
Summary
Background
The aim of this retrospective study was to analyze the fulfillment of different fast-track elements in daily surgical practice.
Methods
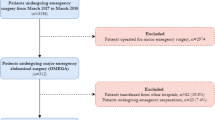
One hundred and forty-nine consecutive patients (69 female, 46 %) with a median(range) age of 68(33–93), were analyzed.
Results
In 46 % of patients no oral bowel preparation was performed. Successful placement of patent ductus arteriosus (PDA) was reached in 94(63 %) patients. Nasogastric tube was removed in 97 %, a drain was placed in 94(63 %) patients. The urine catheter was removed in 43 % until postoperative day (POD) 3. No intravenous medication was recorded in 25(16 %) patients on POD1. In 47(32 %) patients deviation from the postoperative fast-track protocol was observed. Hospital mortality was 0.7 % and rehospitalization rate was 5 %(n = 7).
Conclusion
In summary, this study shows that the extension of the enhanced recovery of surgery (ERAS) protocol in a large department with a great number of staff involved is challenging and needs permanent supervision. Bowel preparation and epidural anesthesia were the elements with worse compliance.


Similar content being viewed by others


References
Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth. 1997;78(5):606–17.
Wilmore DW, Kehlet H. Management of patients in fast track surgery. Br Med J. 2001;322:473–6.
Wind J, Polle SW, Fung Kon Jin PH, Dejong CH, von Meyenfeldt MF, Ubbink DT, Gouma DJ, Bemelman WA Laparoscopy and/or Fast Track Multimodal Management Versus Standard Care (LAFA) Study Group; Enhanced Recovery after Surgery (ERAS) Group. Systematic review of enhanced recovery programmes in colonic surgery. Br J Surg. 2006;93(7):800–9.
Hasenberg T, Keese M, Längle F, Reibenwein B, Schindler K, Herold A, Beck G, Post S, Jauch KW, Spies C, Schwenk W, Shang E. ‘Fast-track’ colonic surgery in Austria and Germany—results from the survey on patterns in current perioperative practice. Colorectal Dis. 2009;11:162–7.
Lyon A, Payne CJ, Mackay GJ. Enhanced recovery programme in colorectal surgery: does one size fit all? World J Gastroenterol. 2012;18:5661–3.
Guillou PJ, Quirke P, Thorpe H, Walker J, Jayne DG, Smith AM, Heath RM, Brown JM. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre, randomized controlled trial. Lancet. 2005;365:1718–26.
Schwenk W, Haase O, Neudecker J, Müller JM. Short term benefits for laparoscopic colorectal resection. Cochrane Database Syst Rev. 2005;3:CD003145
Maessen J, Dejong CH, Hausel J, Nygren J, Lassen K, Andersen J, Kessels AG, Revhaug A, Kehlet H, Ljungqvist O, Fearon KC, von Meyenfeldt MF. A protocol is not enough to implement an enhanced recovery programme for colorectal resection. Br J Surg. 2007;94(2):224–31
Jung B, Påhlman L, Nyström PO, Nilsson E, Mechanical Bowel Preparation Study Group. Multicentre randomized clinical trial of mechanical bowel preparation in elective colonic resection. Br J Surg. 2007;94(6):689–95.
van de Velde CJ, et al. Experts reviews of the multidisciplinary consensus conference colon and rectal cancer 2012: science, opinions and experiences from the experts of surgery. Eur J Surg Oncol. 2014;40(4):454–68
Ahmed J, Khan S, Lim M, Chandrasekaran TV, MacFie J. Enhanced recovery after surgery protocols—compliance and variations in practice during routine colorectal surgery. Colorectal Dis. 2012;14(9):1045–51.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Bräunlein, J., Gasser, E. & Kafka-Ritsch, R. Compliance with and fulfillment of a fast-track protocol in daily surgical practice in a university hospital. Eur Surg 47, 45–48 (2015). https://doi.org/10.1007/s10353-015-0303-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10353-015-0303-2