
Abstract
Aim
To analyze the worldwide epidemiology of lip and oral cavity cancer attributable to smoking.
Methods
The worldwide epidemiology of lip and oral cavity cancer attributable to smoking and its spatial distribution differences were analyzed using the age-standardized mortality rate, age-standardized disability-adjusted life years (DALYs) rate, and estimated annual percent change (EAPC) according to information from the Global Burden of Disease Study 2019.
Results
The number of deaths and DALYs associated with lip and oral cavity cancer attributable to smoking globally showed upward trends from 1990 to 2019, but the age-standardized mortality and DALYs rates decreased. The age-standardized mortality rate gradually increased with age. The age-standardized mortality and DALYs rates were markedly higher in low-middle social development index (SDI) regions than in other regions. The age-standardized mortality and DALYs rates showed slight increasing trends (EAPC = 0.16 and 0.07, respectively) in middle-SDI regions and the greatest decrease (EAPC = –1.60 and –1.74, respectively) in high-SDI regions. The three regions with the highest age-standardized mortality and DALYs rates were South Asia (1.59; 39.68), Eastern Europe (1.33; 40.59), and Central Europe (1.30; 37.67), but the largest increases were observed in East Asia (EAPC = 2.32, EAPC = 2.30), the Northern Mariana Islands (EAPC = 3.79, EAPC = 3.67), and Cabo Verde (EAPC = 2.84; DALY, EAPC = 3.38).
Conclusion
The overall disease burden attributable to smoking is decreasing, but the number of deaths and DALYs are still increasing. Moreover, there are regional and national differences, and high-risk regions and countries should implement targeted interventions to reduce the burden.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Lip and oral cavity cancer is one of the most common malignancies of the head and neck. According to a global report, approximately 581,100 new oral cancer cases were documented globally in 2018, accounting for 3.20% of all new cancer cases. Further, there were approximately 285,500 oral-cancer-related deaths in the same year, accounting for 3.00% of global cancer deaths in that year (Collaborators 2020). The prognosis of patients with lip and oral cavity cancer is related to the local economy and level of medical care. Therefore, in less economically developed countries and regions, it imposes a serious influence on patients (Collaborators 2021).
There are numerous unfavorable aspects for lip and oral cavity cancer, including smoking, excessive alcohol drinking, betel nut consumption, a high body mass index, and oral mucosal disease (Brathwaite et al. 2015; Collaborators 2021). Smoking is one of the greatest significant unfavorable factors for precancerous lesions and cancerous diseases of the lips and oral cavity. Studies have shown that the risk of head and neck cancer is positively associated with the frequency of smoking and the number of years of smoking (Bray et al. 2018). The prevalence of oral tumors is 4–7 times higher in smokers than in nonsmokers (Gakunga and Parkin 2015). Smokeless tobacco use and smoking are the major unfavorable factors for lip and oral cavity cancer in India, accounting for 33.2% and 20.9% of oral cancer disability-adjusted life years (DALYs), respectively (Goodchild et al. 2018). A study in the United States showed that almost 50% of deaths from lip and oral cavity cancer are attributable to smoking (Gupta et al. 2017). A study by Zhang et al. (Harrison et al. 2021) showed that most of the mortality and DALYs associated with lip and oral cavity cancer in China are attributable to smoking.
The worldwide epidemiology of lip and oral cavity cancer attributable to smoking has not been reported. Therefore, we utilized GBD 2019 data to quantify the worldwide epidemiology of lip and oral cavity cancer attributable to smoking by calculating the annual percent change (EAPC) by age, sex, and social development index (SDI) from 1990 to 2019.
Methods
The GBD 2019 database provides an all-inclusive evaluation of 369 diseases and injuries (Hashibe et al. 2007). In this study, the number of deaths, number of DALYs, age-standardized morality rate, and age-standardized DALYs rate from 1990 to 2019 were obtained from the GBD 2019 database. Data were extracted by country, region, and sociodemographic index (SDI), and the analysis was stratified by 5-year age groups and sex. The study was approved by the Medical Ethics Committee of Beilun District People’s Hospital.
GBD 2019 used a new composite indicator, SDI, which is based on per-capita income, the average amount of years of schooling, and the total fertility rate, to assess the burden of disease in different regions (Hashibe et al. 2007). According to the SDI value, 204 countries or regions were classified into the following five regions: low SDI, low-middle SDI, middle SDI, high-middle SDI, and high SDI.
Estimation framework
According to the theoretical structure of comparative risk assessment, GBD 2019 estimated the proportion of disease burden caused by a risk factor in a given population by comparing the exposure distribution of that risk factor with the theoretical minimum risk exposure distribution, assuming that the exposure levels of other risk factors remain unchanged (Hashibe et al. 2007).
Statistical analysis
The age-standardized rate was used to reduce the effects of age structure. The age-standardized rate can be fitted to a regression line, i.e., ln (age-standardized rate) = α + βx + ε, where x = the calendar year. The EAPC was estimated as 100 × (exp (β) − 1), and the 95% confidence interval (CI) for the EAPC was also generated from this model (Liu et al. 2019). Case data (per 10,000 people) are presented with 95% CIs. Differences were regarded as significance at a two-sided P-value < 0.05, and all analyses were performed using the R language (R core team, version 3.5.2).
Results
Global DALYs and mortality
The global number of deaths in patients with lip and oral cavity cancer attributable to smoking in 1990 was 37,406.69, with an age-standardized mortality rate of 0.94 (95% CI 0.80, 1.10), while the global number of DALYs was 1,040,593.38, with an age standardized DALYs rate of 25.01 (95% CI 20.73, 29.33). In 2019, the number of deaths from this type of cancer attributable to smoking was 63,433.56, with an age-standardized mortality rate of 0.77 (95% CI 0.62, 0.93), and the number of DALYs was 1,656,259.98, with an age-standardized mortality rate of 19.69(95% CI 15.61, 23.93). The global number of deaths and DALYs for lip and oral cavity cancer attributable to smoking showed increasing trends year by year from 1990 to 2019, while the age-standardized mortality and DALYs rates showed decreasing trends (EAPC = –0.76 and –0.88, respectively), as shown in Table 1.
DALYs and mortality in different sex and age groups
The number of deaths and DALYs, age-standardized mortality rate, and age-standardized DALYs rate of lip and oral cavity cancer were higher in men than in women globally in 1990 and 2019 (Table 1). The age-standardized mortality rate (men EAPC = –0.80; women EAPC = –0.94) and age-standardized DALYs rate (men EAPC = –0.87; women EAPC = –1.1) decreased from 1990 to 2019 for both men and women. The age-standardized mortality and DALYs rates decreased slightly more in women than in men, as shown in Table 1 and Fig. 1.

Age-specific number (bar plot) and rate (line plot) of DALYs (A) and deaths (B) of lip and oral cavity cancer attributable to smoking in 2019 by sex. DALY, disability-adjusted life year
Overall, the number of deaths and DALYs were much higher in men than in women in all age groups, with peaks in the 60–64 age group. Meanwhile, women had the highest number of deaths in the 65–69 age group. The number of DALYs was highest in the 55–59 age group in men but in the 60–64 age group in women. Mortality rates were much higher in men than in women in all age groups, and the age-standardized mortality rates increased with increasing age in both men and women. The curve of the age-standardized DALYs rate in men was bell-shaped, i.e., it first increased and then decreased with age, peaking at 65–69, whereas the age-standardized DALYs rate in women increased slowly with age (Fig. 1).
DALYs and mortality in different countries and regions
From 1990 to 2019, the number of deaths and DALYs increased steadily in all SDI regions, with much lower number of deaths and DALYs in low-SDI regions. The age-standardized mortality and DALYs rates varied between different regions. The age-standardized mortality and DALYs rates showed overall decreasing trends in all regions except middle-SDI regions in which slight overall increasing trends were observed from 1990 to 2019 (age-standardized mortality rate, EAPC = 0.16; age-standardized DALYs rate, EAPC = 0.07). Specifically, middle-SDI regions showed an increasing trend from 1990 to 2012, and then a decreasing trend year by year. High-SDI regions showed a steady decline year by year, and the decline was largest in these regions (age-standardized mortality rate, EAPC = –1.60; age-standardized DALYs rate, EAPC = –1.74). The age-standardized mortality and DALYs rates were markedly higher in low-middle-SDI regions than in other regions in all years (Table 1, Figs. 2 and 3).

The change trends of number and age-standardized lip and oral cavity cancer DALY, and mortality rate attributable to smoking among different SDI quintiles from 1990 to 2019. (A) Number of DALYs. (B) Number of deaths. (C) Age-standardized DALY rate. (D) Age-standardized mortality rate. DALY = disability adjusted life-year

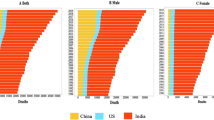
The EAPC of lip and oral cavity cancer age standardized rates attributable to smoking from 1990 to 2019 by regions. (A) The EAPC of age-standardized DALY rate. (B) The EAPC of age-standardized mortality rate. EAPC = estimated annual percentage change. DALY = disability adjusted life-year
In 2019, the three regions with the highest age-standardized mortality and DALYs rates were South Asia (1.59; 39.68), Eastern Europe (1.33; 40.59), and Central Europe (1.30; 37.67). The three regions with the lowest age-standardized mortality and DALYs rates were Central Latin America (0.23; 5.12), Western Sub-Saharan Africa (0.15; 3.85), and Andean Latin America (0.12; 2.79). From 1990 to 2019, East Asia, Oceania, and South Asia showed the greatest increase in the number of deaths and DALYs, and Australia, Eastern Europe, and high-income North America showed the smallest increase in the number of deaths and DALYs. Of the 21 geographical regions included in the analysis, East Asia (EAPC = 2.32), Oceania (EAPC = 0.07), and Eastern Europe (EAPC = 0.03) showed the greatest increase in mortality, whereas Australia (EAPC = –3.58), Central Latin America (EAPC = –2.42), and high-income North America (EAPC = –2.16) showed the largest decline in mortality. The three regions with the highest EAPC values for DALYs were East Asia (2.30), Oceania (0.03), and Eastern Europe (–0.01), and the regions with the largest decline in the number of DALYs were also the regions with the largest decline in mortality, namely Australia (EAPC = –3.52), Central Latin America (EAPC = –2.51), and high-income North America (–2.38). It is noteworthy that East Asia showed the largest increase in the mortality and DALYs rates, as shown in Table 1 and Fig. 3.
Of the 204 countries and regions analyzed, the three countries with the highest age-standardized mortality and DALYs rates were Kiribati, Pakistan, and Palau and the three countries with the lowest age-standardized mortality and DALYs rates were Nigeria, Peru, and Ghana. The three countries with the greatest increase in the number of deaths from 1990 to 2019 were the United Arab Emirates, Cabo Verde, and the Northern Mariana Islands, and the three countries with the smallest increase in the number of deaths during that period were Norway, France, and Croatia. The countries with the greatest increase in the number of DALYs were the United Arab Emirates, Cabo Verde, and Qatar, and the three countries with the smallest increase in the number of DALYs were Croatia, France, and Italy. From 1990 to 2019, the countries with the largest increase in mortality and DALYs rates were the Northern Mariana Islands (EAPC = 3.79) and Cabo Verde (EAPC = 2.84). The three countries with the greatest decrease in mortality rates were Australia (EAPC = –3.69), Colombia (EAPC = –3.54), and Canada (EAPC = –3.53). The three countries with the greatest decline in DALYs rates were Colombia (EAPC = –3.72), Canada (EAPC = –3.70), and Singapore (EAPC = –3.69), as shown in Table 1, Figs. 1 and 2.
Discussion
In this study, we comprehensively analyzed and compared the burden of lip and oral cavity cancer due to smoking by age, sex, and SDI at global, regional, and national levels during the study period. The results showed that the number of deaths and DALYs for lip and oral cavity cancer attributable to smoking increased by 69.6% and 59.2%, respectively, globally from 1990 to 2019. Meanwhile, the age-standardized mortality and DALYs rates showed decreasing trends, with EAPC values of –0.76 and –0.88, respectively. The growth in the number of deaths and DALYs due to lip and oral cavity cancer may be mainly because of global population growth and population aging.
The burden of lip and oral cavity cancer attributable to smoking was much higher in men than in women, mainly because men had higher rates of smoking and were more likely to be exposed to secondhand smoke (Safiri et al. 2022). Another study showed that there were 1.14 billion smokers globally in 2019, with a standardized smoking rate of approximately 32.7% for men aged 15 years and older, which was much higher than the rate of 6.6% for women (Shrestha et al. 2020). The burden of lip and oral cavity cancer due to smoking differed between age groups. The standardized mortality rate increased with age in both men and women, whereas the standardized DALYs rate first increased and then decreased in men, but slowly increased in women. The gradual decline in immunity, body regulation, and metabolic capacity with age and a higher incidence of underlying diseases in the elderly population may have contributed to the higher mortality rate of lip and oral cavity cancer attributable to smoking in the older population. The number of deaths in men with lip and oral cavity cancer attributable to smoking peaked in the 60–64 age group, which is consistent with the number of overall deaths attributed to smoking, which has also been shown to peak in this age group (Safiri et al. 2022). Men in the 55–69 age group had the greatest number of DALYs and deaths, and the standardized DALYs rates also peaked in this age group.
During the study period, the number of deaths and DALYs steadily escalated in all SDI regions. This may be related to the global increase in smoking, improved disease registration systems, and aging populations (Shrestha et al. 2020). Age-standardized DALYs and mortality rates generally showed decreasing trends, which may be attributable to smoking-cessation measures taken by governments and health institutions around the world in recent years. However, there was a slight upward trend in middle-SDI regions, which may be associated with the high prevalence of smoking in men in middle-SDI regions (Safiri et al. 2022). The high-SDI regions had the most decreased age-standardized mortality and DALYs rates, which may be attributable to stronger tobacco control measures and more efficient and effective tobacco use in these regions. Low-middle-SDI regions have a high prevalence of multiple diseases and the highest prevalence of tobacco use. Low-middle-SDI regions are mostly in developing countries, which have a large population base, relatively rapid population growth, and high smoking rates over the past years. The incidence and mortality rates of many cancers caused by smoking have also been reported to be relatively high. China is the largest developing country in the world. It had 2.42 million deaths attributable to smoking in 2019, which is the highest number of deaths caused by smoking for any country (Miranda-Filho and Bray 2020). The multiple reasons mentioned above have led to markedly higher age-standardized mortality and DALYs rates in low-middle-SDI regions than in other regions.
Our study found that the three regions with the highest age-standardized mortality and DALYs rates for lip and oral cavity cancer due to smoking were South Asia, Eastern Europe, and Central Europe, while the three countries with the highest rates were Kiribati, Pakistan, and Palau. The three regions with the lowest mortality and DALYs rates were Central Latin America, Western Sub-Saharan Africa, and Andean Latin America, whereas the three countries with the lowest rates were Nigeria, Peru, and Ghana. These findings are consistent with those of Saeid et al. who found that the burden of cancer attributable to smoking was lower than expected in Central Latin America, Western Sub-Saharan Africa, and Andean Latin America in 2019 (Safiri et al. 2022). The potential reason for the lower attributable burden in these regions is the lack of a well-developed cancer registry system. In addition, the smoking rates in these regions are lower than those in other regions (Siegel et al. 2019). It has been suggested that the decline in cancer burden in most countries, such as Nigeria and Ghana, is associated with their ratification of the World Health Organization Framework Convention on Tobacco Control (Sung et al. 2021). East Asia, Oceania, and Western Europe were the three regions with the most rapid increases in mortality rates, which is consistent with previous studies showing that cancer mortality attributable to smoking has increased most rapidly in these regions in the past three decades (Shrestha et al. 2020). The increases in mortality and DALYs rates are further exacerbated by increased smoking rates, population growth, and population aging in East Asia, which mostly comprises developing countries. Trends in the age-standardized mortality and DALYs rates varied among different countries, with the greatest increases seen in the Northern Mariana Islands and Carbo Verde. The highest number of deaths was seen in Carbo Verde, which is associated with the level of economic development and the quality of healthcare.
The strength relies on the first systematized utilization of GBD 2019 data and methods to estimate the global burden of disease and its trends for lip and oral cavity cancer attributable to smoking by sex, age, and SDI. Our findings offer important guidelines for the establishment of prevention and treatment plans by national and regional authorities. However, there are also certain limitations. First, the GBD 2019 database is based on epidemiological datasets to estimate disease burden, and low-SDI regions may not have robust, well-developed mortality reporting systems or cancer registration systems. Second, data on tobacco use were originated from reports, which may have led to an underrating of the number of people who smoke. In addition, GBD 2019 data only considered smoking grass products, and therefore, some tobacco-free products, chewing tobacco, and tobacco plants were not included, which may also have led to some discrepancies between the study results and the true situation. Taken together, the findings of our study need to be examined with caution.
Conclusions
Overall, the global number of deaths and DALYs from lip and oral cavity cancer attributable to smoking increased yearly from 1990 to 2019, but the age-standardized mortality and DALYs rates showed slight downward trends. The most prominent increases were seen in men and in middle-aged and older populations. Geographical differences in the trends were also noted, with Latin America and high-income North America, Australia, Colombia, and Canada showing the greatest decline, and middle-SDI regions, especially East Asia, showing a slight upward trend. Future disease control policies (e.g., tobacco control) and primitive investigating programs should concentrate on men, older populations, and certain high-risk regions, such as the Northern Mariana Islands, Carbo Verde, the United Arab Emirates, and Qatar. Various targeted health interventions should be implemented in these regions to reduce the disease burden.
Data availability
The datasets generated during and/or analyzed during the current study are available at the website of Global Health Data Exchange (GHDx) (https://ghdx. healthdata. org/gbd results tool). All data were collected from the Global Burden of Diseases database. The Global Burden of Diseases database is publicly available and considered.
References
Brathwaite R, Addo J, Smeeth L, Lock K (2015) A systematic review of tobacco smoking prevalence and description of tobacco control strategies in Sub-Saharan African countries; 2007 to 2014. PLoS One 10(7):e0132401. https://doi.org/10.1371/journal.pone.0132401
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68(6):394–424. https://doi.org/10.3322/caac.21492
Collaborators (2020) Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 396(10258):1223–1249. https://doi.org/10.1016/S0140-6736(20)30752-2
Collaborators (2021) Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990-2019: a systematic analysis from the Global Burden of Disease Study 2019. Lancet 397(10292):2337–2360. https://doi.org/10.1016/S0140-6736(21)01169-7
Gakunga R, Parkin DM (2015) Cancer registries in Africa 2014: a survey of operational features and uses in cancer control planning. Int J Cancer 137(9):2045–2052. https://doi.org/10.1002/ijc.29668
Goodchild M, Nargis N, Tursan d'Espaignet E (2018) Global economic cost of smoking-attributable diseases. Tob Control 27(1):58–64. https://doi.org/10.1136/tobaccocontrol-2016-053305
Gupta B, Bray F, Kumar N, Johnson NW (2017) Associations between oral hygiene habits, diet, tobacco and alcohol and risk of oral cancer: a case-control study from India. Cancer Epidemiol 51:7–14. https://doi.org/10.1016/j.canep.2017.09.003
Harrison JE, Weber S, Jakob R, Chute CG (2021) ICD-11: an international classification of diseases for the twenty-first century. BMC Med Inform Decis Mak 21(Suppl 6):206. https://doi.org/10.1186/s12911-021-01534-6
Hashibe M, Brennan P, Benhamou S, Castellsague X, Chen C, Curado MP, Dal Maso L, Daudt AW, Fabianova E, Fernandez L, Wünsch-Filho V, Franceschi S, Hayes RB, Herrero R, Koifman S, La Vecchia C, Lazarus P, Levi F, Mates D et al (2007) Alcohol drinking in never users of tobacco, cigarette smoking in never drinkers, and the risk of head and neck cancer: pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. J Natl Cancer Inst 99(10):777–789. https://doi.org/10.1093/jnci/djk179
Liu Z, Jiang Y, Yuan H, Fang Q, Cai N, Suo C, Jin L, Zhang T, Chen X (2019) The trends in incidence of primary liver cancer caused by specific etiologies: results from the Global Burden of Disease Study 2016 and implications for liver cancer prevention. J Hepatol 70(4):674–683. https://doi.org/10.1016/j.jhep.2018.12.001
Miranda-Filho A, Bray F (2020) Global patterns and trends in cancers of the lip, tongue and mouth. Oral Oncol 102:104551. https://doi.org/10.1016/j.oraloncology.2019.104551
Safiri S, Nejadghaderi SA, Abdollahi M, Carson-Chahhoud K, Kaufman JS, Bragazzi NL, Moradi-Lakeh M, Mansournia MA, Sullman MJM, Almasi-Hashiani A, Taghizadieh A, Collins GS, Kolahi AA (2022) Global, regional, and national burden of cancers attributable to tobacco smoking in 204 countries and territories, 1990-2019. Cancer Med 11(13):2662–2678. https://doi.org/10.1002/cam4.4647
Shrestha AD, Vedsted P, Kallestrup P, Neupane D (2020) Prevalence and incidence of oral cancer in low- and middle-income countries: a scoping review. Eur J Cancer Care (Engl) 29(2):e13207. https://doi.org/10.1111/ecc.13207
Siegel RL, Miller KD, Wagle NS, Jemal A (2019) Cancer statistics, 2019. CA Cancer J Clin 69(1):7–34. https://doi.org/10.3322/caac.21551
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F (2021) Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71(3):209–249. https://doi.org/10.3322/caac.21660
Acknowledgments
We thank all authors for their contributions to the article.
Contribution to the field statement
We first systematized utilization of GBD 2019 data and methods to estimate the global burden of disease and its trends for lip and oral cavity cancer attributable to smoking by sex, age, and SDI. There are regional and national differences, and high-risk regions and countries should implement targeted interventions to degrade the burden. Our findings offer important guidelines for the establishment of prevention and treatment plans by national and regional authorities.
Author information
Authors and Affiliations
Contributions
Yifeng Wang: Conceptualization; Lidan Zhuo: Methodology; Saiyan Yang: Data curation; Cheng Dong: Writing - Original draft preparation; Xuzhi Hu: Visualization, Formal analysis; Yifeng Wang: Writing - Reviewing and Editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
This study was performed in line with the principles of the Declaration of Helsinki. The study was approved by Beilun District People’s Hospital.
Conflicts of interest
The authors declare they have no financial interests.
Ethics approval
The survey including human participants was approved and evaluated by the Medical Ethics Committee of Beilun District People’s Hospital.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOC 1902 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wang, Y., Zhuo, L., Yang, S. et al. The worldwide epidemiology of lip and oral cavity cancer attributable to smoking based on the Global Burden of Disease Study 2019. J Public Health (Berl.) (2023). https://doi.org/10.1007/s10389-023-02081-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10389-023-02081-2