
Abstract
Aim
This study investigates the impact of gender inequality on cancer mortality among European women across 27 countries from 2013 to 2020.
Subject and methods
The study explores the link between gender inequality and cancer mortality, employing pooled ordinary least squares regression. It evaluates socioeconomic gaps, healthcare access disparities, risky behaviours, and elements like screening, education, and life expectancy. The study also investigates how healthcare spending, employment, self-perceived health, and leisure activities influence mortality.
Results
The study shows that breast and cervical cancer screenings (BCS) significantly reduce cancer-related deaths among European women (CDW), with a negative impact of −0.0875. Similarly, tertiary education and participation in education and training (WEP) show a negative impact of −0.0021. Absolute life expectancy for women at birth (LEW) demonstrates a negative impact of −5.2603, all contributing to decreased cancer-related deaths.
Conversely, certain variables have a contradictory positive impact on CDW. Total healthcare expenditure (HCE) has a positive impact of +0.0311, and full-time equivalent employment (FER) of +0.3212. Women engaging in activities (WLW) has a positive impact of +0.6572. Self-perception of good health (WHG), refraining from smoking or harmful drinking (NSN) (+0.2649), and an active lifestyle with consumption of fruits and vegetables (PAF) (+0.2649) also impact positively, collectively contributing to increased cancer mortality among women.
Conclusion
The study highlights the importance of combating gender inequality to decrease cancer deaths in European women. Strategies include closing healthcare gaps and enhancing health education. Complex links between smoking, alcohol, and cancer mortality require further research. Interventions targeting disparities, healthcare access, and risky behaviours can notably lower cancer mortality.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gender inequality refers to the imbalance in treatment and opportunities individuals experience based on gender, resulting in disparities across various facets of life (EIGE 2023a). Women in low, middle-, and high-income countries are disproportionately affected by cancer due to vulnerabilities related to gender inequality, poverty, and environmental factors (Cesario 2012). Based on the research by Donington and Colson (2011), it becomes evident that gender inequality has played a pivotal role in contributing to a substantial rise in cancer cases among women. This distressing trend has propelled cancer to the forefront as the primary cause of mortality among women in the United States.
The extent of this disparity transcends social realms and permeates into health outcomes, casting a prominent shadow over women's cancer fatality rates, as highlighted in the research by Vaccarella et al. (2023) and the Organisation for Economic Co-operation and Development (OECD 2015). The intricate tapestry of gender inequality intertwines with myriad facets, giving rise to discrepancies in cancer-related consequences. Elements including socioeconomic conditions, educational disparities, healthcare accessibility, and societal norms synergistically contribute to the vulnerability of women to cancer, dictating the trajectory of diagnosis, therapeutic interventions, and ultimate survival rates (WHO 2021; Allen and Sesti 2018; Mobaraki and Soderfeldt 2010).
This concept is further reinforced by the work of Donington and Colson (2011), who emphasize the multifaceted role of gender inequality in the aetiology, prevention, and management of cancer. Their research underscores the complexity of this issue, which is intricately woven with physiological variations, behavioural influences, lifestyle factors, and equitable access to medical care. As evidenced by the findings of Jolidon (2022) and Willems et al. (2020), the presence of macro-level gender inequality has a detrimental impact on women's engagement in cancer screening initiatives. This lamentable circumstance has subsequently contributed to an alarming surge in cancer mortality rates. Indeed, Wellems et al. (2020) employed Bird and Rieker's (2008) theory of constrained choices, which explains how policy, community, work, and family contexts shape gender-related health differences and individuals' health decisions. This approach highlighted that women's health benefits from policies promoting political participation, autonomy, family roles, and increased macro-level empowerment.
Moreover, increased autonomy and decision-making authority boost women's use of healthcare services (Osamor and Grady 2016). Conversely, unfavourable social contexts and policies can limit women's ability to prioritize health, constraining their control over health choices and presenting conflicts between health and family responsibilities (Bird and Rieker 2008). Similarly, gender inequalities perpetuated through reproductive health, family, employment, and political policies can worsen women's health via stress, discrimination, financial strain, violence, and the double burden of work (Borrell et al. 2014).
Across European nations, a spectrum of variations in gender inequality comes into view, indicating that certain countries contend with more pronounced disparities than others. For instance, in 2013, Latvia (0.231), Hungary (0.251), Romania (0.315), and Bulgaria (0.214) experienced notable gender inequality, evident through values surpassing the threshold of 0.2. Conversely, Sweden (0.048), Denmark (0.039), the Netherlands (0.042), Finland (0.062), Germany (0.079), Slovenia (0.070), Luxembourg (0.071), Belgium (0.074), Austria (0.085), Italy (0.087), Spain (0.084), and Portugal (0.098) demonstrated lower levels of gender inequality, each registering values under 0.1. Despite concerted efforts aimed at addressing gender inequality, Hungary (0.222), Romania (0.283), and Bulgaria (0.211) have consistently maintained high levels of inequity even as of 2021 (see Fig. 1A, B). These nations offer insights into the unique attributes of gender inequality within the European context, encompassing dimensions such as gender pay disparity, occupational segregation, inadequate representation in leadership positions, and the intricate dynamics surrounding work/life balance.

Illustrates the assessment of the gender inequality index across European countries from 2013 to 2021 (A, B). This index represents the extent of gender inequality within the 27 European countries during the specified years. Furthermore, an examination of the gender inequality index within the European countries was conducted from 2013 to 2021 (C). The map graph, a critical visualization in this study, was meticulously crafted by the authors utilizing data from the United Nations Development Programme (UNDP 2022)
Undoubtedly, gender inequality persists as a prevalent concern within European countries, encompassing disparities across domains such as education, employment, decision-making, healthcare, and societal interactions. Women's educational opportunities often remain constrained, limiting their entrance into traditionally male-dominated professions. The labour market reflects this inequality through employment gaps, occupational segregation, and a persistent gender pay disparity. Despite strides in various sectors, women's representation in political and economic decision-making positions continues to lag behind. Within healthcare, discernible gaps in service access and reproductive health persist. The broader issues of gender-based violence and discrimination further compound these challenges. Pursuing equitable solutions necessitates unwavering commitment, as ongoing policy initiatives and advocacy endeavours seek to shape a society that is inclusive and fair to all (European Institute for Gender Equality 2023a; European Commission 2020).
Through legislative measures, policy frameworks, and awareness campaigns, European countries have embarked on a journey to cultivate gender equality and empower women. These collective efforts have resulted in a reduction in gender inequality, from a value of 0.126 in 2013 to 0.100 in 2021—an encouraging 2.6% decline (refer to Fig. 1C). This approach signifies a step forward in the quest for parity and serves as a testament to the potential impact of dedicated initiatives on reshaping the gender landscape.
This intersection of varying gender inequality levels with a pressing concern within European countries, namely cancer mortality, is a significant aspect to consider. In European countries, cancer-related deaths carry considerable weight with regard to public health. In 2013, several European countries registered elevated cancer mortality rates among women. Notably, Hungary (268.6), Denmark (258.4), Slovakia (234.4), the Netherlands (233.1), Slovenia (234.7), Ireland (244.0), Croatia (242.5), Czechia (223.5), Poland (219.8), Latvia (215.5), Sweden (207.8), Estonia (207.3), Germany (205.4), and Belgium (200.5) faced relatively higher rates. On the contrary, Greece (175.9), Bulgaria (175.2), Cyprus (151.0), Portugal (167.4), and Spain (160.4) displayed comparably lower rates of cancer mortality among women. The year 2020 marked a reduction in cancer mortality rates among women in several European countries, including France, Germany, Belgium, Sweden, Estonia, Luxembourg, and Austria. These countries have demonstrated progress in addressing the issue of cancer-related deaths among women. Nonetheless, Slovakia, Hungary, Poland, Latvia, Ireland, Denmark, Czechia, and Croatia still grapple with persistently high cancer mortality rates among women (refer to Fig. 2A, B). Remarkably, European countries have witnessed a notable decline in the cancer mortality rate among women over time. Concerted efforts and initiatives led to a reduction from 262 in 2013 to 241 by the year 2020 (see Fig. 2C).

Illustrates the landscape of cancer-related mortality among women in European countries, delineating crucial aspects across distinct time frames and geographical extents: (A, B) Cancer-related mortality in women across various European countries for the years 2013 and 2020, offering a comparative view of how this vital metric has evolved. (C) Overall cancer-related mortality among women encompassing all European countries from 2013 to 2020, enabling a comprehensive understanding of the cumulative trends over this period. The authors have meticulously crafted the visual representation presented in this map graph. It draws upon data sourced from Eurostat (2023a)
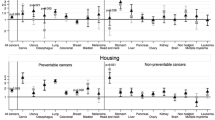
Moreover, breast cancer emerges as the predominant contributor to cancer-related deaths among women in European countries, representing 28.75% of cases in 2020. Lung cancer follows closely at 27.18%, colorectal cancer at 21.60%, pancreatic cancer at 13.94%, and ovarian cancer at 8.54% (refer to Fig. 3A). This distribution underscores the significant impact of these specific cancer types on women's health in European countries.

Cancer-related mortality patterns among women in the European countries, 2020: (A) Distribution of cancer-related deaths by the most common causes—percentage distribution (%) across the European countries in 2020. (B) Estimated cancer mortality by age group—percentage distribution (%) among women across the European countries in 2020. (C) Distribution of cancer mortality by cancer type—percentage distribution (%) among women across the European countries in 2020. (D) Age-standardized cancer mortality rates among women across the European countries in 2020. The authors crafted this graphical representation, using data from the European Cancer Information System (ECIS 2023)
Within the European countries, the distribution of cancer-related deaths among women in 2020 reveals distinct variations across diverse age groups: Among women aged 0–44 years, breast cancer is the principal cause of cancer-related deaths, contributing to 31% of cases. Cervical/uterine cancer follows at 11%, accompanied by brain central nervous system (CNS) cancer at 10%, lung cancer at 6%, and other cancer sites at 42% (refer to Fig. 3B). In the age group of 45–64 years, lung cancer is the primary cause of cancer-related deaths among women, accounting for 24% of cases. Breast cancer closely follows at 20%, while colorectal cancer constitutes 9%, pancreatic cancer is 7%, and other cancer sites 40% (refer to Fig. 3B).
For women aged 65 years and above, breast cancer remains a notable cause of cancer deaths, contributing to 16% of cases. Lung cancer ranks second at 15%, colorectal cancer at 14%, pancreatic cancer at 9%, and other cancer sites account for 46% of the distribution (refer to Fig. 3B).
The percentage distribution of cancer mortality among women in the European countries for 2020 reveals noteworthy patterns. Breast cancer accounts for 16.53% of cancer-related deaths, making it a substantial contributor. Lung cancer follows closely behind at 15.61%, with colorectal cancer representing 12.4% of mortality cases. Pancreatic cancer contributes to 8.01% of cancer deaths among women. Remarkably, other cancer sites encompass 26.58% of the overall mortality distribution (Fig. 3C).
Regarding mortality among women in European countries, the age-standardized mortality rate attributed to breast cancer stands at 34.1 per 100,000, while lung cancer registers at 33.2 per 100,000. Colorectal cancer is characterized by an age-standardized rate of 24.5 per 100,000, while pancreatic cancer is recorded at 16.2 per 100,000 population. Meanwhile, ovarian cancer demonstrates an age-standardized rate of 10.2 per 100,000 population (Fig. 3D). This comprehensive overview of cancer mortality statistics among women underscores the critical health implications and provides a basis for further exploration and analysis.
The above statistics unequivocally underscore the imperative nature of delving into the factors contributing to women's susceptibility to cancer-related mortality within European countries. Extensive research consistently reveals that gender-based discrepancies in cancer mortality emanate from intricate interplays among biological, behavioural, societal, and systemic elements. A notable instance is the potential hindrance women encounter in obtaining timely cancer diagnoses, often due to lower levels of health literacy or constrained access to healthcare services. Furthermore, prevailing societal norms and gender-specific expectations can dissuade women from seeking swift medical attention or participating in vital cancer screening initiatives, as Jolidon (2022) and Willems et al. (2020) mentioned.
Ameliorating gender inequality in cancer mortality necessitates a multifaceted and comprehensive strategy. Gaining a profound understanding of the precise mechanisms by which gender-based disparities impact cancer outcomes empowers healthcare systems and policymakers to enact targeted measures and policies to alleviate such inequalities. This proactive approach includes promoting gender-sensitive healthcare practices, enhancing accessibility to cancer screening and treatment, and addressing the underlying social determinants of health that disproportionately affect women. These interventions must acknowledge and cater to the distinct challenges encountered by diverse subsets of women, whether rooted in age, socioeconomic status, or geographical location. By embracing a holistic framework, this investigation can aspire to diminish gender-driven disparities in cancer mortality, thus enhancing the overall well-being and prospects of women across European countries.
Exploring the link between gender inequality and cancer mortality is a topic addressed by a limited number of researchers in the existing literature. A few authors have explored this topic (e.g., Vaccarella et al. 2023; Jolidon 2022; Chan et al. 2022; Gedefaw et al. 2020; Raghupathi and Raghupathi 2020; Bosetti et al. 2013; World Cancer Research Fund/American Institute for Cancer Research 2018; Lugo et al. 2017; Donington and Colso 2011). As an illustration, Bosetti et al. (2013) delved into European cancer mortality data from 1980 to 2009. Their findings highlighted persistent gender disparities, with men exhibiting higher mortality rates across most cancer types. Breast and lung cancers emerged as the foremost causes of cancer-related deaths among women. This investigation emphasized the need to scrutinize the underlying factors contributing to the observed gender-based gaps in cancer mortality rates.
Socioeconomic factors are instrumental in shaping these disparities. For instance, Vaccarella et al. (2023) conducted an insightful study examining the correlation between socioeconomic status and cancer survival in Europe from 1990 to 2015. Their findings revealed that women from lower socioeconomic backgrounds faced higher mortality rates. Socioeconomic disparities, encompassing education, income, and occupation, contribute significantly to the gender inequality manifested in cancer-related fatalities.
Additionally, risk behaviours, such as alcohol and tobacco consumption, further contribute to the variance in cancer mortality rates between genders. Lugo et al. (2017) explored smoking prevalence in Italy, offering insights that resonate with the broader European context. While the study focused on Italy, its implications extend to the general trend within the European Union (EU). The research revealed that, although smoking rates were generally higher among men, the gender disparity was diminishing in numerous countries. This shift suggests that women are becoming increasingly susceptible to the detrimental health effects of smoking, including lung cancer, thus exacerbating the gender discrepancy in cancer-related deaths.
Moreover, dietary habits and physical activity influence cancer mortality rates among women. A balanced intake of fruits and vegetables, coupled with regular exercise, is recognized for contributing to overall well-being and reducing specific cancer risks (World Cancer Research Fund/American Institute for Cancer Research 2018; Chan et al. 2022).
Most investigations thus far have focused primarily on examining the influence of inequalities solely on cancer mortality. As a result, the potential correlation between gender inequality and cancer mortality among women has been largely overlooked. To put it differently, a significant gap within the current literature necessitates thorough exploration. Furthermore, it is noteworthy that the preceding studies mentioned have not incorporated gender inequality indicators into their investigative methodologies or econometric models. Hence, these existing gaps create an opportunity for this investigation into the intricate relationship between gender inequality and cancer mortality in women.
This investigation seeks to answer the following question to address this knowledge gap. To what extent does gender inequality among women in Europe impact cancer mortality? Two potential hypotheses are proposed to explore this inquiry:
-
H1: Gender inequality in European countries influences women's cancer mortality rates through educational disparities, socioeconomic status, healthcare access, and risk behaviours. Greater gender inequality may result in limited education and awareness, promoting unhealthy behaviours and impeding healthcare access. These combined factors could contribute to higher cancer mortality rates (e.g., Donington and Colson 2011; OECD 2015; Gavurova et al. 2020; Willems et al. 2020; Jolidon 2022; and Vaccarella et al. 2023).
-
H0: Gender inequality within European countries is not significantly associated with cancer mortality rates among women. This suggests that lower levels of gender inequality, characterized by reduced discrepancies in socioeconomic status, healthcare access, and risk behaviours, do not correlate with increased mortality rates among women with cancer in European nations.
This study will examine the impact of gender inequality indicators on cancer mortality rates among women in European countries from 2013 to 2020 to validate these hypotheses and address the research gap. This impact will be achieved by applying econometric methods, such as pooled ordinary least squares (OLS) regression. The study aims to offer insights into gender disparities in cancer mortality and to identify the contributing factors. While the chosen methodology enables quantitative analysis and the examination of large-scale trends, it is essential to acknowledge its limitations, including aggregated data that may conceal individual-level variations, reliance on existing data sources with potential accuracy and completeness issues, and the study's observational nature.
This research aims to fill a significant gap in the existing literature by exploring the intricate relationship between gender inequality and cancer mortality, specifically focusing on women within the European context. While previous studies have examined gender disparities in cancer outcomes and the factors influencing them, few have undertaken a holistic approach that delves into the multifaceted dimensions of gender inequality and its intersection with cancer-related mortality rates.
The motivation behind this research stems from recognizing that gender inequality is a persistent issue that permeates various aspects of individuals' lives, including health outcomes. The observed disparities in cancer mortality rates between genders highlight the need for a comprehensive investigation into the underlying factors contributing to these differences. By unravelling the complexities of this relationship, this investigation can reveal the mechanisms through which gender inequality influences cancer outcomes, thereby informing targeted interventions and policies that aim to reduce these disparities.
The relevance and significance of this research lie in its potential to drive evidence-based interventions and strategies aimed at mitigating gender-driven disparities in cancer-related mortality. As cancer continues to be a significant public health concern within European countries, understanding the role of gender inequality in exacerbating these disparities is pivotal. This study's findings can potentially inform healthcare systems, policymakers, and advocacy efforts in devising interventions that foster equitable access to healthcare services, promote gender-sensitive healthcare practices, and address systemic gender inequalities that impact women's health outcomes.
This research introduces novel contributions to the existing body of work by adopting a comprehensive approach that considers the multifaceted dimensions of gender inequality and their interplay with cancer mortality outcomes. By employing pooled OLS regression, this investigation seeks to provide quantitative insights into the specific socioeconomic, healthcare, and behavioural factors that contribute to gender-based disparities in cancer mortality rates. Integrating economic and health-related methodologies adds depth and rigour to the analysis, offering a nuanced understanding of the complex interactions at play.
In contrast to existing studies that often focus on specific aspects of cancer disparities or gender inequality, this investigation's unique contribution lies in its holistic approach that considers the comprehensive spectrum of factors contributing to gender-driven disparities in cancer-related deaths. By considering a wide range of variables, including socioeconomic status, healthcare access, risk behaviours, and societal norms, this study aims to provide a comprehensive view of the multifaceted landscape of the impact of gender inequality on cancer outcomes. As such, this research promises to advance our understanding of the gender-related dynamics within cancer mortality and to inform evidence-based strategies to effectively address these disparities.
This study, striving for a thorough and all-encompassing inquiry, will rigorously follow a structured sequence of theoretical research procedures. These deliberately chosen steps, artistically illustrated in Fig. 4, have been meticulously crafted to guarantee a coherent and robust exploration of the focal topic.

Scientific method steps. The authors created this figure
This paper introduces the related literature in the following section as a basis for the subsequent sections. Section 2 outlines the research methodology and data, while Section 3 presents the empirical results. The main findings are thoroughly discussed in Section 4, and Section 5 presents the conclusions.
Data and methods
In this section, this empirical investigation will detail the approach, methodologies, and considerations that guided the empirical investigation exploring the impact of gender inequality on cancer mortality among women in 27 diverse European countries.
Study design
This empirical investigation examined the association between gender inequality and cancer mortality in women across 27 European countries including Austria, Belgium, Bulgaria, Croatia, Cyprus, Czechia, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Spain, and Sweden.
The selection of 27 European countries for this investigation is justified as it provides a diverse representation of the region, capturing socioeconomic, cultural, and healthcare variations. By including multiple countries, we can explore the influence of regional factors on gender disparities in cancer mortality, enhance the statistical power of the analysis, and facilitate meaningful comparisons and benchmarking. This approach enables a comprehensive examination of the impact of gender inequality on cancer mortality in women across different contexts, contributing to a deeper understanding of the issue and informing effective strategies to reduce disparities.
The study utilized a time series from 2013 to 2020. The selection of a time series for the study's analysis of the impact of gender inequality on cancer mortality among women in 27 diverse European countries is grounded in the data availability and integrity principle. By focusing on this specific time frame, the study ensures the utilization of complete and reliable data, thereby ensuring the consistency and comparability of the analysis across different countries and years. This approach mitigates the potential issues associated with the use of more recent data, such as data collection methodologies and reporting accuracy, and allows for statistically significant findings while contextualizing the results within the historical and sociopolitical landscape of the period.
Data
Table 1 presents the variables selected for this empirical investigation. These variables will be used to analyse and assess the relationship between different factors and the research objective.
The selected variables were thoughtfully chosen to analyse the impact of gender inequality on cancer mortality in women. These independent variables are scientifically justified and relevant to women's health, as follows:
-
Healthcare_expenditure (HCE): Adequate healthcare services, including cancer screening and treatment, are vital for women's access to quality healthcare, impacting cancer outcomes (Starfield et al. 2005; Akinyemiju et al. 2015).
-
Bc_cc_screenings_women (BSC): Screening programs for breast and cervical cancer detection at an early stage can improve survival rates and reduce mortality among women (Yang et al. 2022).
-
Fte_employment_rate_women (FER): Women's employment rates reflect their socioeconomic status and access to healthcare resources, including cancer prevention and treatment (Vaccarella et al. 2023).
-
Women_edu_part (WEP): Women's higher education levels are associated with better health outcomes, including lower cancer mortality, through improved health literacy and healthcare-seeking behaviours (Gedefaw et al. 2020; Raghupathi and Raghupathi 2020; Vaccarella et al. 2023). Moreover, engagement in education and training programs promotes health knowledge, awareness, and behaviours related to cancer prevention, detection, and treatment adherence among women (Del Carmen et al. 2021; Poudel et al. 2021).
-
Women_leisure_workers (WLW): Regular physical activity and leisure engagement contribute to improved overall health, reduced cancer risk, and better cancer outcomes in women (Schnohr et al. 2005; Liu et al. 2016).
-
Women_health_good (WHG): Women who perceive their health as good or very good will likely experience better overall health and access adequate healthcare services. This positive self-perception may indicate a healthier lifestyle, including regular exercise, a balanced diet, and proactive healthcare-seeking behaviours. Moreover, women who perceive their health as good or very good may experience several benefits associated with lower cancer deaths (Korn et al. 2013).
-
Life_expectancy_women (LEW): Higher life expectancy reflects better overall health and access to healthcare, leading to lower cancer mortality rates among women (Ranabhat et al. 2018; Hao et al. 2020).
-
Non_smoke_nondrink_women (NSN): Lower prevalence of smoking and harmful drinking behaviours reduces the risk of various cancers and contributes to decreased cancer mortality rates among women (Anand et al. 2008; Lugo et al. 2017).
-
Phys_activity_fruit_veg_women (PAF): Regular physical activity and a healthy diet, including fruits and vegetables, protect against cancer and can lower cancer mortality rates among women (Donaldson 2004; Schnohr et al. 2005; Liu et al. 2016; Kerschbaum and Nüssler 2019; Chan et al. 2022).
-
Unmet_medical_needs_women (UMN): High rates of unmet need for medical examinations indicate barriers to accessing healthcare services, including cancer screening, potentially leading to delayed diagnosis and increased cancer mortality among women (Williams et al. 2013; Quintal et al. 2023).
The independent variables FER, WEP, WLW, WHG, LEW, NSN, PAF, and UMN are indicators in the Gender Equality Index developed by the European Institute for Gender Equality (EIGE) (2023b). Studying women in this investigation is justified due to the unique implications of gender inequality on their health outcomes, socioeconomic disadvantages, and risk behaviours. It provides valuable insights into the factors contributing to gender disparities in cancer mortality, helping develop targeted interventions to improve outcomes and address these disparities.
Method
This subsection delineates the pivotal stages of the methodology, beginning with preliminary tests and culminating in applying the pooled OLS regression. After outlining the theoretical framework guiding our investigation, the next phase reveals the meticulous empirical research steps that will be methodically undertaken. The sequential progression of empirical inquiry, depicted in Fig. 5, is primed to manifest the tangible application of the study's theoretical foundations. These steps have been meticulously structured to operationalize abstract concepts, allowing the study to gather tangible data and tangible observations from the real world.

Empirical investigation steps. The authors developed this figure
Figure 5 offers a visual representation of these empirical investigation stages, outlining the systematic methodology that the study will adopt. By adhering to this well-structured framework, the study endeavours to bridge the conceptual gap between theory and practical execution, thereby cultivating a comprehensive understanding of the subject matter. Each empirical step is executed precisely, interlocking seamlessly with its precursor to ensure a coherent and progressively unfolding investigative process.
This painstaking approach aims to extract practical insights and substantive conclusions that enrich academic scholarship and pragmatic comprehension. By meticulously adhering to the outlined empirical investigation steps, the study aspires to validate its theoretical hypotheses while illuminating the nuanced intricacies that surface in the real-world context. Such methodological transparency reinforces the study's integrity and empowers fellow researchers with a clear roadmap for replicating and extending this empirical investigation in the future.
Preliminary tests
Before initiating the pooled OLS estimator regression, it is essential to execute initial examinations to comprehend the nature of the variables within the economic model. As a result, the following preliminary assessments were undertaken to gauge the attributes of the variables featured in the model:
-
I.
Descriptive analysis: Descriptive statistics encompassing mean, standard deviation, minimum, maximum, and quartiles were computed for each variable. These statistics provided an overarching snapshot of the variable characteristics.
-
II.
Histogram visualization: Histograms were employed to visually depict the distribution of each variable. This visualization aided in detecting potential skewness, kurtosis, or outliers within the dataset.
-
III.
Pairwise correlation test (Jolliffe 2002): The calculation of pairwise correlations revealed the magnitude and direction of the linear relationships between variable pairs, offering insights into their interconnectedness.
-
IV.
Normality test via skewness and kurtosis (D'Agostino and Pearson 1973): A test was conducted to determine whether each variable adhered to a normal distribution. The null hypothesis assumed a normal distribution for the variable.
-
V.
Pesaran CD test (Pesaran 2004): This test assessed the presence of cross-sectional dependence within panel data. The null hypothesis posited the absence of cross-sectional dependence.
-
VI.
Fisher-type unit root test (Fisher 1925): This test examined the potential presence of a unit root in each variable. The null hypothesis suggested the existence of a unit root.
-
VII.
Variance inflation factor (VIF) test (Belsley et al. 1980): This test checked for multicollinearity between the variables.
-
VIII.
Autocorrelation test using the Wooldridge method (Wooldridge 2002): This test examined the potential presence of autocorrelation within the error term. The null hypothesis posited the absence of autocorrelation.
-
IX.
Heteroskedasticity test through the Breusch–Pagan/Cook–Weisberg approach (e.g., Breusch and Pagan 1979; Cook and Weisberg 1983): This test evaluated the existence of heteroskedasticity within the error term. The null hypothesis implied the absence of heteroskedasticity.
The insights garnered from these initial assessments were instrumental in understanding the attributes of the variables and flagging potential concerns, such as deviations from normality, autocorrelation, or heteroskedasticity. These issues could impact the subsequent pooled OLS regression analysis. Furthermore, these preliminary tests are widely employed across the econometric literature to ensure model robustness and validity (e.g., Baltagi 2013; Greene 2012; Wooldridge 2015).
Pooled OLS model
The pooled OLS model regression is a statistical method used to estimate the relationship between a dependent variable and one or more independent variables. The general equation for the pooled OLS model regression is:
where x1, ⋯, x12 are the independent variables, β1, ⋯, β12 are the regression coefficients representing the relationship between the independent variables and the dependent variable CDW, and εit is the error term, representing the unexplained variation in the dependent variable. Therefore, the pooled OLS regression estimates the values of the regression coefficients (β) that minimize the sum of squared residuals, providing insight into the relationship between the independent and dependent variables. The coefficients can be interpreted as the average change in the dependent variable associated with a one-unit change in the corresponding independent variable, holding other variables constant.
The utilization of pooled OLS regression in this study is underpinned by its suitability for panel data analysis involving multiple European countries over a period. This model efficiently capitalizes on the combined time series and cross-sectional variations inherent in the dataset, providing statistical power to uncover potential relationships between gender inequality and cancer mortality. Pooled OLS simplifies the investigation of a shared relationship by assuming homogeneity of regression coefficients across countries, allowing for a straightforward interpretation of findings. While acknowledging its limitations in capturing country-specific nuances, this approach presents a practical means to discern general trends and patterns across diverse countries, facilitating effective communication of research outcomes to various stakeholders.
Econometric software and Stata commands
Indeed, this empirical investigation utilized Stata 17.0 (License number 54389) as the chosen econometric software. The study employed various Stata commands to conduct the analysis, including but not limited to sum, histogram, pwcorr, sktest, xtcd, xtunitroot, vif, xtserial, hettest, reg, and reg robust. These commands were utilized for conducting preliminary tests and model estimations. The following section will provide an overview of the empirical results obtained in this research.
Empirical results
This section unveils the empirical findings of our study, preceded by a series of preliminary tests before the pooled OLS regression analysis. As a prelude, Table 2 expounds the summary statistics for the variables under scrutiny, delivering an overview of their distribution and essential attributes.
The results from Table 2 above show that the variable CDW has an average of approximately 5.29 with a standard deviation of 0.14, ranging from 4.94 to 5.59. For HCE, the mean is about 9.55, with a standard deviation of 1.56, spanning from 6.68 to 12.98. BCS has an average of 4.00, a standard deviation 0.30, and ranges between 3.30 and 4.43. Similarly, FER shows an average of 3.74, a standard deviation of 0.14, and data ranging from 3.37 to 4.08. The variable WEP exhibits an average of approximately 43.33, a standard deviation 14.40, and varies from 20 to 82. WLW has an average of 0.09, a standard deviation of 0.21, and ranges from −0.54 to 0.34. For WHG, the mean is approximately 4.13, the standard deviation is 0.18, and the data spans from 3.64 to 4.43. LEW shows an average of 4.41, with a slight standard deviation of 0.03, varying from 4.34 to 4.45. NSN has an average of 4.28, a standard deviation of 0.08, and ranges from 4.11 to 4.44. PAF averages around 3.46, with a higher standard deviation of 0.51, from 1.95 to 4.22. Lastly, UMN averages 1.56, a standard deviation of 0.81, and ranges from 0 to 3.09. These statistics provide valuable insights into the dataset's central tendencies, spread, and ranges, contributing to a comprehensive understanding of the variables' characteristics before further regression analysis.
Following the presentation of descriptive statistics for the variables, the next step involves the computation of histograms to visually represent the distribution of each variable. These histograms aid in identifying any potential skewness, kurtosis, or outliers within the dataset. Figure 6 shows the histogram of variables.

Histogram of variables. The Stata command histogram was used
The histograms provide valuable insights into the data distribution for each variable. The dependent variable CDW exhibits a relatively symmetrical distribution, indicating a reasonably even spread of observations across its value range. Similarly, the independent variable HCE displays a roughly symmetrical distribution, suggesting a balanced distribution of observations across its range. Conversely, the independent variable BCS demonstrates right-skewness, indicating a greater concentration of observations with smaller BCS values and fewer with larger values. FER, another independent variable, shows a relatively symmetrical distribution, mirroring the dispersion of observations.
On the other hand, WEP exhibits left-skewness, implying a higher number of observations with larger WEP values and fewer with smaller values. The independent variables WLW, WHG, and LEW exhibit right-skewed distributions, suggesting that more observations are concentrated in the lower value range, while the independent variables NSN, PAF, and UMN display roughly symmetrical distributions, reflecting an even distribution of observations across their respective value ranges.
After generating the histograms for the variables, a pairwise correlation test was conducted to examine the relationships between variables. The results of the pairwise correlation test are presented in Table 3.
The findings presented in Table 3 reveal a range of correlation levels among the variables, from weak to moderate. Noteworthy correlations include a positive association between CDW and FER, as well as CDW and WEP. Conversely, negative correlations are evident between CDW and WHG, LEW, NSN, and UMN. Furthermore, a positive correlation is observed between HE and WHG, along with LEW, while HCE exhibits a negative correlation with BCS. Other variables also exhibit diverse degrees of correlation.
After completing the pairwise correlation test, further analyses were conducted on the dataset. Specifically, the skewness/kurtosis tests for normality (D'Agostino and Pearson 1973) were carried out to assess the distribution of each variable in the econometric model. The outcomes of the skewness/kurtosis tests for normality are presented in Table 4.
The outcomes of the skewness/kurtosis tests suggest that the variables CDW, HCE, BCS, FER, WEP, WLW, WHG, LEW, and PAF deviate from a normal distribution. In contrast, NSN and UMN variables demonstrate a closer approximation to a normal distribution. After completing the skewness/kurtosis tests, the next step involves conducting the Pesaran CD test. The outcomes of the Pesaran CD test are presented in Table 5.
The findings in Table 5 demonstrate that cross-sectional dependence exists in the residuals of the panel data regression for certain variables (CDW, HCE, BCS, and FER). This finding suggests that the assumption of cross-sectional independence might not be valid for these variables. However, it is essential to note that the CD test results are not reported for the variables WEP, WLW, WHG, LEW, NSN, PAF, and UMN, indicating that the test could not be conducted due to missing observations for these particular variables. This limitation highlights the necessity of addressing missing data to ensure comprehensive and accurate statistical analyses.
When cross-sectional dependence is detected, assessing the presence of unit roots among the variables in the econometric model becomes imperative. The Fisher-type unit root test was employed to accomplish this. The outcomes of the Fisher-type unit root test are presented in Table 6, providing insight into the stationarity properties of the variables under investigation.
The insights from Table 6 shed light on the stationarity characteristics of the variables under scrutiny. Notably, it becomes evident that CDW and BCS variables exhibit behaviour between the I(0) and I(1). Conversely, the variable HCE demonstrates stationarity, indicating an absence of trend or unit root. However, it is worth noting that for variables FER, WEP, WLW, WHG, LEW, NSN, PAF, and UMN, the unit root tests could not be conducted due to data unavailability, resulting in missing observations for these specific variables. In simpler terms, the Fisher-type unit root test requires strongly balanced data for precise outcomes, a challenge shared by the Levin–Lin–Chiu unit root test and the Pesaran unit root test.
Following the completion of the unit root tests, multicollinearity among the dataset's variables was assessed through the computation of VIF values. The outcomes of the VIF test are presented in Table 7.
The VIF test results reveal that none exceeds the threshold of 10, indicating that the multicollinearity is not severe. With a mean VIF of 4.59, the overall model has a moderate level of multicollinearity. While it is crucial to consider multicollinearity when interpreting regression results, the findings suggest it is not a significant concern. Lastly, the Wooldridge and Breusch–Pagan/Cook–Weisberg and Breusch–Pagan/Cook–Weisberg tests were conducted. The results of these tests are presented in Table 8.
Table 8 indicates that the Wooldridge test for autocorrelation in panel data could not be executed due to unbalanced panel data. Conversely, the Breusch–Pagan/Cook–Weisberg test results for heteroskedasticity reveal a chi-square statistic of 1.61 (p = 0.2047). This outcome suggests a lack of substantial evidence to reject the null hypothesis of constant variance, indicating the absence of heteroskedasticity within the model. Consequently, the justification for employing pooled OLS regression remains strong, as it assumes constant variance and is corroborated by the absence of substantial contradictory evidence.
Following the preliminary tests, the pooled OLS regression can be performed. The decision to utilize pooled OLS regression in this study is supported by the comprehensive analysis of the dataset's characteristics and the findings of various diagnostic tests. First, the descriptive statistics presented in Table 2 offer an initial understanding of the variables' distributions, means, and ranges. While variations exist, no extreme outliers or highly skewed distributions are observed that would necessitate adopting alternative regression techniques. Furthermore, the pairwise correlation analysis results in Table 3 reveal moderate levels of correlation among the variables, indicating that multicollinearity is not severe. While some variables show significant correlations, they do not exhibit exceptionally high collinearity. Although cross-sectional dependence is detected for certain variables in the CD test (see Table 5), this finding does not inherently invalidate the use of pooled OLS, especially when robust standard errors can account for potential heteroskedasticity and cross-sectional dependence. The Fisher-type unit root test results (see Table 6) provide insights into the stationarity characteristics of the variables, and while some exhibit boundary behaviour, these outcomes do not preclude the application of pooled OLS.
Moreover, the VIF values (see Table 7) indicate a moderate level of multicollinearity, but none exceeds the threshold of concern. Finally, the lack of significant evidence to reject the null hypothesis of constant variance in the Breusch–Pagan/Cook–Weisberg test (see Table 8) supports the assumption of homoskedasticity, a fundamental assumption of OLS. In light of these findings, pooled OLS regression is justified as it aligns with the nature of the dataset and the absence of severe violations of OLS assumptions. Therefore, Table 9 shows pooled OLS and pooled OLS robust results.
The results of the analysis demonstrate the statistical significance of both models (F(10, 51) = 24.19 and 54.57, p < 0.0001), indicating a solid level of significance. The models also exhibit a high R-squared value of 0.8259, suggesting a good fit. The coefficients of the independent variables provide insights into their impact on the dependent variable, CDW. Specifically, the variable BCS exhibits a negative impact of (−0.0875) on CDW, implying a reduction in deaths caused by cancer in women in European countries. Similarly, WEP has a negative impact of (−0.0021), and LEW has a negative impact of (−5.2603), further contributing to reduced cancer-related deaths in women.
However, certain independent variables show a positive impact on CDW. For instance, HCE (+0.0311), FER (+0.3212), WLW (+0.6572), WHG (+0.4057), NSN (+0.2649), PAF (+0.2649), and UMN (+0.0325) are associated with an increase in deaths caused by cancer in women in European countries. The p-values associated with the coefficients indicate their statistical significance, with values below 0.05 considered significant. This case suggests that several variables significantly impact CDW while accounting for other independent variables in the model. These findings contribute to our understanding of factors influencing cancer-related deaths in women in European countries. Figure 7 summarizes the findings presented in the preceding table.

Summary of empirical results. The authors created this figure
In the following section, the results obtained from the empirical investigation will be discussed.
Discussion
The impact of breast and cervical cancer screening on reducing deaths from cancer in women across European countries highlights the importance of increased participation in screening programs. This positive outcome can be attributed to improved access to screening services, awareness campaigns promoting early detection, and the support of effective healthcare systems (Yang et al. 2022). Moreover, higher participation in these screening programs may reduce gender inequality, reflecting improved healthcare access and opportunities for women in these areas.
Similarly, the negative impact of higher education and participation in education and training on women's cancer-related deaths underscores the crucial role of education in improving health outcomes. Women with higher education levels tend to possess greater health literacy, access to information, and understanding of preventive measures (Gedefaw et al. 2020; Raghupathi and Raghupathi 2020; Vaccarella et al. 2023). Educational programs improve health literacy, raise awareness about cancer prevention, and enhance access to healthcare information and services (Del Carmen et al. 2021; Poudel et al. 2021). By promoting educational opportunities and providing comprehensive health education, we can contribute to lower mortality rates in European countries by empowering women to make informed decisions regarding cancer prevention, early detection, and lifestyle choices. Furthermore, the increasing number of women with higher education levels and access to educational programs suggests progress in reducing gender inequality in the educational sphere.
The negative impact of higher life expectancy in women on cancer-related deaths in European countries is encouraging, as it indicates improved overall health, better access to healthcare, advancements in cancer prevention, early detection, and more effective treatment options (Ranabhat et al. 2018; Hao et al. 2020). Additionally, this result implies that efforts to address gender inequality by promoting equal access to healthcare and health education may positively impact women's health outcomes. Nevertheless, to comprehend this issue fully, it is essential to consider other factors and indicators of gender inequality.
It must be noted that some independent variables positively impact cancer-related deaths in women. For instance, the positive correlation between total healthcare expenditure and cancer mortality suggests that despite higher healthcare expenditures, inefficiencies or gaps in healthcare systems might exist, leading to delayed diagnosis, inadequate treatment, or suboptimal healthcare outcomes (Prentice and Pizer 2007).
This unexpected impact on cancer mortality rates in certain European countries can be linked to their relatively low healthcare expenditure per capita. In 2020, several European countries, including Lithuania, Slovakia, Latvia, Hungary, Poland, Croatia, Bulgaria, and Romania, exhibited lower healthcare expenditure levels than anticipated (Eurostat 2023c). Thus, reduced healthcare spending can contribute to an increase in cancer mortality rates through various mechanisms, such as limited access to healthcare services, delayed diagnosis and treatment, reduced investment in screening and prevention, compromised quality of care, and inadequate supportive services (e.g., McKee et al. 2012; Allemani et al. 2018; Jemal et al. 2011). This result raises concerns about potential gender inequality within healthcare systems, such as disparities in access to quality care or barriers to timely diagnosis and treatment for women.
The positive impact of the full-time equivalent employment (FTE) rate in women on cancer-related deaths indicates that a higher full-time employment rate may contribute to increased stress levels, unhealthy behaviours, and neglect of personal health (Trudel-Fitzgerald et al. 2017). These factors could lead to a higher incidence of cancer and, consequently, increased mortality among women in European countries.
Furthermore, the positive impact of women participating in sporting, cultural, or leisure activities outside their homes could be associated with low daily or weekly participation of women in sporting, cultural, or leisure activities outside their homes. This lack of regular physical activity contributes to a sedentary lifestyle, which increases the risk of chronic conditions, including cancer. Factors such as societal norms, time constraints, limited access to resources and facilities, safety concerns, and gender stereotypes contribute to lower engagement in these activities (Park et al. 2020; World Cancer Research Fund/American Institute for Cancer Research 2018; Eurofound 2016; European Commission 2017). Addressing these barriers requires comprehensive efforts to promote gender equality, provide inclusive and affordable recreational opportunities, improve access to facilities, challenge stereotypes, and create safe and supportive environments for women to engage in sporting, cultural, and leisure activities.
The unexpected positive impact of women who do not smoke and are not involved in harmful drinking on cancer-related deaths in women requires careful interpretation. While not smoking and avoiding excessive alcohol consumption are generally protective factors against cancer, it is essential to consider the influence of gender differences in alcohol consumption and smoking habits. Women typically consume less alcohol and smoke less than men. Nevertheless, recent increases in alcohol and tobacco consumption among women (White 2020) suggest the need to carefully consider these results, as other confounding variables and unaccounted risk factors could influence the relationship. Cultural and societal influences, as well as variations in alcohol consumption patterns across countries, may also contribute to the unexpected nature of this relationship.
The positive impact of women engaging in physical activities and/or consuming fruits and vegetables on cancer-related deaths suggests that reported levels of physical activity and fruit and vegetable consumption alone may not be sufficient to counteract other risk factors or offer substantial protection against cancer (Donaldson 2004). Moreover, multiple factors contribute to the limited participation of women in physical activities and their consumption of fruits and vegetables within European countries. These factors include sociocultural norms, ingrained gender stereotypes, limited access to facilities and resources, time constraints impacting work/life balance, a lack of knowledge and awareness, and concerns related to body image and societal pressures (Eurostat 2018; European Commission 2017; Eurofound 2016; Baskin and Galligan 2019).
Furthermore, it is essential to acknowledge the influence of education levels in this context. As emphasized by Pem and Jeewon (2015) and Assari and Lankarani (2018), individuals with lower levels of education often face barriers to accessing proper nutritional education. They may encounter misinformation regarding the significance of maintaining healthy dietary habits, especially fruit and vegetable consumption. As a result, this misinformation can substantially impact their actual dietary choices.
Considering that certain European countries report lower levels of education among women, it is plausible that this educational disparity plays a role in the observed patterns of fruit and vegetable consumption. Additionally, lower educational attainment is associated with reduced physical activity participation, as Droomers et al. (2001) highlighted.
Low income is likely another factor contributing significantly to this situation. Assari and Lankarani (2018) highlight that limited financial resources often lead individuals to prioritize more affordable, calorie-dense foods over fresh produce. Processed and less healthy options frequently provide more calories per dollar, making them an attractive budget choice. Moreover, fresh fruits and vegetables can be relatively expensive, particularly in areas with limited access to affordable produce. This situation can deter individuals with lower incomes from regularly purchasing these items. In the context of women's circumstances, the prevailing gender pay gaps within Europe may significantly impact women's economic well-being, potentially making it more challenging for them to afford nutritious food options. Consequently, women with lower education and income levels may face compounded financial barriers when purchasing fruits and vegetables.
The impact of self-perceived health on cancer deaths in women may be linked to a false sense of security. Women who perceive themselves as healthy may delay cancer screening and timely medical attention, leading to advanced stages of cancer and higher mortality rates (Nonzee et al. 2015). This issue may also reflect gender inequality, with limited healthcare access, educational disparities, and societal expectations influencing women's healthcare decisions. Addressing these disparities is crucial for equal access to resources, awareness, and timely care.
The impact of unmet need for medical examinations among women on cancer-related deaths is alarming. This increase in unmet medical need is closely linked to limited healthcare access, waiting lists, financial barriers, geographical distance, and inadequate awareness (Collins et al. 2019). In European countries, different age groups reported varying percentages of unmet medical need, with older age groups commonly citing expenses, distance, and waiting lists as the prevalent reasons (Eurostat 2023d).
The specific reasons for unmet medical need varied among European countries. For instance, the expense was the most common barrier in several countries, including Belgium, Bulgaria, Greece, France, Italy, Cyprus, Latvia, Luxembourg, Austria, Portugal, and Romania. Waiting lists were the primary issue in Estonia, Ireland, Spain, Lithuania, Poland, Slovenia, Slovakia, Finland, Sweden, and Norway. In Czechia, Denmark, Germany, Croatia, Hungary, Malta, the Netherlands, and Switzerland, individuals preferred to wait and see whether the problem was resolved independently (Eurostat 2023d).
Furthermore, this situation may also be linked to the low proportions of women aged 50 to 69 undergoing breast and cervical cancer screening. Possible barriers that hinder the realization of this screening and the previously identified low investments in healthcare could contribute to this phenomenon.
In conclusion, the findings discussed above provide valuable insights into the relationship between gender inequality and deaths from cancer in women in European countries, confirming hypothesis H1. This research underscores the fact that greater gender inequality in these nations influences cancer mortality rates among women through disparities in education, socioeconomic status, healthcare access, and risk behaviours. Specifically, it demonstrates that higher levels of gender inequality may result in limited education and awareness, promote unhealthy behaviours, and impede healthcare access, all collectively contributing to higher cancer mortality rates.
The findings of this investigation align with a substantial body of existing research (Donington and Colson 2011; OECD 2015; Gavurova et al. 2020; Willems et al. 2020; Jolidon 2022; and Vaccarella et al. 2023), providing robust support for hypothesis H1. They reveal that disparities in education and socioeconomic status can hinder women's ability to make informed decisions regarding cancer prevention, early detection, and healthy lifestyle choices. Furthermore, limited access to healthcare services, coupled with gender-related barriers, can lead to delayed diagnosis and inadequate treatment. These barriers collectively contribute to the observed higher cancer mortality rates in women, particularly in countries with greater gender inequality.
This study's methodological rigour and the acknowledgement of its limitations, including the exclusion of certain variables due to multicollinearity, further strengthen the credibility of the findings. However, it is important to note that this investigation focused on a specific set of variables and that other factors may also play a role in cancer outcomes. To comprehensively address the complex interplay between gender inequality and cancer outcomes, further research should explore additional indicators of gender inequality and consider various factors influencing cancer outcomes. This will allow us to gain a deeper understanding of the impact of gender inequality on women's health and inform evidence-based strategies to improve healthcare access, awareness, and outcomes, ultimately working towards a more equitable society.
In light of this research, hypothesis H0, which suggests that lower levels of gender inequality are not significantly associated with increased cancer mortality rates among women in European countries, is not supported. The findings of this study provide compelling evidence that gender inequality indeed has a significant impact on women's cancer mortality rates within the European context.
In conclusion, the findings discussed above provide valuable insights into the link between gender inequality and deaths from cancer in women in European countries. The results support hypothesis (1), which suggests that higher levels of gender inequality, specifically in terms of disparities in socioeconomic status, healthcare access, and risk behaviours, are associated with increased mortality rates in women with cancer. The exclusion of certain variables due to multicollinearity emphasizes the study's methodological rigour and acknowledges its limitations, ultimately strengthening the credibility of the findings. Further research should explore additional indicators of gender inequality and consider various factors influencing cancer outcomes to comprehensively address the complex interplay between gender inequality and cancer outcomes. By doing so, we can gain a deeper understanding of the impact of gender inequality on women's health and inform evidence-based strategies to improve healthcare access, awareness, and outcomes, ultimately working towards a more equitable society.
Conclusions
In conclusion, this study has undertaken a comprehensive and rigorous examination of the empirical data, providing valuable insights into the intricate relationship between gender inequality and cancer mortality among women in European countries. The investigation embarked upon a systematic exploration, commencing with foundational preliminary tests that laid the groundwork for subsequent sophisticated analyses. This approach ensured that the findings were rooted in a solid methodological framework, enhancing the credibility and significance of the outcomes.
The initial presentation of preliminary tests established a robust foundation for the subsequent pooled OLS regression analysis. The study ensured a nuanced understanding of the data by scrutinizing the variables' distribution and attributes in Table 2 and visually depicting their characteristics using Fig. 6. The identification of potential skewness, kurtosis, and outliers, supported by histograms, further enhanced the rigour of the investigation. The subsequent pairwise correlation test, as illustrated in Table 3, provided a glimpse into associations among variables and shed light on potential interdependencies that could influence the subsequent analytical approach.
The endeavour to assess the normality of variable distributions through the skewness/kurtosis tests (Table 4) offered significant insights by highlighting deviations from the normal distribution for certain variables. These insights paved the way for the Pesaran CD test (Table 5), which uncovered cross-sectional dependence in the residuals of specific variables, thereby guiding the selection of appropriate analytical strategies. The Fisher-type unit root test (Table 6) further enriched the analysis by revealing the diverse stationarity properties of the variables, emphasizing the dataset's nuanced nature.
Crucially, multicollinearity concerns were addressed through the VIF test (Table 7), which demonstrated a moderate level of multicollinearity without breaching critical thresholds. Similarly, the Breusch–Pagan/Cook–Weisberg test for heteroskedasticity (Table 8) affirmed the suitability of employing pooled OLS regression, reinforcing the reliability of the chosen analytical approach.
The subsequent pooled OLS regression results (Table 9) not only substantiated the significance of the models but also highlighted their robustness. The results of the analysis demonstrate the statistical significance of both models (F(10, 51) = 24.19 and 54.57, p < 0.0001), indicating a solid level of significance. The models also exhibit a high R-squared value of 0.8259, suggesting a good fit. The coefficients of the independent variables provide insights into their impact on the dependent variable, CDW. Specifically, variables like BCS exhibit a negative impact of (−0.0875) on CDW, implying a reduction in deaths caused by cancer in women in European countries. Similarly, WEP has a negative impact of (−0.0021), and LEW has a negative impact of (−5.2603), further contributing to reduced cancer-related deaths in women. However, certain independent variables show a positive impact on CDW. For instance, HCE (+0.0311), FER (+0.3212), WLW (+0.6572), WHG (+0.4057), NSN (+0.2649), PAF (+0.2649), and UMN (+0.0325) are associated with an increase in deaths caused by cancer in women in European countries.
The findings advance the current knowledge state and resonate within a broader context. The meticulous discussion and contextualization of the results within the framework of gender inequality and healthcare outcomes illuminate the intricate interplay between these factors and cancer mortality. The multifaceted relationship unveiled through this study demonstrates protective and adverse impacts across various dimensions, expanding our comprehension of this complex issue.
This investigation makes substantial theoretical contributions by shedding light on the intricate nexus between gender inequality and cancer-related deaths among women in European countries. The study underscores the significance of preventive healthcare measures, such as cancer screening, in reducing mortality rates and emphasizes the broader implications of gender disparities within healthcare systems. The research elucidates how higher educational attainment can empower women with health literacy and informed decision-making capabilities by linking education to health outcomes. Additionally, the study delves into the intricate interplay between societal factors and health, revealing how employment rates and lifestyle choices can influence stress levels and ultimately impact cancer mortality. By uncovering unexpected relationships, the research highlights the complexities of health behaviours and the importance of nuanced interpretations. Ultimately, the findings collectively contribute to a comprehensive understanding of how gender inequality manifests in health outcomes and offer actionable insights for policy interventions that can mitigate disparities and enhance women's health in European societies.
Policy implications
The insights from this study bear profound implications for developing effective policy frameworks and intervention strategies to curb cancer mortality rates among women across European nations. Recognizing the multifaceted nature of gender inequality is pivotal in attaining enhanced health outcomes. In light of the findings, the following policy recommendations emerge as valuable considerations:
-
I.
Priority should be accorded to policies that strive to diminish the prevailing socioeconomic inequalities that underpin gender-driven discrepancies in healthcare access and outcomes. Initiatives geared toward fostering economic empowerment, educational advancement, and equitable opportunities for women are instrumental in mitigating the adverse influence of socioeconomic factors on cancer mortality rates.
-
II.
Policy interventions must zero in on guaranteeing equitable access to high-quality healthcare services for all women. This endeavour entails dismantling barriers that hinder prompt diagnosis, effective treatment, and comprehensive follow-up care. Propagating awareness about accessible healthcare resources and bolstering healthcare infrastructure can culminate in improved outcomes for women navigating the challenges of cancer.
-
III.
Addressing risk behaviours that contribute to the exacerbation of cancer mortality rates is of paramount significance. Tailored public health campaigns and educational initiatives should be meticulously crafted to foster wholesome lifestyles and behaviours among women. Emphasis should be placed on critical determinants such as tobacco use, alcohol consumption, physical activity, and nutrition, empowering women to make informed choices that positively impact their health trajectories.
-
IV.
Policies must be implemented to support underprivileged women financially, ensuring that cost is not a barrier to cancer screening and treatments. This support could include subsidies, insurance coverage, or vouchers for screening.
-
V.
Cancer prevention and screening should be integrated into maternal and child health programs. These integrated services can reach women during pregnancy and childcare, emphasizing the importance of screening and healthy behaviours.
-
VI.
Ensuring that women are adequately represented in cancer treatments, medications, and therapies in clinical trials is critical. This helps tailor treatments to women's specific needs and ensures that they have access to cutting-edge therapies.
-
VII.
Palliative care programs should be developed that are sensitive to the unique physical and emotional needs of women with advanced cancer. Palliative care should aim to improve the quality of life for women living with cancer.
-
VIII.
Networking and peer support groups for women with cancer are important. These groups can provide emotional support, share experiences, and promote a sense of community among women facing similar challenges.
-
IX.
We must invest in comprehensive cancer screening programs that specifically target women's health needs. These programs should include regular mammograms and cervical cancer screening and should ensure that these services are accessible and affordable.
-
X.
The use of telehealth and telemedicine services should be promoted, making it easier for women to access healthcare consultations and follow-ups, especially in underserved or remote areas.
If implemented, these policy recommendations have the potential to save the lives of 800,000 women a year by significantly reducing the number of deaths caused by gender inequality in cancer outcomes. By prioritizing policies that address socioeconomic inequalities, ensuring equitable access to high-quality healthcare services, promoting healthy behaviours, providing financial support, integrating cancer prevention into maternal and child health programs, enhancing women's representation in clinical trials, developing sensitive palliative care programs, fostering supportive networks, and investing in comprehensive cancer screening programs, we can create a healthcare landscape that is fairer, more accessible, and tailored to women's specific needs. Moreover, by promoting the use of telehealth and telemedicine services, we can bridge gaps in healthcare access for women in underserved or remote areas. These policies not only stem from empirical research but also carry the potential to yield a profound positive impact, ultimately saving the lives of 800,000 women each year while promoting gender equity and improving overall health outcomes in European countries.
Limitations and future research
The study acknowledges inherent limitations arising from its reliance on secondary data sources, potentially leading to inaccuracies and variations in cancer mortality rates and gender inequality indicators. For future research, establishing collaborations with international organizations to implement standardized data collection methodologies could significantly enhance data accuracy and maintain consistency. It is essential to recognize that the generalizability of the findings is restricted to European countries, and the direct applicability to regions with distinct sociocultural contexts and healthcare systems may be limited. Indeed, to address this shortcoming, future investigations could encompass a more diverse range of countries, thereby validating the cross-cultural significance of the observed associations.
The study's observational design precludes establishing a causal relationship between gender inequality and cancer mortality. Future research could explore experimental or quasi-experimental designs to provide more robust evidence of causality. Moreover, diligent efforts to control for unmeasured confounding variables could bolster the accuracy and validity of the findings. Future studies could incorporate a comprehensive array of gender inequality indicators and delve into the multifaceted factors influencing the observed associations to broaden the scope of inquiry. This approach might entail examining genetic predispositions, environmental exposures, and individual lifestyle choices that potentially contribute to the variation in cancer mortality rates among women.
Conducting longitudinal studies would be invaluable to gain deeper insights into the dynamics over time. Longitudinal analysis could shed light on the intricate interplay between changes in gender inequality and healthcare policies and their evolving impact on cancer mortality rates. By investigating temporal trends, these analyses could provide a clearer understanding of the underlying mechanisms driving these associations.
This study contributes noteworthy insights into the intricate relationship between gender inequality and cancer mortality among European women. Acknowledging and addressing its limitations while also propelling future research endeavours holds the potential to refine our comprehension of these critical issues. This approach, in turn, can guide evidence-based strategies to advance women's health and foster equitable societies on a broader scale.
Data availability
Some or all data and models that support the findings of this study are available from the corresponding author upon reasonable request.
Code availability
The analyses were performed using Stata 17.0 (Licence number 58799).
References
Akinyemiju TF, McDonald JA, Lantz PM (2015) Health care access dimensions and cervical cancer screening in South Africa: analysis of the world health survey. BMC Public Health 15:382. https://doi.org/10.1186/s12889-015-1686-5
Allemani C, Matsuda T, Di Carlo V, Harewood R, Matz M, Nikšić M, Bonaventure A, Valkov M, Johnson CJ, Estève J, Ogunbiyi OJ, Azevedo E Silva G, Chen WQ, Eser S, Engholm G, Stiller CA, Monnereau A, Woods RR, Visser O et al (2018) Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 391(10125):1023–1075. https://doi.org/10.1016/S0140-6736(17)33326-3
Allen J, Sesti F (2018) Health inequalities and women – addressing unmet needs. British Med Assoc (BMA), 1-12
Anand P, Kunnumakkara AB, Sundaram C, Harikumar KB, Tharakan ST, Lai OS, Sung B, Aggarwal BB (2008) Cancer is a preventable disease that requires major lifestyle changes. Pharm Res 25(9):2097–2116. https://doi.org/10.1007/s11095-008-9661-9
Assari S, Lankarani MM (2018) Educational Attainment Promotes Fruit and Vegetable Intake for Whites but Not Blacks. J (Basel) 1(1):29–41. https://doi.org/10.3390/j1010005
Baltagi BH (2013) Econometric Analysis of Panel Data, 5th ed. Wiley
Baskin R, Galligan R (2019) Disordered eating and the perinatal period: A systematic review and best evidence synthesis of mental health and psychosocial correlates. https://doi.org/10.1002/erv.2675
Belsley DA, Kuh E, Welsch RE (1980) Regression Diagnostics: Identifying Influential Data and Sources of Collinearity. Wiley
Bird CE, Rieker PP (2008) Gender and Health: the Effects of Constrained Choices and Social Policies. Cambridge University Press, Cambridge
Borrell C, Palencia L, Muntaner C et al (2014) Influence of macrosocial policies on women's health and gender inequalities in health. Epidemiol Rev 36(2014):31–48
Bosetti C, Malvezzi M, Chatenoud L, Negri E, Levi F, La Vecchia C (2013) Cancer mortality in Europe, 2005–2009, and an overview of trends since 1980. Ann Oncol 24(10):2657–2671. https://doi.org/10.1093/annonc/mdt301
Breusch TS, Pagan AR (1979) A simple test for heteroscedasticity and random coefficient variation. Econometrica 47:1287–1294. https://doi.org/10.2307/1911963
Cesario SK (2012) Global Inequalities in the Care of Women With Cancer. Nurs Women’s Health. https://doi.org/10.1111/J.1751-486X.2012.01761.X
Chan JE, Caesar MA, Mann AK, Koh-Bell A, Richardson MT, Johnson CR, Kapp DS, Chan JK (2022) The role of diet compared to physical activity on women's cancer mortality: Results from the Third National Health and Nutrition Examination Survey. Front Public Health 10:853636. https://doi.org/10.3389/fpubh.2022.853636
Collins J, Bowie D, Shannon G (2019) A descriptive analysis of health practices, barriers to healthcare, and the unmet need for cervical cancer screening in the Lower Napo River region of the Peruvian Amazon. Womens Health (Lond) 15:1745506519890969. https://doi.org/10.1177/1745506519890969
Cook RD, Weisberg S (1983) Diagnostics for heteroscedasticity in regression. Biometrika 70:1–10. https://doi.org/10.1093/biomet/70.1.1
D'Agostino RB, Pearson ES (1973) Tests for departure from normality. Biometrika 60:613–622. https://doi.org/10.2307/2335409
Del Carmen OJM, Emilia GRD, Mares BH, Marcela OJ (2021) Educational interventions on breast cancer in men and women: a necessity in primary healthcare. Ecancer 15:1255. https://doi.org/10.3332/ecancer.2021.1255
Donaldson MS (2004) Nutrition and cancer: a review of the evidence for an anti-cancer diet. Nutr J 3(19):1–21. https://doi.org/10.1186/1475-2891-3-19
Donington JS, Colson YL (2011) Sex and gender differences in non-small cell lung cancer. Sem Thor Cardiovasc Surg. https://doi.org/10.1053/J.SEMTCVS.2011.07.001
Droomers M, Schrijvers CTM, Mackenbach JP (2001) Educational level and decreases in leisure time physical activity: predictors from the longitudinal GLOBE study journal of. Epidemiol Commun Health 55:562–568
ECIS (2023) European Cancer Information System. Retrieved from https://ecis.jrc.ec.europa.eu/explorer.php?$0-0$1-AE27$4-2$3-All$6-0,85$5-2020,2020$7-8$CEstByCancer$X0_8-3$CEstRelativeCanc$X1_8-3$X1_9-AE27$CEstBySexByCancer$X2_8-3$X2_-1-1. Accessed 12 June 2023
Eurofound (2016) European Quality of Life Survey. Retrieved from https://www.eurofound.europa.eu/surveys/european-quality-of-life-surveys/european-quality-of-life-survey-2016. Accessed 12 June 2023
European Commission (2017) Sport and physical activity. Retrieved from https://ec.europa.eu/sport/policy/sport-and-physical-activity_en. Accessed 12 June 2023
European Commission (2020) Gender Equality. Retrieved from https://ec.europa.eu/info/policies/justice-and-fundamental-rights/gender-equality_en. Accessed 12 June 2023
European Institute for Gender Equality (EIGE) (2023a) Gender inequality. 2023. Retrieved from https://eige.europa.eu/publications-resources/thesaurus/terms/1329?language_content_entity=en. Accessed 12 June 2023
European Institute for Gender Equality (EIGE) (2023b) Gender inequality. Retrieved from https://eige.europa.eu/publications-resources/thesaurus/terms/1329?language_content_entity=en. Accessed 12 June 2023
Eurostat (2018) Women and Men in the EU: Statistics on Gender Equality. Retrieved from https://ec.europa.eu/eurostat/statistics-explained/index.php/Women_and_Men_in_the_EU_-_Statistics_on_gender_equality. Accessed 12 June 2023
Eurostat (2023a) Death due to cancer. Retrieved from https://ec.europa.eu/eurostat/databrowser/view/TPS00116/default/table. Accessed 12 June 2023
Eurostat (2023b) Total health care expenditure. Retrieved from https://ec.europa.eu/eurostat/databrowser/view/TPS00207/default/table. Accessed 12 June 2023
Eurostat (2023c) Healthcare expenditure statistics. Retrieved from https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Healthcare_expenditure_statistics#Healthcare_expenditure. Accessed 12 June 2023
Eurostat (2023d) Unmet needs for medical care. Retrieved from https://ec.europa.eu/eurostat/statistics-explained/index.php/Unmet_needs_for_medical_care. Accessed 12 June 2023
Fisher RA (1925) Statistical methods for research workers. Oliver and Boyd, Edinburgh, Scotland
Gavurova B, Ivankova V, Rigelsky M, Suhanyi L (2020) Impact of Gender Inequalities in the Causes of Mortality on the Competitiveness of OECD Countries. Int J Environ Res Public Health 17(10):3698. https://doi.org/10.3390/ijerph17103698
Gedefaw A, Yilma TM, Endehabtu BF (2020) Information seeking behavior about cancer and associated factors among university students, Ethiopia: A cross-sectional study. Cancer Manag Res 12:4829–4839. https://doi.org/10.2147/CMAR.S259849
Greene WH (2012) Econometric analysis, 7th edn. Pearson Education, Boston, MA
Hao L, Xu X, Dupre ME et al (2020) Adequate access to healthcare and added life expectancy among older adults in China. BMC Geriatr 20(129):1–15. https://doi.org/10.1186/s12877-020-01524-9
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D (2011) Global cancer statistics. CA: A Cancer J Clin 61(2):69–90. https://doi.org/10.3322/caac.20107
Jolidon V (2022) Gender inequality and mammography screening: Does living with a partner improve women's mammography uptake? Social Sci Med 298:114875. https://doi.org/10.1016/j.socscimed.2022.114875
Jolliffe IT (2002) Principal component analysis. 2nd ed. Springer
Kerschbaum E, Nüssler V (2019) Cancer prevention with nutrition and lifestyle. Visceral Med 35(4):204–209. https://doi.org/10.1159/000501776
Korn L, Gonen E, Shaked Y, Golan M (2013) Health perceptions, self and body image, physical activity, and nutrition among undergraduate students in Israel. PLoS One 8(3):e58543. https://doi.org/10.1371/journal.pone.0058543
Liu L, Shi Y, Li T, Qin Q, Yin J, Pang S, Nie S, Wei S (2016) Leisure time physical activity and cancer risk: evaluation of the WHO's recommendation based on 126 high-quality epidemiological studies. Br J Sports Med 50(6):372–378. https://doi.org/10.1136/bjsports-2015-094728
Lugo A, Zuccaro P, Pacifici R et al (2017) Smoking in Italy in 2015-2016: Prevalence, trends, roll-your-own cigarettes, and attitudes towards incoming regulations. Tumori 103(4):353–359. https://doi.org/10.5301/tj.5000644
McKee M, Karanikolos M, Belcher P, Stuckler D (2012) Austerity: A failed experiment on the people of Europe. Clin Med 12(4):346–350. https://doi.org/10.7861/clinmedicine.12-4-346
Mobaraki AEH, Soderfeldt B (2010) Gender inequity in Saudi Arabia and its role in public health. EMHJ - Eastern Mediterranean Health J 16(1):113–118. https://apps.who.int/iris/handle/10665/117827
Nonzee NJ, Ragas DM, Ha Luu T, Phisuthikul AM, Tom L, Dong X, Simon MA (2015) Delays in cancer care among low-income minorities despite access. J Womens Health 24(6):506–514. https://doi.org/10.1089/jwh.2014.4998
OECD (2015) Gender gaps in cancer mortality remain large in OECD countries, but starting to narrow. https://www.oecd.org/gender/data/gender-gaps-in-cancer-mortality-remain-large-in-oecd-countries-but-starting-to-narrow.htm. Accessed 12 June 2023
Osamor PE, Grady C (2016) Women's autonomy in health care decision-making in developing countries: a synthesis of the literature. Int J Womens Health 8(2016):191–202
Park JH, Moon JH, Kim HJ, Kong MH, Oh YH (2020) Sedentary lifestyle: Overview of updated evidence of potential health risks. Korean J Fam Med 41(6):365–373. https://doi.org/10.4082/kjfm.20.0165
Pem D, Jeewon R (2015) Fruit and Vegetable Intake: Benefits and Progress of Nutrition Education Interventions- Narrative Review Article. Iran J Public Health 44(10):1309–1321
Pesaran MH (2004) General diagnostic tests for cross section dependence in panels. Cambridge Working Papers in Economics, No. 0435. https://doi.org/10.1017/S026646660420307
Poudel K, Sumi N, Yano R (2021) Impact of peer-led cancer education program on knowledge, health beliefs, practice, and self-esteem among pairs of Nepalese High-School students and their knowledge-sharing partners. Healthcare 9(1):64. https://doi.org/10.3390/healthcare9010064
Prentice JC, Pizer SD (2007) Delayed access to health care and mortality. Health Serv Res 42(2):644–662. https://doi.org/10.1111/j.1475-6773.2006.00626.x
Quintal C, Moura Ramos L, Antunes M, Lourenço Ó (2023) Unmet healthcare needs among the population aged 50+ and their association with health outcomes during the COVID-19 pandemic. Eur J Ageing 20(1):12. https://doi.org/10.1007/s10433-023-00758-x
Raghupathi V, Raghupathi W (2020) The influence of education on health: An empirical assessment of OECD countries for the period 1995–2015. Arch Public Health 78:1–18. https://doi.org/10.1186/s13690-020-00402-5
Ranabhat CL, Atkinson J, Park M-B, Kim C-B, Jakovljevic M (2018) The influence of universal health coverage on life expectancy at birth (LEAB) and healthy life expectancy (HALE): A multi-country cross-sectional study. Front Pharmacol 9:960. https://doi.org/10.3389/fphar.2018.00960
Schnohr P, Grønbaek M, Petersen L, Hein HO, Sørensen TI (2005) Physical activity in leisure-time and risk of cancer: 14-year follow-up of 28,000 Danish men and women. Scand J Public Health 33(4):244–249. https://doi.org/10.1080/14034940510005752
Starfield B, Shi L, Macinko J (2005) Contribution of primary care to health systems and health. Milbank Q 83(3):457–502. https://doi.org/10.1111/j.1468-0009.2005.00409.x
Trudel-Fitzgerald C, Poole EM, Idahl A, Lundin E, Sood AK, Kawachi I, Kubzansky LD, Tworoger SS (2017) The association of work characteristics with ovarian cancer risk and mortality. Psychosom Med 79(9):1059–1067. https://doi.org/10.1097/PSY.0000000000000464
UNDP (United Nations Development Programme) (2022) Human Development Report 2021/2022: Uncertain Times, Unsettled Lives: Shaping our Future in a Transforming World. New York
Vaccarella S, Georges D, Bray F, Ginsburg O, Charvat H (2023) Socioeconomic inequalities in cancer mortality between and within countries in Europe: a population-based study. Lancet Reg Health Eur 25:100551. https://doi.org/10.1016/j.lanepe.2022.100551
White AM (2020) Gender differences in the epidemiology of alcohol use and related harms in the United States. Alcohol Res 40(2). https://doi.org/10.35946/arcr.v40.2.01
Willems SB, Cullati VP et al (2020) Cancer screening participation and gender stratification in Europe. J Health Soc Behav 61:377–395
Williams A, Erb-Downward J, Bruzelius E, O'Hara-Cicero E, Maling A, Machin L, Viera-Delgado M, Valera P, Maysonet N, Weiss ES (2013) Exploring cancer screening in the context of unmet mental health needs: A participatory pilot study. Prog Commun Health Partnersh 7(2):123–134. https://doi.org/10.1353/cpr.2013.0027
Wooldridge JM (2002) Econometric analysis of cross-section and panel data. MIT Press, Cambridge, MA
Wooldridge J (2015) Introductory Econometrics: A Modern Approach. Nelson Education
World Cancer Research Fund/American Institute for Cancer Research (2018) Diet, Nutrition, Physical Activity and Cancer: A Global Perspective. Continuous Update Project Expert Report. Retrieved from https://www.wcrf.org/dietandcancer. Accessed 12 June 2023
World Health Organization (WHO) (2021) Gender and health. Retrieved from https://www.who.int/news-room/questions-and-answers/item/gender-and-health.. Accessed 12 June 2023
Yang Z, Liu J, Wang Q (2022) Diagnose earlier, live longer? The impact of cervical and breast cancer screening on life span. PLoS One 17(7):e0270347. https://doi.org/10.1371/journal.pone.0270347
Funding
Open access funding provided by FCT|FCCN (b-on). UCILeR is an R&D unit accredited and funded by FCT—Portugal National Agency within the scope of its strategic project: UIDB/04643/2020. CeBER: R&D unit funded by National Funds through FCT—Fundação para a Ciência e a Tecnologia, I.P., project UIDB/05037/2020.
Author information
Authors and Affiliations
Contributions
M.K: Conceptualization, Methodology, Writing—original draft preparation, Supervision, Validation, Data curation, Investigation, Formal analysis, Visualization. J.A.F: Reviewing, Editing, and Investigation. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Conflicts of interest/Competing interests
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Koengkan, M., Fuinhas, J.A. The influence of gender inequality on women’s cancer mortality in European countries: a quantitative study. J Public Health (Berl.) (2023). https://doi.org/10.1007/s10389-023-02175-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10389-023-02175-x