
Abstract
Background
In 2020, COVID-19 spread rapidly in Iran and other parts of the world. Some of the epidemiological aspects of this disease remain unknown; therefore, the present study was designed with the aim of determining the trend of incidence and mortality of COVID-19 from February 2020 to July 2021 in southern Iran.
Methods
The present study was a cross-sectional analytical study that included all people who had COVID-19 in the period from February 2020 to July 2021 and whose information had been registered in the Infectious Diseases Center of Larestan city and MCMC unit. The study area included the cities of Larestan, Evaz, and Khonj, located in the south of Fars province in southern Iran.
Results
Since the emergence of COVID-19 until July 2021, a total of 23,246 new cases of infection were reported in the southern region of Fars province. The average age of patients was 39.90±18.30 years and the range of ages varied from 1 to 103 years. The results of the Cochran–Armitage trend test showed that the trend of the disease in 2020 was completely upward. The first positive case of COVID-19 was recorded on February 27, 2020. The incidence curve in 2021 is sinusoidal, but in general, the results of the Cochran–Armitage trend test showed that the incidence of the disease increased significantly (P-trend < 0.001). Most cases were reported in July, April, and the end of March.
Conclusion
In general, the incidence rate of COVID-19 has varied sinusoidally from 2020 to mid-2021. Although the incidence of the disease increased, the number of deaths has fallen. It seems that the increase in the number of diagnostic tests and the implementation of the national COVID-19 immunization program have been effective in changing the trend of the disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In December 2019, several cases of pneumonia of unknown etiology were seen in Wuhan, Hubei Province, China, which were later identified as being caused by a beta-coronavirus (Delam et al. 2022; Xie and Chen 2020). These patients had an epidemiological link to an extensive seafood market (Rothan and Byrareddy 2020). This virus is a common human–animal coronavirus that is highly genetically similar (96.3%) to the RaTG13 bat coronavirus (Paraskevis et al. 2020). This is not the first time that a coronavirus has created an epidemic and threatened global health (Di Gennaro et al. 2020). This is the third case of coronavirus pneumonia in the world in the past 20 years. For the first time in 2002, a beta-coronavirus caused acute respiratory syndrome coronavirus (SARS-CoV) in China and led to 8000 infections and 774 victims in 37 countries. Again in 2012, it gave rise to the Middle East Respiratory Syndrome (MERS-CoV) virus, which was discovered in Saudi Arabia, with 2494 infections and 858 deaths (De Wit et al. 2016; Otuonye et al. 2020).
After China, COVID-19 spread rapidly around the world and covered all continents and regions worldwide (Lai et al. 2020). The first confirmed case of COVID-19 outside of China was found on January 13, 2020, in Bangkok, Thailand (Di Gennaro et al. 2020). Italy, the United States of America, Iran, Turkey, Canada, South Korea, and Brazil are the countries which, in addition to China, have faced a major epidemic of this disease (Antonelli et al. 2020). Two risk factors can be mentioned for the spread of COVID-19, one is traveling to an area with a history of infection in the community in the past 14 days, and the other is having close relationships with people infected with the virus (Antonelli et al. 2020). This disease began in Iran on February 19, 2020, in the city of Qom in the center of Iran, and after a short period of time, it spread widely across all provinces (Salimi et al. 2020). The World Health Organization has declared that COVID-19 is a recognized public health concern. This epidemic is the sixth public emergency of international concern after H1N1 (2002), polio (2014), Ebola in West Africa (2014), Zika (2016), and Ebola in the Democratic Republic of Congo (2019) (Bazrafshan et al. 2020a, b; Delam and Eidi 2020). COVID-19 causes severe respiratory tract infections in humans. The most common symptoms at the beginning of the disease are fever, cough, shortness of breath, and fatigue. In addition, according to the results of the computed tomography (CT) diagnostic test, it was shown that there was abnormality and turbidity in the chest of all patients (Lake 2020; Zhai et al. 2020). Underlying diseases such as obesity, high blood pressure, diabetes, cardiovascular diseases, and chronic obstructive pulmonary disease (COPD) can affect the progression of the disease and the resulting weakness (Antonelli et al. 2020; Kang et al. 2020; Park et al. 2020). In the first days of the onset of the disease, the mean incubation period of the disease was 5.2 days (It varied from 1 to 19 days.) (Bulut and Kato 2020; Wilder-Smith and Freedman 2020). One of the classic public health measures to contain the epidemic of this disease was quarantine and social distancing (Wilder-Smith and Freedman 2020). In the wake of the pandemic, China imposed one of the largest lockdowns in history, including shutting down public transportation such as buses, trains, ferries, and airports (Zhai et al. 2020). In Iran, schools, educational institutions, and religious places were closed, gatherings were stopped, and a travel ban was imposed (Salimi et al. 2020).
Epidemiological investigation of diseases can play a valuable role in controlling epidemics and provide solid evidence to health policymakers so that they can plan timely and effectively to control epidemics. In this study, the researchers intend to comprehensively investigate the epidemiological aspects of COVID-19 in southern Iran in the period of February 2020 to July 2021.
Methods
Type of study
The present study was a cross-sectional analytical study.
Study group
This study included all people who had COVID-19 in the period from February 2020 to July 2021 whose information had been registered in the Infectious Diseases Center of Larestan city and MCMC unit.
Study area
The study area included the cities of Larestan, Evaz and Khonj, which are located in the south of Fars province, in the south of Iran. According to the latest population statistics registered in the apple system of the Ministry of Health, Treatment and Medical Education of Iran, the covered population in these three cities is approximately 272,000 people. In terms of climate, Larestan, Evaz, and Khonj are considered as arid regions, and the average annual rainfall in these regions from 2003 to 2010 was approximately 151.8 mm (Bazrafshan et al. 2020a, b). Larestan city is the largest city in the province of Fars in terms of area, which is located in the southern part of this province (Delam et al. 2020).
Ethical considerations
During all stages (completing a checklist and entering data into the software), the patients’ information was kept confidential.
Data collection
The researchers investigated all records of COVID-19 cases in the Centre for Communicable Diseases of Larestan between February 2020 and July 2021 from daily visits. This center records data pertaining to three cities in the south of Fars province: Larestan, Evaz, and Khonj.
Statistical analysis
After completing the checklists, the data were entered into SPSS, version 25. Descriptive and analytical statistics of the variables are represented by tables and figures. Frequency (percentage) was used to measure qualitative variables. The trend of COVID-19 incidence during these years was analyzed using the Cochran–Armitage trend test. A P-value less than 0.05 was considered significant.
Results
Descriptive statistics
New cases
Since the appearance of COVID-19 until July 2021, a total of 23,246 new cases of infection were reported in the southern region of Fars province. The mean age of patients was 39.90±18.30 years and the range of ages varied from 1 to 103 years. Most cases were female (50.2%), but there was no significant difference between men and women in terms of contracting the disease. Approximately 1351 cases (5.8 %) of all patients were admitted to the hospital due to worsening of their physical condition. Only 12.9% of patients had an underlying disease, and the majority of cases were residents of urban areas (Table 1).
Mortality
A total of 343 people died due to COVID-19. The mean age of the deceased was approximately 70.94±16.95 years. The majority of deceased cases were men (58.9%). In terms of nationality, 94.8% of the deceased were Iranian and 5.2% were Afghan, and 66.8% had one or more underlying diseases (Table 2).
Trends
Incidence in 2020
The results of the Cochran–Armitage trend test showed that the trend of the disease in 2020 was completely upward. The first positive case of COVID-19 was recorded on February 27, 2020. Over time and with the increase in the number of diagnostic tests, on June 03, the highest number of newly identified cases of COVID-19 were recorded. In general, we saw widespread epidemics in these areas in June and July. From the beginning of August to the end of October, the cases showed a significant decrease, but again in November, the cases increased rapidly. In general, the incidence of COVID-19 increased significantly in 2020 (P-trend < 0.001) (Fig. 1).

Changes in the incidence of COVID-19 in southern Iran in 2020
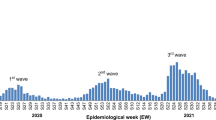
Incidence in 2021
With the increase in diagnostic tests, especially rapid diagnostic tests, positive cases also increased. With the increase in diagnostic tests, especially rapid diagnostic tests, positive cases also increased. The incidence curve in 2021 is sinusoidal, but in general, the results of the Cochran–Armitage trend test showed that the incidence of the disease has increased significantly (P-trend < 0.001). Most cases were observed in July, April, and late March (Fig. 2).

Changes in the incidence of COVID-19 in southern Iran in 2021
Mortality in 2020
The first death due to the disease was recorded on March 21, 2020. The highest number of deaths was reported on August 15. The results of the Cochrane–Armitage trend test for mortality in 2020 showed that mortality due to COVID-19 increased significantly (P-trend < 0.001) (Fig. 3).

Changes in the mortality of COVID-19 in southern Iran in 2020
Mortality in 2021
The first death in 2021 was observed on January 9. Contrary to the trend of deaths in 2020, in 2021 the trend of deaths was decreasing (P-trend = 0.518) (Fig. 4).

Changes in the mortality of COVID-19 in southern Iran in 2021
Discussion
The present study was designed with the aim of identifying the epidemiological characteristics of COVID-19 in the southern region of Fars province in southern Iran. The results of the study showed that women were more often infected with COVID-19 than men, although this percentage was not statistically significant. Gomes et al. (2021), as well as Tan et al. (2021), reported in their studies that women were more affected than men. It seems that the higher percentage of the disease in women is due to the fact that more women go to health-treatment centers to receive health care, and this causes the disease to be diagnosed in them earlier. In our study, men accounted for 58.90% of all deaths, showing men had higher mortality despite the lower incidence rate. Studies by Li et al. (2020), Rajabinejad and Asgarian-Omran (2021), Chen et al. (2020), Ejaz et al. (2021), and the report of the Epidemiology Working Team of the Chinese Center for Disease Control and Prevention (Team 2020) also reported a higher mortality rate in men. These statistics can be due to the fact that there are more ACE2 receptors in the lungs and hearts of men and people with heart disease, diabetes, and high blood pressure (these diseases are also more common in men) and this makes them more vulnerable to some diseases, including COVID-19 (Sama et al. 2020). Of course, in this statistical difference, sex hormones and the adaptive immune system may also play a significant role because the testosterone hormone in men suppresses the immune system, and the sex hormone estrogen helps women to fight viral infections (Jaillon et al. 2019; Klein et al. 2015; Salciccia et al. 2021). Also, women’s adaptive immune system has more CD4+ T cells (Abdullah et al. 2012). It seems that usually men go to health centers when the disease has progressed, and they have serious problems (Banks 2001). In 2020, the highest incidence occurred between May to July and from November to September. The incidence rate of COVID-19 in general in Iran also increased very rapidly between November 1 and December 30, 2020, so that the number of patients reached 1,200,000 from about 600,000 (Leite Junior et al. 2019). In the period from May to July 2020, there were events such as Muslim holidays and Ramadan, when people go to visit relatives and religious gatherings. Also, the closeness of the Nowruz holiday date to this period and the fact that weddings in these areas often take place during the period of Nowruz until the end of June may also explain this increasing trend in the incidence rate. The high incidence of the disease between September and November may also be due to the cold weather and gathering of people in homes, which can increase contacts and cause an outbreak of the disease. On the other hand, during this interval, the incidence of viral diseases such as influenza increases, which can lead to a decrease in the strength of the immune system and make people susceptible to other infections, including COVID-19. In 2020, the highest number of deaths was reported on August 15. The results of the 2020 Cochrane–Armitage mortality trends test showed that deaths due to COVID-19 had an upward trend, which may be because there were not many strategies to treat, control, and prevent the disease and the extent and availability of diagnostic kits was also limited. Contrary to the trend of deaths in 2020, in 2021 the trend of deaths was decreasing.
It seems that the downward trend of the disease in 2021 was due to the ease and extent of access to diagnostic tests for COVID-19 (identifying the disease earlier and in the early stages), more experience of health professionals, and vaccination against COVID-19.
Limitations of the study
One of the major limitations of the study was the lack of access to the clinical information of COVID-19 patients, which could help in identifying the epidemiological status of the disease. Also, another limitation of the study was the high number of missing data, which forced us to remove some variables.
Conclusion
In general, the incidence rate of COVID-19 varied sinusoidally from 2020 to mid-2021. Although the incidence of the disease increased, the number of deaths has fallen. It seems that the increase in the number of diagnostic tests and the implementation of the national COVID-19 immunization program have been effective in changing the trend of the disease. Therefore, it seems that educating the community in the field of health care and equipping the diagnostic centers for COVID-19 with more advanced diagnostic tests can help in early diagnosis of the disease and reducing severe cases. Also, the continuous implementation of the vaccination program can greatly reduce the incidence of disease or death caused by it. The trend of the disease shows that there is a possibility of an epidemic at any moment of time; therefore, it is still necessary for the health and medical personnel to be prepared and for the people to follow the health guidelines.
References
Abdullah M, Chai P-S, Chong M-Y, Tohit ERM, Ramasamy R, Pei CP, Vidyadaran S (2012) Gender effect on in vitro lymphocyte subset levels of healthy individuals. Cell Immunol 272(2):214–219. https://doi.org/10.1016/j.cellimm.2011.10.009
Antonelli A, Elia G, Ferrari SM, Foddis R, De Marco S, Cristaudo A, Fallahi P (2020) The COVID-19, epidemiology, clinic and prevention. Current Genomics 21(3):157
Banks I (2001) No man's land: men, illness, and the NHS. Bmj 323(7320):1058–1060. https://doi.org/10.1136/bmj.323.7320.1058
Bazrafshan M-R, Eidi A, Keshtkaran Z, Shokrpour N, Zand P, Delam H (2020a) Epidemiological and clinical aspects of the coronavirus disease 2019 (COVID-19) outbreak based on global data: a review article. J Health Sci Surveillance Syst 8(3):100–104. https://doi.org/10.30476/jhsss.2020.86851.1102
Bazrafshan M-R, Shokrpour N, Delam H (2020b) Ten-year trends of the incidence of Cutaneous Leishmaniasis in the South of Fars Province, Iran, During 2007-2016. Int J Epidemiol Res 7(3):120–124. https://doi.org/10.34172/IJER.2020.21
Bulut C, Kato Y (2020) Epidemiology of COVID-19. Turk J Med Sci 50(SI-1):563–570
Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, Zhang L (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 395(10223):507–513. https://doi.org/10.1016/S0140-6736(20)30211-7
De Wit E, Van Doremalen N, Falzarano D, Munster VJ (2016) SARS and MERS: recent insights into emerging coronaviruses. Nat Rev Microbiol 14(8):523
Delam H, Eidi A (2020) WhatsApp Messenger role in Coronavirus Disease 2019 (COVID 19) Pandemic. J Health Sci Surveillance Syst 8(4):183–184. https://doi.org/10.30476/jhsss.2020.87202.1107
Delam H, Shokrpour N, Nikbakht H-A, Hassanipour S, Safari K, Bazrafshan M-R (2020) Changing patterns in epidemiology of malaria between 2006 and 2018 in the South of Fars province, southern Iran: the fall and rise of malaria. Annals Global Health, 86(1)
Delam H, Moghaddam S, Zare R (2022) Efficacy and safety of COVID-19 vaccines in different variants and doses: a systematic review. Int J Epidemiol Res 9(4):184–195. https://doi.org/10.34172/EHSJ.2022.33
Di Gennaro F, Pizzol D, Marotta C, Antunes M, Racalbuto V, Veronese N, Smith L (2020) Coronavirus diseases (COVID-19) current status and future perspectives: a narrative review. Int J Environ Res Public Health 17(8):2690
Ejaz R, Ashraf MT, Qadeer S, Irfan M, Azam A, Butt S, Bibi S (2021) Gender-based incidence, recovery period, and mortality rate of COVID-19 among the population of district Attock, Pakistan. Braz J Biol 83:e249125. https://doi.org/10.1590/1519-6984.249125
Gomes DR, Souza RC, Oliveira UR, Mattos MP, Aleluia ÍRS, Mapeli AMJC, Coletiva S (2021) Inland expansion of COVID-19 in western Bahia: epidemiological profile and spatial analysis of deaths and confirmed cases. 26:4665-4680
Jaillon S, Berthenet K, Garlanda C (2019) Sexual dimorphism in innate immunity. Clin Rev Allergy Immunol 56(3):308–321. https://doi.org/10.1007/s12016-017-8648-x
Kang Z, Luo S, Gui Y, Zhou H, Zhang Z, Tian C, Fan H (2020) Obesity is a potential risk factor contributing to clinical manifestations of COVID-19. Int J Obes 44(12):2479–2485
Klein SL, Marriott I, Fish EN (2015) Sex-based differences in immune function and responses to vaccination. Trans R Soc Trop Med Hyg 109(1):9–15. https://doi.org/10.1093/trstmh/tru167
Lai C-C, Wang C-Y, Wang Y-H, Hsueh S-C, Ko W-C, Hsueh P-R (2020) Global epidemiology of coronavirus disease 2019 (COVID-19): disease incidence, daily cumulative index, mortality, and their association with country healthcare resources and economic status. Int J Antimicrob Agents 55(4):105946
Lake MA (2020) What we know so far: COVID-19 current clinical knowledge and research. Clin Med 20(2):124
Leite Junior JB, de Mello Bastos JM, Samuels RI, Carey RJ, Carrera MP (2019) Reversal of morphine conditioned behavior by an anti-dopaminergic post-trial drug treatment during re-consolidation. Behav Brain Res 359:771–782. https://doi.org/10.1016/j.bbr.2018.08.009
Li X, Xu S, Yu M, Wang K, Tao Y, Zhou Y, Zhao J (2020) Risk factors for severity and mortality in adult COVID-19 inpatients in Wuhan. J Allergy Clin Immunol 146(1):110–118. https://doi.org/10.1016/j.jaci.2020.04.006
Otuonye NM, Olumade TJ, Ojetunde MM, Holdbrooke SA, Ayoola JB, Nyam IY, Abayomi A (2020) Clinical and demographic characteristics of COVID-19 patients in Lagos, Nigeria: a descriptive study. J Natl Med Assoc 113(3):301–306. https://doi.org/10.1016/j.jnma.2020.11.011
Paraskevis D, Kostaki EG, Magiorkinis G, Panayiotakopoulos G, Sourvinos G, Tsiodras S (2020) Full-genome evolutionary analysis of the novel corona virus (2019-nCoV) rejects the hypothesis of emergence as a result of a recent recombination event. Infect Genet Evol 79:104212
Park M, Cook AR, Lim JT, Sun Y, Dickens BL (2020) A systematic review of COVID-19 epidemiology based on current evidence. J Clin Med 9(4):967
Rajabinejad M, Asgarian-Omran H (2021) COVID-19 gender difference pattern in Iranian population compared to the global pattern; a systematic review and meta-analysis. https://doi.org/10.1101/2021.05.23.21257692
Rothan HA, Byrareddy SN (2020) The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun 109:102433
Salciccia S, Del Giudice F, Eisenberg ML, Mastroianni CM, De Berardinis E, Ricciuti GP, Maggi M (2021) Testosterone target therapy: focus on immune response, controversies and clinical implications in patients with COVID-19 infection. Ther Adv Endocrinol Metab 12:20420188211010105. https://doi.org/10.1177/20420188211010105
Salimi R, Gomar R, Heshmati B (2020) The COVID-19 outbreak in Iran. J Glob Health 10(1)
Sama IE, Ravera A, Santema BT, van Goor H, Ter Maaten JM, Cleland JGF, Voors AA (2020) Circulating plasma concentrations of angiotensin-converting enzyme 2 in men and women with heart failure and effects of renin-angiotensin-aldosterone inhibitors. Eur Heart J 41(19):1810–1817. https://doi.org/10.1093/eurheartj/ehaa373
Tan TW, Tan HL, Chang MN, Lin WS, Chang CM (2021) Effectiveness of epidemic preventive policies and hospital strategies in combating COVID-19 outbreak in Taiwan. Int J Environ Res Public Health 18(7). https://doi.org/10.3390/ijerph18073456
Team ECCw (2020) The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19)—China, 2020. 2(8): 113
Wilder-Smith A, Freedman DO (2020) Isolation, quarantine, social distancing and community containment: pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J Travel Med
Xie M, Chen Q (2020) Insight into 2019 novel coronavirus—an updated interim review and lessons from SARS-CoV and MERS-CoV. Int J Infect Dis 94:119–124
Zhai P, Ding Y, Wu X, Long J, Zhong Y, Li Y (2020) The epidemiology, diagnosis and treatment of COVID-19. Int J Antimicrob Agents 55(5):105955
Acknowledgments
The present study with the code of 1400-92 was approved by the Student Research Committee of Larestan University of Medical Sciences. We sincerely thank the Student Research Committee for its financial support of the study.
Funding
We sincerely thank the Student Research Committee for its financial support of the study.
Author information
Authors and Affiliations
Contributions
HD and BR: designed the study. ASh, ArE, KhS, and RSh: screened and analyzed the data. HD, BZ, and ZK: drafted the manuscript. HD, Ash, and MA: critically revised the text of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
The present study with the code of IR.LARUMS.REC.1400.003 was approved by the ethics committee of Larestan University of Medical Sciences. Patient information remained confidential throughout the study.
Ethical considerations
During all stages (completing a checklist and entering data into the software), the patients’ information was kept confidential.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Conflict of interest
There is no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Rezaei, B., Shahedi, A., Keshtkaran, Z. et al. Changes in incidence and mortality trend due to COVID-19 in southern Iran, from 2020 to 2021: based on Cochran–Armitage trend test. J Public Health (Berl.) (2023). https://doi.org/10.1007/s10389-023-01902-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10389-023-01902-8