doi.org/10.24898/tandro.2022.25993
Al Ghamdi NH (2022) Knowledge of human papilloma virus (HPV), HPV-vaccine and pap smear among adult Saudi women. J Family Med Prim Care 11(6):2989–2999. https://doi.org/10.4103/jfmpc.jfmpc_2094_21
Al Shdefat S, Al Awar S, Osman N, Khair H, Sallam G, Maki S (2022) Identification level of awareness and knowledge of Emirati men about HPV. J Healthc Eng 21(2022):5340064. https://doi.org/10.1155/2022/5340064
Andiwijaya FR, Davey C, Bessame K, Ndong A, Kuper H (2022) Disability and participation in breast and cervical cancer screening: a systematic review and meta-analysis. Int J Environ Res Public Health 2;19(15):9465. https://doi.org/10.3390/ijerph19159465
Baiden P, Panisch LS, Kim YJ, LaBrenz CA, Kim Y, Onyeaka HK (2021) Association between first sexual ıntercourse and sexual violence victimization, symptoms of depression, and suicidal behaviors among adolescents in the United States: findings from 2017 and 2019 national youth risk behavior survey. Int J Environ Res Public Health 27;18(15):7922. https://doi.org/10.3390/ijerph18157922
Centers for Disease Control and Prevention (2022) Genital HPV infection – basic fact sheet ınternet adress: https://www.cdc.gov/std/hpv/stdfact-hpv.htm Access Date: 26.10.2022
Çevik E, Coşkun A (2021) Current approach to HPV infection and the role of the midwife. JOWHEN J Women’s Health Nurs 7(3):215–229
Della Fera AN, Warburton A, Coursey TL, Khurana S, McBride AA (2021) Persistent human papillomavirus ınfection. Viruses 20;13(2):321. https://doi.org/10.3390/v13020321
Demir F (2019) Validity and reliability of the Turkish version of Human Papilloma Virus knowledge scale. University of Health Sciences Gülhane Institute of Health Sciences Public Health Nursing Master Thesis Ankara
Erol Ö (2020) Preventing cancer development. Oncology nursing expanded and updated 2nd Edition (in), Can G (Editor), nobel medical ınscriptions, Istanbul, p: 31–39. (ISBN:978–605–335–505–2)
Flood T, Wilson IM, Prue G, McLaughlin M, Hughes CM (2020) Impact of school-based educational interventions in middle adolescent populations (15–17yrs) on human papillomavirus (HPV) vaccination uptake and perceptions/knowledge of HPV and its associated cancers: a systematic review. Prev Med 139:106168. https://doi.org/10.1016/j.ypmed.2020.106168
Food and Drug Administration (2015) Prescribing information [package insert]. Gardasil (human papillomavirus quadrivalent [types 6, 11, 16, and 18] vaccine, recombinant). Silver Spring, MD: US Department of Health and Human Services, Food and Drug Administration; 2015. Internet adress: https://www.fda.gov/media/74350 download Access Date: 08.11. 2022
Food and Drug Administration (2016) Prescribing information [package insert]. Cervarix (human papillomavirus bivalent [types 16 and 18] vaccine, recombinant). Silver Spring, MD: US Department of Health and Human Services, Food and Drug Administration; 2016. Internet adress: https://www.fda.gov/media/78013/download Access Date: 08.11.2022
Food and Drug Administration (2018) Prescribing information [package insert]. Gardasil 9 (human papillomavirus 9-valent vaccine, recombinant). Silver Spring, MD: US Department of Health and Human Services, Food and Drug Administration; 2018. Internet adress: https://www.fda.gov/media/90064/download Access Date: 08.11.2022
Garg A, Galvin AM, Matthes S, Maness SB, Thompson EL (2022) The connection between social determinants of health and Human Papillomavirus testing knowledge among women in the USA. J Cancer Educ 37(1):148–154. https://doi.org/10.1007/s13187-020-01798-y
Güllü A (2023) Examining HPV knowledge levels of midwifery and nursing undergraduate students: a cross-sectional study in Turkey. African J Reprod Health 27(6):101–109. https://doi.org/10.29063/ajrh2023/v27i6.11
Gürsoy MY, Sağtaş F (2022) Human Papillomavirus vaccination in male university students in Turkey: Coverage rate, barriers, and associated factors. J Prev 28:1–11. https://doi.org/10.1007/s10935-022-00711-1
Keten HS, Ucer H, Dalgaci AF, Isik O, Ercan Ö, Guvenc N (2021) Knowledge, attitude, and behavior of teachers regarding HPV (Human Papillomavirus) and vaccination. J Cancer Educ 36(3):584–590. https://doi.org/10.1007/s13187-019-01668-2
Kops NL, Hohenberger GF, Bessel M, Correia Horvath JD, Domingues C, Kalume Maranhã AG, Albus de Souza FM, Benzaken A, Pereira GF, Wendland EM (2019) Knowledge about HPV and vaccination among young adult men and women: Results of a national survey. Papillomavirus Res (amsterdam, Netherlands) 7:123–128. https://doi.org/10.1016/j.pvr.2019.03.003
Lee HY, Luo Y, Daniel C, Wang K, Ikenberg C (2022) Is HPV vaccine awareness associated with HPV knowledge level? findings from HINTS data across racial/ethnic groups in the US. Ethn Health 27(5):1166–1177. https://doi.org/10.1080/13557858.2020.1850648
López N, Garcés-Sánchez M, Panizo MB, de la Cueva IS, Artés MT, Ramos B, Cotarelo M (2020) HPV knowledge and vaccine acceptance among European adolescents and their parents: a systematic literature review. Public Health Rev 41:10. https://doi.org/10.1186/s40985-020-00126-5
Medication Guide (2024) Gardasil Kuadivalan Human Papillomavirüs (Type 6. 11. 16. 18) Recombinant vaccine 2024 prices. Internet Adress: https://www.ilacrehberi.com/ilac-fiyatlari/8699636950104/?y=2024. Accessed 04.18.2024
Meites E, Gee J, Unger E, Markowitz L (2021) Epidemiology and prevention of vaccine-preventable diseases. Centers for disease control and prevention. Human Popillomavirus. 14th ed. Washington DC: Public Health Foundation p.165–178. Internet Adress:https://www.cdc.gov/vaccines/pubs/pinkbook/downloads/hpv.pdf Access Date:13.08.2022
Newman PA, Logie CH, Doukas N, Asakura K (2013) HPV vaccine acceptability among men: a systematic review and meta-analysis. Sex Transm Infect 89(7):568–574. https://doi.org/10.1136/sextrans-2012-050980
Ozansoy N (2022) Men’s thoughts and attıtudes about sexualıty and vırgınıty in the context of hegemonıc masculınıty. Imgelem 2022;6(10): 307–330. https://doi.org/10.53791/imgelem.1069942
Ozdemir S, Akkaya R, Karaşahin KE (2020) Analysis of community-based studies related with knowledge, awareness, attitude, and behaviors towards HPV and HPV vaccine published in Turkey: a systematic review. J Turkish German Gynecol Assoc 21(2):111–123. https://doi.org/10.4274/jtgga.galenos.2019.2019.0071
Republic of Türkiye Ministry of Health General Directorate of Public Health (2023) 1-31 January cervical cancer awareness month. Internet Adress https://hsgm.saglik.gov.tr/tr/haberler-kanser/1-31-ocak-serviks-kanserifarkindalik-ayi.html. Accessed 12 Apr 2024
Republic of Türkiye Ministry of Labour and Social Security (2024) New minimum wage determined as 17 thousand 022 TL for 2024. Internet adress: https://www.csgb.gov.tr/asgari-ucret/. Accessed 20 Mar 2024
Tao Y, Shao H, Zhang T, Pu J, Tang C (2022) Factors influencing men’s attitudes toward HPV vaccination in males ıncluded in the Chinese National immunization program. Vaccines (Basel) 10(7):1054. https://doi.org/10.3390/vaccines10071054
Thompson EL, Wheldon CW, Rosen BL, Maness SB, Kasting ML, Massey PM (2020) Awareness and knowledge of HPV and HPV vaccination among adults ages 27–45 years. Vaccine 38(15):3143–3148. https://doi.org/10.1016/j.vaccine.2020.01.053
Turkey Demographic and Health Survey (2018) Internet adress: https://hips.hacettepe.edu.tr/tr/2018_tnsa_analiz_ve_rapor-56 Access Date:03.12.2024
Waller J, Ostini R, Marlow LA, McCaffery K, Zimet G (2013) Validation of a measure of knowledge about human papillomavirus (HPV) using item response theory and classical test theory. Prev Med 56(1):35–40. https://doi.org/10.1016/j.ypmed.2012.10.028
World Health Organization (2021) WHO guideline for screening and treatment of cervical pre-cancer lesions for cervical cancer prevention. 2021. Internet Adress: https://www.who.int/publications/i/item/9789240030824 Access Date: 12.29.2022
Acknowledgements
The authors would like to thank all of the participants who agreed to participate in the study.
Funding
Open access funding provided by the Scientific and Technological Research Council of Türkiye (TÜBİTAK). The authors received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
NG: Conceptualization, Methodology, Software, Supervision, Writing—review & editing.
BU: Conceptualization, Methodology, Software, Formal analysis, Writing—review & editing.
AYK: Methodology, Formal analysis, Writing—review & editing.
Corresponding author
Ethics declarations
Ethical approval
For the research, permission was first obtained from Istanbul University-Cerrahpaşa Social Sciences and Humanities Ethics Committee (Ethics Committee Date-No: 2022/249). Written permission was received from the author who performed the Turkish validity and reliability study of the HPV Knowledge Scale. The participants were first presented with an “Informed Consent Form” at the beginning of the Google survey and were requested to tick “I agree to participate in the study” if they voluntarily wanted to participate in the research. Those who did not give consent or discontinued the survey were not included in the study. All stages of the study were conducted in accordance with the Declaration of Helsinki.
Conflict of interest
The authors have no conflicts of interest to declare that are related to the content of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gencturk, N., Uncu, B. & Karaahmet, A.Y. Evaluation of the relationship between Human Papilloma Virus knowledge level and vaccination in adult individuals: a cross-sectional study. J Public Health (Berl.) (2024). https://doi.org/10.1007/s10389-024-02252-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10389-024-02252-9