
Abstract
Background
The Middle East and North Africa (MENA) region continues to have the lowest prevalence of HIV (human immunodeficiency virus) in the world, less than 0.1%, yet new transmissions are increasing. Consistent condom use can reduce the probability of transmission by 90–95%, and its use remains as the staple prevention method; however, this isn’t the case for the MENA region, where condom use, knowledge of proper use, and accessibility are limited.
Aims
To conduct a systematic review on condom use, its use across different population groups, and its barriers and facilitators in countries that fall under the UNAIDS regional classification of MENA.
Methods
This systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines. The search included electronic databases: PubMed/MEDLINE, Academic Search Ultimate, COCHRANE, APA PsycINFO, ScienceDirect, CINAHL Complete, Scopus. There was no date restriction.
Results
Of the 471 records retrieved, 45 articles were appraised and included in the analysis. The reported barriers and facilitators are sub-divided into personal, social, and structural factors. Condom accessibility, partner objection, and their perceived ineffectiveness were key barriers, whereas availability, cost, and lack of awareness were rarely mentioned. Concerns of personal health and future financial security, as well as positive peer influence and delayed sexual experience, were identified as motivators.
Conclusion
Condom promotion in the region needs to incorporate gender-based power in relationships and the influence of religion, as well as the legal and structural factors. More investment and research are needed for women-initiated contraceptive and digital healthcare initiatives.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Sexually transmitted infections (STIs) are one of the heaviest burdens on public health systems in low and high-income countries. The MENA (Middle East and North Africa) region continues to have a low prevalence of HIV, less than 0.1% yet, the number of new transmissions has increased by 33% from 2010 to 2021. It unfortunately also has the lowest HIV treatment coverage in the world (50% of PLHIV in 2021) and the lowest proportion of PLHIV who are virally suppressed (44% in 2021) (UNAIDS 2022).
Research has shown that correct and consistent condom use is an effective form of STI prevention, reducing the probability of transmission by 90–95% ( Pinkerton and Abramson 1997). Increasing condom use remains as a key public health prevention method, since condoms have no major medical side-effects, are relatively easy to obtain and carry, and are cost-effective (Evans et al. 2020 ).
However, gaps and inequities in condom access, knowledge, and use are still prevalent in MENA. In Libya, for example, 40% (of 227) of men who have sex with men (MSM) (Valadez et al. 2013) have had unprotected sex with both men and women, and only 20%–54% of people who inject drugs in the region have ever used condoms (Mumtaz et al. 2014).
This present study is, to our knowledge, the first systematic review to capture and examine the condom-use landscape in MENA, presenting an overview of condom use across all groups, the reasons for condom use/non-use, as well as the barriers that interfere and facilitators that encourage condom use.
The current systematic review on the MENA region has two overarching aims:
-
a)
review the state of evidence for condom use, and;
-
b)
analyse individual, interpersonal and structural-level barriers/facilitators to condom use.
Search strategy
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines. The search was limited to the 19 countries included in the UNAIDS classification of MENA: Algeria, Bahrain, Djibouti, Egypt, Iraq, Jordan, Kuwait, Lebanon, Libya, Morocco, Oman, Qatar, Saudi Arabia, Somalia, Sudan, Syria, Tunisia, United Arab Emirates (UAE), and Yemen. At the start of this review, Iran was still included in MENA before its transfer to the Asia and the Pacific Region as reported in the UNAIDS Global report 2022 (UNAIDS 2022). As a result, it was decided to remove the studies from Iran during the study assessment stage.
The following electronic databases were searched: PubMed/MEDLINE, Academic Search Ultimate, COCHRANE, APA PsycINFO, ScienceDirect, CINAHL Complete, and Scopus.
The search strategy included terms specific to condom use, access and barriers, using free-text terms and medical subject headings (MeSH) terms that included ‘condom’, ‘barriers’, ‘Middle-East’, ‘North Africa’ and each of the countries. Reference lists of the reviewed articles were hand-searched. Studies were limited to English language and there were no date restrictions.
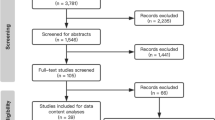
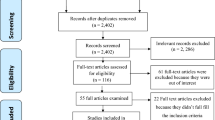
The number of records retrieved was 471, and 215 titles and abstracts were screened. To be included in this review, papers needed to meet the following criteria: (1) be research studies, (2) have abstracts which mentioned condom use, (3) be studies that sampled men and women regardless of their sexual orientation and marital status, and (4) relate to MENA countries. A total of 203 papers were examined in full-text for eligibility, and 90 articles were appraised. As a result of Iran’s exclusion, 45 papers were excluded, and 45 papers were included in the review.
All articles retrieved from initial searches were imported into Endnote and duplicates removed. AH screened titles and abstracts against the eligibility criteria for inclusion. PR and EvT independently screened a random selection of 20% of all abstracts for consistency. Any disagreements were resolved with a discussion within the team.
The process was recorded on a Microsoft Excel spreadsheet, and the risk of bias/quality of the studies was assessed individually. Quality was assessed using the appropriate checklist from CASP and the Mixed Methods Appraisal Tool (MMAT) for mixed-methods studies. No study was found to have a high risk of bias, although religious and cultural restrictions resulted in certain groups and questions, i.e., single women and anal sex, being omitted.
Data extraction and analysis
A standardised data extraction form was developed in Excel. AH extracted data from the final 45 included articles, which was checked by PR and EvT. The quantitative and qualitative findings were analysed separately. Thematic analysis was used for the qualitative data (Fig. 1).

PRISMA flow chart
Findings
A summary of the findings for each sample group for the different study types is presented in Tables 1, 2, and 3 (placed in Appendix below due to its size, which would interrupt the main narrative). A synthesis of all barriers and facilitators is presented in a conceptual model (Fig. 2). The 45 studies included: 37 quantitative, six qualitative, and two mixed-methods studies; 14 were from Lebanon, seven Egypt, seven Sudan, six Jordan, four Saudi Arabia, two Morocco, two Yemen, one each from Iraq, Somalia, and UAE.

Model of barriers and facilitators of condom use in MENA region
One study on drug-users, five on female sex workers (FSWs), nine on MSMs, eight on men, six on women, eight on general population, five on youths, two on prisoners, two on refugees, one on male sex workers, and one on PLHIV.
Quantitative results
Thirty-seven quantitative studies: 1996 to 2021, 11 Lebanon (Adib et al. 2002; Barbour and Salameh 2009; Kahhaleh et al. 2009; Mahfoud et al. 2010; Wagner et al. 2014; Salameh et al. 2016; Tohme et al. 2016; Heimer et al. 2017; Assi et al. 2019; Storholm et al. 2021; Zaki et al. 2021), seven Egypt (Kabbash et al. 2007; El-Sayyed et al. 2008; Nada and Suliman 2010; Soliman et al. 2010; Wahdan et al. 2013; Saleh et al. 2014; Farghaly et al. 2020), five Sudan (Ibnouf et al. 2007; Abdelrahim 2010; Zeidan et al. 2011; Mohamed and Mahfouz 2013; Mohamed 2014), four Saudi Arabia (Fageeh 2014; Wafa et al. 2014; Alhusain et al. 2018; Aladham et al. 2020), four Jordan (Alkaiyat et al. 2014; Al Rifai et al. 2015; Al-Maharma et al. 2019; Alyahya et al. 2019), two in Morocco (Laraqui et al. 2017; Bozicevic et al. 2018), and one each in Iraq (Ismael and Sabir Zangana 2012), Yemen (Mirzazadeh et al. 2014), Somalia (Kriitmaa et al. 2010) and UAE (Ghazal-Aswad et al. 2002).
Qualitative and mixed-methods results
Six qualitative studies: 2002 to 2020, two each in Lebanon (Wagner et al. 2012; Aunon et al. 2015), Sudan (Elshiekh et al. 2020; Elshiekh et al. 2021) and Jordan (Petro-Nustas and Al-Qutob 2002; Khalaf et al. 2008). Two mixed-method studies from 2004 and 2006 from Lebanon and Yemen (Kulczycki 2004; Busulwa et al. 2006).
Themes
Personal
In a region shaped by a patriarchal society whereby males dominate in decision-making (Petro-Nustas and Al-Qutob 2002; Khalaf et al. 2008), reduced male personal pleasure and societal masculine beliefs were barriers to condom use:
“It is not the wife’s right to force any authority — in decision making — over her husband, this is not allowed by any social norm or endorsed by any law in any society in the world” (Petro-Nustas and Al-Qutob 2002)
The most stated reasons given for not using condoms by men were ‘I don’t like condoms’ and ‘reduced sexual pleasure’ (Adib et al. 2002; Petro-Nustas and Al-Qutob 2002; Kulczycki 2004; Busulwa et al. 2006; Kabbash et al. 2007; Ismael and Sabir Zangana 2012; Alkaiyat et al. 2014; Mirzazadeh et al. 2014; Mohamed 2014; Aunon et al. 2015; Laraqui et al. 2017). Some men voiced feelings of embarrassment and contempt toward the idea of using or even buying a contraceptive method (Petro-Nustas and Al-Qutob 2002; Kabbash et al. 2007; Alkaiyat et al. 2014; Mirzazadeh et al. 2014; Mohamed 2014).
This resistance is undoubtedly a result of condom efficacy (Kulczycki 2004; Busulwa et al. 2006; Alkaiyat et al. 2014; Mohamed 2014; Al Rifai et al. 2015; Elshiekh et al. 2020), harmful effects (Ghazal-Aswad et al. 2002; Kabbash et al. 2007; Elshiekh et al. 2020), lack of knowledge of proper use (Busulwa et al. 2006; Kabbash et al. 2007; Assi et al. 2019; Elshiekh et al. 2020; Zaki et al. 2021), and fear that suggesting to use a condom may lead the female partner to suspect that they may have been unfaithful (Petro-Nustas and Al-Qutob 2002; Kulczycki 2004) or are having sex with men (Wagner et al. 2012; Wagner et al. 2014). Partner objection was the main reason given for non-condom use for women, demonstrating that women often dismiss their sexual and health needs in order to keep their partners sexually content and stay in the relationship (Kulczycki 2004; Khalaf et al. 2008; Abdelrahim 2010; Kriitmaa et al. 2010; Zeidan et al. 2011; Al-Maharma et al. 2019; Zaki et al. 2021).
Notions of fear, violence, abandonment, and stigmatisation (Kulczycki 2004; Busulwa et al. 2006; Elshiekh et al. 2020; Zaki et al. 2021) among women is emulated throughout the studies, whether it is requesting condom use or purchasing condoms. Fear was also found to be a conduit of condom use regardless of the gender; fear of transmission (Wagner et al. 2012; Wahdan et al. 2013; Elshiekh et al. 2020), and the social and legal repercussions of pregnancy outside of marriage (Wagner et al. 2012; Elshiekh et al. 2020).
One of the main obstacles to condom use by sex workers was the financial implication, losing the client, or being paid more for condomless sex (Zeidan et al. 2011; Aunon et al. 2015). When a condom was used by a FSW, it was often suggested by the client (Kriitmaa et al. 2010; Mahfoud et al. 2010). This supports the findings that men use condoms more when having extramarital sexual relations due to the misconception that the probability of acquiring HIV is greater (Petro-Nustas and Al-Qutob 2002; Kulczycki 2004).
It is apparent that the concept of self-esteem is significant in the increase of condom use, and transpires when an individual places importance on their health (Kulczycki 2004; Busulwa et al. 2006; Wagner et al. 2012; Aunon et al. 2015; Elshiekh et al. 2020) as well as their financial future. Early sexual debut plays a major role in inconsistent condom use (Kahhaleh et al. 2009; Abdelrahim 2010; Nada and Suliman 2010; Al Rifai et al. 2015), which could be due to the confidence to negotiate safe sex or the knowledge of STI preventative methods not having been acquired yet.
Six studies indicated the co-occurrence of low condom use with other high-risk behaviours such as substance use (Assi et al. 2019; Farghaly et al. 2020; Zaki et al. 2021) and alcohol use (Mohamed 2014; Al Rifai et al. 2015; Laraqui et al. 2017; Assi et al. 2019; Farghaly et al. 2020; Zaki et al. 2021).
Four found that the educational level of participants (Ismael and Sabir Zangana 2012; Alkaiyat et al. 2014; Mohamed 2014; Farghaly et al. 2020) as well as their sexual partners (Ismael and Sabir Zangana 2012) had a positive effect on condom use.
Low risk perception was present in all groups studied. Responses that included ‘Condom was not necessary’ (Kabbash et al. 2007; Kriitmaa et al. 2010; Mirzazadeh et al. 2014; Laraqui et al. 2017; Abdelrahim 2010) and ‘I didn’t think of it’ (Abdelrahim 2010; Mirzazadeh et al. 2014; Laraqui et al. 2017) were supported by appearance-based judgements (Aunon et al. 2015) and claims of HIV being a ‘gay thing’ (Wagner et al. 2012).
Being in a long-term partnership or a marriage promotes a sense of trust and confidence that the partner is monogamous and there is no risk of STI transmission, therefore it is concluded that condoms are not needed (Adib et al. 2002; Petro-Nustas and Al-Qutob 2002; Wagner et al. 2012; Alkaiyat et al. 2014; Mirzazadeh et al. 2014; Wagner et al. 2014; Laraqui et al. 2017; Assi et al. 2019; Zaki et al. 2021) and their use can be seen as a sign of distrust and ‘anti-love’ (Aunon et al. 2015; Elshiekh et al. 2020). If condoms are used, it would be for contraception (Busulwa et al. 2006; Ismael and Sabir Zangana 2012; Mohamed and Mahfouz 2013; Wafa et al. 2014; Alhusain et al. 2018), although they are not the preferred method (Kulczycki 2004; Abdelrahim 2010; Aladham et al. 2020).
Social
Women are culturally required to be sexually inexperienced or passive (Kulczycki 2004; Elshiekh et al. 2020) and to dismiss their own sexual pleasure and health (Petro-Nustas and Al-Qutob 2002).
Misconceptions (Busulwa et al. 2006; Kabbash et al. 2007; Khalaf et al. 2008; Ismael and Sabir Zangana 2012; Mohamed and Mahfouz 2013; Wagner et al. 2014; Al Rifai et al. 2015; Aunon et al. 2015; Laraqui et al. 2017; Elshiekh et al. 2020; Elshiekh et al. 2021), hearsay (Kulczycki 2004) and gossip are significant obstacles in condom promotion and acceptance.
Those who perceived their peers and network as having positive attitudes towards safe sex and condom use reported more condom use (Elshiekh et al. 2020; Elshiekh et al. 2021) than those who didn’t.
Condom use is regularly associated with illicit (extramarital and premarital) sex (Petro-Nustas and Al-Qutob 2002; Kulczycki 2004; Busulwa et al. 2006; Elshiekh et al. 2021) which in turn, increases the socio-cultural stigma of purchasing and using condoms (Alkaiyat et al. 2014; Mirzazadeh et al. 2014; Mohamed 2014).
A study of university students in Lebanon found that condom use is higher in more liberal climates that allow open discussion (Salameh et al. 2016). This is particularly relevant to young people, as many are practising premarital sex without proper understanding of STI transmission and prevention (Kriitmaa et al. 2010; Elshiekh et al. 2021). Two studies highlighted that heterosexual sexually active people(Wagner et al. 2012; Elshiekh et al. 2020) are more concerned about pregnancy than HIV/STIs:
“In Beirut, most girls require the use of condoms because they are scared of getting pregnant, and they are scared of scandal.” (Wagner et al. 2012)
The stigmatisation of women’s sexuality increases their vulnerability to STIs as it prevents them from being prepared by carrying condoms (Zaki et al. 2021) and/or relying on their partner to have one with them (Kriitmaa et al. 2010; Mahfoud et al. 2010; Elshiekh et al. 2021).
The opposition to condom promotion by healthcare providers stems from socio-religious beliefs that condom promotion encourages illegal sex (Busulwa et al. 2006; Elshiekh et al. 2020; Elshiekh et al. 2021) and that natural family planning methods are better (Khalaf et al. 2008).
The stigma associated with premarital sex is linked with the importance of the woman’s virginity (Elshiekh et al. 2020), ensuring that the hymen remains intact and avoiding pregnancy. This fear of social disgrace encourages non-vaginal sex which is mostly unprotected, as there is a misconception that HIV transmission is more likely through vaginal sexual contact than through anal or oral (Abdelrahim 2010; Wagner et al. 2014). The prevalence of heterosexual anal sex is undetermined; however, it does occur among young adults (Zaki et al. 2021).
There is a myriad of problems associated with another under-researched topic: unendorsed marriages. Zawaj mut‘ah or informal marriages (Saleh et al. 2014) are controversial in the region, as they are not religiously sanctioned in most countries. These marriages allow men to marry a woman, often privately and verbally, sometimes for a pre-determined period of time and a specific price, have sexual relations, and divorce without consequences. As they are socially invisible, it is perceived that women in particular lack any health protection.
Structural
The query into condom availability is unclear. In some studies, it relates to the ability to purchase condoms, in others it is implied as being to do with accessibility. Inaccessibility is defined as ‘not available’ (Adib et al. 2002; Abdelrahim 2010; Wahdan et al. 2013; Mirzazadeh et al. 2014; Laraqui et al. 2017; Assi et al. 2019) or ‘obtaining/ purchasing condoms’ in one study (Alkaiyat et al. 2014), and it was a suggestion of ‘unplanned sexual encounter/heat of the moment’ in other studies (Adib et al. 2002; Kriitmaa et al. 2010; Elshiekh et al. 2021).
Condoms are readily available in the region (Abdelrahim 2010; Ismael and Sabir Zangana 2012; Wahdan et al. 2013) as an accepted form of contraception and are usually purchased in pharmacies (Laraqui et al. 2017; Soliman et al. 2010). Nonetheless, there are barriers, as some countries require verification of marriage (Busulwa et al. 2006), there is a lack of privacy at point of sale (Kabbash et al. 2007; Mohamed and Mahfouz 2013), and sometimes the cost of condoms is an issue (Busulwa et al. 2006; Mohamed and Mahfouz 2013; Alkaiyat et al. 2014; Laraqui et al. 2017).
Refugees, MSM, drug users, and sex workers have limited access to health services (Kriitmaa et al. 2010; Mahfoud et al. 2010; Alkaiyat et al. 2014; Al-Maharma et al. 2019; Storholm et al. 2021), have language barriers (Mahfoud et al. 2010; Wafa et al. 2014), and are subjected to status or legal discrimination (Kriitmaa et al. 2010; Zeidan et al. 2011; Aunon et al. 2015; Tohme et al. 2016; Farghaly et al. 2020).
Financial needs and the lack of self-esteem (Farghaly et al. 2020) are also motivators for accepting condomless sex for more money (Zeidan et al. 2011; Aunon et al. 2015). Condom use has also been significantly associated with participants who are more financially stable and had a place to live (Ismael and Sabir Zangana 2012; Aunon et al. 2015) .
Sexual health education is limited in schools across the region ,and many of the sexually active participants only gain knowledge about condom use several years after practising sex. Some wouldn’t have seen a condom before (Elshiekh et al. 2020; Elshiekh et al. 2021).
“The first time I heard about the condom was 3 years ago. I started practising sex many years before that, but I did not have enough knowledge about using condoms” (Elshiekh et al. 2020).
Eight studies concluded that training on proper condom use was necessary (Busulwa et al. 2006; Kabbash et al. 2007; Ismael and Sabir Zangana 2012; Wahdan et al. 2013; Mohamed 2014; Assi et al. 2019), and that those who attend are more likely to know how to use condoms and use them consistently (Wahdan et al. 2013; Elshiekh et al. 2020).
The Internet has opened new avenues for people to access sexual health information, providing enough privacy and freedom to research (Saleh et al. 2014; Elshiekh et al. 2021) and discuss issues otherwise considered a taboo in the region. Not only is access to Internet associated with increased condom use but the relative anonymity makes it easier to initiate the discussion of HIV status and condom use (Wagner et al. 2012). This also means that people in the region have access to online pornography which influence sexual behaviours (Assi et al. 2019; Elshiekh et al. 2021; Zaki et al. 2021).
One study found a significant association between condom use and HIV testing (Zeidan et al. 2011). HIV testing can also be a reason to discontinue condom use; in this context, it is a milestone in the relationship and one that signifies commitment and trust.
“My boyfriend and I got tested together, because if it is serious and we want to have sex without a condom obviously we have to get tested.” (Wagner et al. 2012)
Discussion
This systematic review has accentuated often hidden personal, social, and structural barriers that affect STI/HIV transmissions as well as identified potential facilitators for effective interventions.
It is essential that the promotion of condoms reinforces positive messages that condoms promote personal health and future financial security rather than using fear as a motivator. To address the concept of masculine superiority, the interventions should appeal to the existing values. Men should be encouraged to consider consistent condom use is a healthy attribute of masculinity, namely taking care of their own and their partner’s health and quality of life.
Women need to be empowered to consider their own health by providing them with a viable tool for HIV prevention that they can initiate and control. Female condoms enable women to take the initiative in protecting their own reproductive health as well as countering the barriers and misconceptions men have against using male condoms.
The influence of religion in the region (Ghazal-Aswad et al. 2002; Petro-Nustas and Al-Qutob 2002; Kulczycki 2004; Busulwa et al. 2006; Ibnouf et al. 2007; El-Sayyed et al. 2008; Khalaf et al. 2008; Barbour and Salameh 2009; Zeidan et al. 2011; Ismael and Sabir Zangana 2012; Wagner et al. 2012; Wahdan et al. 2013; Alkaiyat et al. 2014; Fageeh 2014; Mirzazadeh et al. 2014; Mohamed 2014; Wafa et al. 2014; Al Rifai et al. 2015; Aunon et al. 2015; Alhusain et al. 2018; Al-Maharma et al. 2019; Aladham et al. 2020; Elshiekh et al. 2020; Elshiekh et al. 2021; Zaki et al. 2021) is strong, and interventions should be developed within these frameworks. Leverage on religious teachings to promote the use of condoms as a means of safeguarding of one’s health and that of others is necessary.
To counter the negative effects of misinformation, open discussions of sexual health and the socio-cultural stigma to purchasing and using condoms need to be addressed. This should begin with the healthcare professionals, as they are critical in raising awareness and confidence in condom use and its efficacy.
The Internet is a powerful platform whereby people can access explicit information on safe sex privately, avoiding any social or legal repercussions. Digital healthcare initiatives can decrease the burden on the health systems, and reduce the stigma/embarrassment associated with condom training as well as correcting any misconceptions.
A key limitation of this review is the exclusion of potential studies that are in French, as it is the main European language in several countries in MENA. As with any systematic review, some studies may have been missed due to the concise search terms or as a result of publication bias and thus excluded from this review. It does need to be acknowledged that as all the included studies are primary research papers, they carry their own risks of bias such as selection bias, due to the nature of the research and geographical locations.
Conclusion
This review found that condom use among different groups of population is generally low and is associated with the governing policies, structure, beliefs, practices, and norms of not only of the region but the community they belong to. Recognising both the barriers and facilitators may help health promotors across the MENA region to improve their targeted condom-use messages to the appropriate populations.
Availability of data and material
These are available as they are published papers.
References
Abdelrahim MS (2010) HIV prevalence and risk behaviors of female sex workers in Khartoum, north Sudan. AIDS 24(Suppl 2):S55–S60
Adib SM, Akoum S, El-Assaad S, Jurjus A (2002) Heterosexual awareness and practices among Lebanese male conscripts. Eastern Mediterranean Health J 8(6):765–775
Al Rifai R, Nakamura K, Seino K, Kizuki M, Morita A (2015) Unsafe sexual behaviour in domestic and foreign migrant male workers in multinational workplaces in Jordan: occupational-based and behavioural assessment survey. BMJ Open 5(6):e007703
Aladham M, Turkistany H, Masud N, Alaqeel F, Alharbi R, Aljbli L, Alharisi A, Alotaibie M, Almotairi A, Alassaf A (2020) Differences in knowledge about contraception among Saudi males and females at tertiary hospitals in Riyadh. J Family Med Primary Care 9(12):6254–6260
Alhusain F, Alkaabba F, Alhassan N, Alotaibi S, Breakeit S, Musaudi E, Alhasan A (2018) Patterns and knowledge of contraceptive methods use among women living in Jeddah, Saudi Arabia. Saudi J Health Sci 7(2):121–126
Alkaiyat A, Schaetti C, Liswi M, Weiss MG (2014) Condom use and HIV testing among men who have sex with men in Jordan. J Int AIDS Soc 17:1–8
Al-Maharma D, Safadi R, Ahmad M, Halasa S, Nabolsi M, Dohrn J (2019) Knowledge, attitudes and practices of Syrian refugee mothers towards sexually transmitted infections. Int J Women's Health 11:607–615
Alyahya MS, Hijazi HH, Alshraideh HA et al (2019) Do modern family planning methods impact women’s quality of life? Jordanian women’s perspective. Health Qual Life Outcomes 17:154
Assi A, Abu Zaki S, Ghosn J, Kinge N, Naous J, Ghanem A, Abou Abbas D, Bakouny Z, Azzi G, Tomb R (2019) Prevalence of HIV and other sexually transmitted infections and their association with sexual practices and substance use among 2238 MSM in Lebanon. Scientific Rep 9(1):15142
Aunon FM, Wagner GJ, Maher R, Khouri D, Kaplan RL, Mokhbat J (2015) An exploratory study of HIV risk behaviors and testing among male sex workers in Beirut, Lebanon. Social Work Public Health 30(4):373–384
Barbour B, Salameh P (2009) Knowledge and practice of university students in Lebanon regarding contraception. East Mediterr Health J 15(2):387–399
Bozicevic I, Guezzar F, Stulhofer A, Bennani A, Handanagic S, Barbaric J, El Rhilani H, Alami K, Khattabi H, Riedner G, Maaroufi A (2018) HIV prevalence and related risk behaviours in female seasonal farm workers in Souss Massa Draa, Morocco: results from a cross-sectional survey using cluster-based sampling. Sex Transm Infect 94(7):515–517
Busulwa R, Takiyaddin M Y, Azzubeidi A A, El Zein El Mousaad H, Tawillah J and Ziady H, (2006). Perceptions of the condom as a method of HIV prevention in Yemen. East Mediterr Health J, 12 Suppl 2, S64-S77.
El-Sayyed N, Kabbash IA, El-Gueniedy M (2008) Knowledge, attitude and practices of Egyptian industrial and tourist workers towards HIV/AIDS. East Mediterr Health J 14(5):1126–1135
Elshiekh HF, Hoving C, de Vries H (2020) Exploring determinants of condom use among university students in Sudan. Arch Sex Behavior 49(4):1379–1391
Elshiekh HF, de Vries H, Hoving C (2021) Assessing sexual practices and beliefs among university students in Khartoum, Sudan; a qualitative study. Sahara J 18(1):170–182
Evans WDA, Hatheway M, Deperthes B (2020) Systematic review of peer-reviewed literature on global condom promotion programs. Int J Environ Res Public Health 17(7):2262
Fageeh WMK (2014) Sexual behavior and knowledge of human immunodeficiency virus/aids and sexually transmitted infections among women inmates of Briman Prison, Jeddah, Saudi Arabia. BMC Infect Dis 14(1):1–12
Farghaly AG, Alkassabany YM, El-Ghitany EM (2020) HBV, HCV and HIV among female sex workers; is it a health problem? Sex Relationship Ther 35(4):462–477
Ghazal-Aswad S, Zaib-Un-Nisa S, Rizk DEE, Badrinath P, Shaheen H, Osman N (2002) A study on the knowledge and practice of contraception among men in the United Arab Emirates. J Family Plann Reprod Health Care 28(4):196–200
Heimer R, Barbour R, Khouri D, Crawford FW, Shebl F, Aaraj E, Khoshnood K (2017) HIV risk, prevalence, and access to care among men who have sex with men in Lebanon. AIDS Res Hum Retrovir 33(11):1149–1154
Ibnouf AH, van den Borne HW, Maarse JAM (2007) Utilization of family planning services by married Sudanese women of reproductive age. East Mediterr Health J 13(6):1372–1381
Ismael AS, Sabir Zangana JM (2012) Knowledge, attitudes and practice of condom use among males aged (15–49) years in Erbil Governorate. Global J Health Sci 4(4):27–36
Kabbash IA, El-Sayed NM, Al-Nawawy AN, Shady IK, Zeid MSA (2007) Condom use among males (15-49 years) in lower Egypt: knowledge, attitudes and patterns of use. East Mediterr Health J 13(6):1405–1416
Kahhaleh JG, El Nakib M, Jurjus AR (2009) Knowledge, attitudes, beliefs and practices in Lebanon concerning HIV/AIDS, 1996–2004. East Mediterr Health J 15(4):920–933
Khalaf I, Abu-Moghli F, Callister L, Rasheed R (2008) Jordanian women's experiences with the use of traditional family planning. Health Care Women Int 29(5):527–538
Kriitmaa K, Testa A, Osman M, Bozicevic I, Riedner G, Malungu J, Irving G, Abdalla I (2010) HIV prevalence and characteristics of sex work among female sex workers in Hargeisa, Somaliland, Somalia. AIDS 24(Suppl 2):S61–S67
Kulczycki A (2004) The sociocultural context of condom use within marriage in rural Lebanon. Stud Family Plann 35(4):246–260
Laraqui S, Laraqui O, Manar N, Ghailan T, Belabsir M, Deschamps F, Laraqui CH (2017) The assessment of seafarers' knowledge, attitudes and practices related to STI/HIV/AIDS in northern Morocco. Int Maritime Health 68(1):26–30
Mahfoud Z, Afifi R, Ramia S, El Khoury D, Kassak K, El Barbir F, Ghanem M, El-Nakib M, DeJong J (2010) HIV/AIDS among female sex workers, injecting drug users and men who have sex with men in Lebanon: results of the first biobehavioral surveys. AIDS 24(Suppl 2):S45–S54
Mirzazadeh A, Emmanuel F, Gharamah F, Al-Suhaibi AH, Setayesh H, McFarland W, Haghdoost AA (2014) HIV prevalence and related risk behaviors in men who have sex with men, Yemen 2011. AIDS Behavior 18(Suppl 1):S11–S18
Mohamed BA (2014) Correlates of condom use among males in North Sudan. Sex Health 11(1):31–36
Mohamed BA, Mahfouz MS (2013) Factors associated with HIV/AIDS in Sudan. BioMed Res Int 2013:1–6
Mumtaz GR, Weiss HA, Thomas SL, Riome S, Setayesh H, Riedner G, Semini I, Tawil O, Akala FA, Wilson D, Abu-Raddad LJ (2014) HIV among people who inject drugs in the Middle East and North Africa: systematic review and data synthesis. PLoS Med 11(6):e1001663
Nada KH, Suliman EDA (2010) Violence, abuse, alcohol and drug use, and sexual behaviors in street children of Greater Cairo and Alexandria, Egypt. AIDS 24(Suppl 2):S39–S44
Petro-Nustas W, Al-Qutob R (2002) Jordanian men's attitudes and views of birth-spacing and contraceptive use (a qualitative approach). Health Care Women Int 23(6/7):516–529
Pinkerton SD, Abramson PR (1997) Effectiveness of condoms in preventing HIV transmission. Social Sci Med 44(9):1303–1312
Salameh P, Zeenny R, Salame J, Waked M, Barbour B, Zeidan N, Baldi I, Salame J (2016) Attitudes towards and practice of sexuality among university students in Lebanon. J Biosocial Sci 48(2):233–248
Saleh WF, Gamaleldin SF, Abdelmoty HI, Raslan AN, Fouda UM, Mohesen MN, Youssef MAFM (2014) Reproductive health and HIV awareness among newly married Egyptian couples without formal education. Int J Gynecol Obstet 126(3):209–212
Soliman C, Rahman IA, Shawky S, Bahaa T, Elkamhawi S, El Sattar AA, Oraby D, Khaled D, Feyisetan B, Salah E, El Taher Z, El Sayed N (2010) HIV prevalence and risk behaviors of male injection drug users in Cairo, Egypt. AIDS 24(Suppl 2):S33–S38
Storholm ED, Mutchler MG, Ghosh-Dastidar B, Balan E, Mokhbat J, Kegeles SM, Wagner GJ (2021) Gearing up for PrEP in the Middle East and North Africa: an initial look at willingness to take PrEP among young men who have sex with men in Beirut, Lebanon. Behavior Med 47(2):111–119
Tohme J, Egan JE, Friedman MR, Stall R (2016) Psycho-social correlates of condom use and HIV Testing among MSM refugees in Beirut, Lebanon. AIDS Behavior 20(Suppl 3):417–425
UNAIDS (2022) IN DANGER: UNAIDS Global AIDS Update 2022. Joint United Nations Programme on HIV/AIDS, Geneva
Valadez JJ, Berendes S, Jeffery C, Thomson J, Ben Othman H, Danon L, Turki AA, Saffialden R and Mirzoyan L (2013) Filling the knowledge gap: measuring HIV prevalence and risk factors among men who have sex with men and female sex workers in Tripoli, Libya. PLoS One 8(6):e66701
Wafa F, Sami B, Hanin Al T, Muhammad Y, Esam A, Suha F, Mona A, Moneerah A, Soonham Y, Taha K (2014) Chlamydia trachomatis infection among female inmates at Briman prison in Saudi Arabia. BMC Public Health 14(1):267–272
Wagner G, Aunon FM, Kaplan RL, Rana Y, Khouri D, Tohme J, Mokhbat J, Graham SM (2012) A qualitative exploration of sexual risk and HIV testing behaviors among men who have sex with men in Beirut, Lebanon. PLoS ONE 7(9):1–7
Wagner G, Tohme J, Hoover M, Frost S, Ober A, Khouri D, Iguchi M, Mokhbat J (2014) HIV prevalence and demographic determinants of unprotected anal sex and HIV testing among men who have sex with men in Beirut, Lebanon. Arch Sex Behavior 43(4):779–788
Wahdan I, Wahdan A, El Gueneidy M, El Rahman IA (2013) Prevalence and determinants of condom utilization among people living with HIV/AIDS in Egypt. East Mediterr Health J 19(12):967–974
Zaki SA, Naous J, Ghanem A, Abou Abbas D, Tomb R, Ghosn J, Assi A (2021) Prevalence of STIs, sexual practices and substance use among 2083 sexually active unmarried women in Lebanon. Scientific Reports 11(1):1–11
Zeidan ZA, Abdu MZ, Gadour MO, Bhairy NM (2011) Condom use among illegal multi-partners females in the Sudan. Sudan J Med Sci 6(3):195–198
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Abier Hamidi. Dr Pramod Regmi and Prof. Dr Edwin van Teijlingen independently screened a random selection of 20% of all abstracts for consistency.
The first draft of the manuscript was written by Abier Hamidi, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval
Not required for this review.
Consent to participate
Not required as these are already published papers
Consent for publication
Not required as these are already published papers
Competing interest
The authors have no competing interests to declare that are relevant to the content of this article.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hamidi, A., Regmi, P. & van Teijlingen, E. Facilitators and barriers to condom use in Middle East and North Africa: a systematic review. J Public Health (Berl.) (2023). https://doi.org/10.1007/s10389-023-01923-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10389-023-01923-3