
Abstract
Aim
This paper reports the first estimation of an SF-6D value set based on the SF-12 for Spain.
Methods
A representative sample (n = 1020) of the Spanish general population valued a selection of 56 hypothetical SF-6D health states by means of a probability lottery equivalent (PLE) method. The value set was derived using both random effects and mean models estimated by ordinary least squares (OLS). The best model was chosen on the basis of its predictive ability assessed in terms of mean absolute error (MAE).
Results
The model yielding the lowest MAE (0.075) was that based on main effects using OLS. Pain was the most significant dimension in predicting health state severity. Comparison with the previous SF-6D (SF-36) model estimated for Spain revealed no significant differences, with a similar MAE (0.081). Nevertheless, the new SF-6D (SF-12) model predicted higher utilities than those generated by the SF-6D (SF-36) scoring algorithm (minimum value − 0.071 vs − 0.357).
Conclusion
A value set for the SF-6D (SF-12) based on Spanish general population preferences elicited by means of a PLE technique is successfully estimated. The new estimated SF-6D (SF-12) preference-based measure provides a valuable tool for researchers and policymakers to assess the cost-effectiveness of new health technologies in Spain.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Quality-adjusted life years (QALYs) are commonly recommended as the preferred outcome measure to be used in health technology assessment (HTA) [1], as they combine survival and health-related quality of life (HRQoL) into a single number [2]. Utility weights used to calculate QALY-based cost-effectiveness ratios can be obtained from health-related multiattribute utility (MAU) instruments, such as, among others, the EuroQol five-dimensions (EQ-5D), with three or five levels [3, 4], Assessment of Quality of Life [5], Health Utilities Index (HUI) 2 and 3 [6, 7], and the two versions of the six-dimensional health state Short Form (SF-6D) derived from the Short-Form 36 (SF-36) health survey [8, 9]. All these MAU instruments use value sets, also called tariffs, based on the preferences elicited from a representative sample of the general population by means of valuation techniques such as discrete choice experiment (DCE) [2, 10, 11], time trade-off (TTO) [2, 10, 12, 13], standard gamble (SG) [8], or lottery equivalent (LE) methods [14].
The SF-36 is a 36-item questionnaire [15] that covers eight health domains: physical functioning, role limitations due to physical health, role limitations due to emotional problems, energy/fatigue or vitality, emotional well-being or mental health, social functioning, bodily pain, and general health. There are two versions of the SF-36 [16, 17] that differ in the number of response choices on some items and the way that domain scores are interpreted. This health survey is commonly used in health status assessment and HTA [18, 19]. The SF-36 has been translated and validated in various languages, including Spanish, following a standardized procedure [20].
The SF-12 health survey is a shortened version of the SF-36 questionnaire, comprising 12 items. As occurred with the SF-36, there are also two versions of the SF-12 questionnaire [21, 22]. Existing evidence suggests that the SF-12 can replicate more than 90 percent of the variance in both physical and mental component summary scores of the SF-36 [22, 23], demonstrating reliability and validity as a shorter form of the questionnaire [21, 24].
Neither the SF-36 nor the SF-12 can yield utility weights by themselves, so they are not able to compute QALYs directly. Nevertheless, as SF-6D health states are based on SF-36/SF-12 items, value sets for the SF-6D allow analysts and practitioners to attach preference scores to SF-36/SF-12 surveys. In this way, the seminal study conducted by Brazier et al. [8] estimated the SF-6D value set from the SF-36 for the UK. Later on, Brazier and Roberts [25] inferred the SF-6D value set from the SF-12 using the same data set of the previous study [8].
In contrast to the UK, there is no SF-6D value set derived from the SF-12 for Spain; there is only one SF-6D tariff based on the SF-36 [14]. This article aims to address this gap by presenting a new SF-6D value set derived from the SF-12 and comparing it with the previous one based on the SF-36, both originated from the same survey, similar to what Brazier and Roberts [25] did for the UK.
The paper is organized as follows. The next section describes the design of the valuation survey, as well as the health states selected, the elicitation procedure applied to value them, and the modeling strategy used to estimate the SF-6D (SF-12) value set. Section “Results” shows the main results of our study, including the model finally chosen. The estimated value set is compared to that previously estimated from the SF-36 in Spain and to the SF-6D (SF-12) UK’s tariff as well. Finally, “Discussion” closes the paper.
Methods
Study design
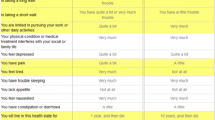
The valuation survey was designed to value health states defined by the SF-6D (SF-36), and the data from this survey are used in this study to estimate a preference-based scoring algorithm for the SF-6D (SF-12). This version of the SF-6D is shown in Table 1.
A representative sample of the general Spanish population (n = 1020) was obtained through a two-stage stratified sampling methodology. To optimize the response rate, recruitment strategies included advance contact, reminders, appointment scheduling, and small gifts. Since the survey was sponsored by the Department of Health, high collaboration was achieved, obtaining a response rate of 90%. The survey received approval from the ethics committee. Respondents were interviewed and grouped into 17 subsamples, consisting of 60 individuals each. Each respondent valued a maximum of 5 health states out of a total of 78 using a probability lottery equivalent (PLE) method. The detailed design of the survey has been reported elsewhere [14].
Selection of health states
As noted above, a total of 78 SF-6D (SF-36) health states were used in the survey. Of these, 49 were obtained by running the Orthoplan module of SPSS version 17, which yields the minimum subset of states, which allows the estimation of an additive model. The remaining states (including the worst possible SF-6D state, the so-called ‘pits’ state) up to 78 were included to estimate potential interaction effects between attributes. This subset of 78 health states, originally selected for the estimation of the SF-6D (SF-36) tariff [14], was reduced to 56 states (Table 2) to estimate the SF-6D (SF-12) algorithm. Since the PF and PAIN dimensions have a more reduced number of levels in the SF-12-based version of the SF-6D than in the SF-36-based one, some states were excluded from the estimation.
In the initial setup, all respondents were required to assess 5 health states, which were randomly distributed across the 17 models from the original pool of 78 states. Consequently, some health states were evaluated in more than one model, leading to a higher number of valuations. As a consequence of reducing the number of health states from 78 to 56 compatible with the SF-12, the range of health states valued by each individual considered for modeling varies between 2 and 5.
The interviews
Data were collected through face-to-face computer-assisted personal interviews (CAPI) conducted by trained interviewers. The average duration per interview was around 20 min. The survey was divided into four parts. First, the SF-6D classification system was explained to the respondents. Second, they were asked to rate five SF-6D health states on a visual analogue scale. Next, preference weights for the five health states were elicited using the PLE. Specifically, information was gathered concerning gender, marital status, highest level of education attained, monthly income, and health habits, such as whether the interviewee was a smoker or not. Regarding health status, respondents fulfilled both EQ-5D-3L and SF-12 instruments.
Valuation method
The PLE asks for the probability p that makes the respondents indifferent between the gamble denoted by (full health, p; death), yielding full health with probability p and death with probability 1–p, and the gamble denoted by (full health, 0.5; h), yielding full health and the health state h with the same probability. This approach enabled us to capture preferences for states regarded as both better and worse than death. If the respondent favored the second gamble over the first in the initial question (i.e., for p = 0.5), it indicated that state h was perceived as preferable to death. Consequently, the ultimate probability of indifference, denoted as p*, was elicited within the range of 0.5 to 1. Conversely, if the first gamble was preferred over the second for p = 0.5, then state h was considered worse than death, and p* was elicited within the range of 0 to 0.5. Following the expected utility theory, assuming the convention that the utility of perfect health is 1 and the utility of death is 0, the utility of health state h is calculated as U(h) = 2p* – 1.
Modeling
Our initial specification is a model without interactions between variables, that is, a main effects model, whose constant term was forced to unity to ensure that the utility of full health equals one. In our analysis, we introduced a dichotomous variable labeled 'MOST,' taking a value of 1 if any dimension reached its maximum level and 0 otherwise. We also introduced a variable aiming to capture the total sum of dimensions within the state. However, these variables did not improve the model in any case, leading to their exclusion from the final specification. The model was estimated by following a dual regression approach, as common in many studies [8, 26,27,28,29], using both ordinary least squares (OLS) and random effects (RE) estimators. The optimal model is chosen on the basis of its predictive ability in terms of mean absolute error (MAE) and the proportion of predictions outside 0.01, 0.05, and 0.1 ranges on either side of the actual value.
Results
The sample
A total of 15 participants were excluded from the analysis due to ordinal inconsistencies in their PLE valuations. Such inconsistencies came from the fact that some health states could be logically ordered, i.e., one of them had an equal or higher (worse) level than the other one in each of the six dimensions. An ordinal inconsistency occurred when a higher value was assigned to a logically more severe health state than to a less severe one. Furthermore, seven respondents were excluded from the analysis because they were not willing to accept any risk of death to improve their health, thus implicitly assigning a utility 1 to a health state which is worse than perfect health. After exclusions, the final sample used to estimate the SF-6D (SF-12) scoring algorithm consisted of 998 individuals. This exclusion rate (2.16%) is slightly lower than that observed in the Dutch study [31], which was 2.5%. Table 3 shows the sociodemographic characteristics of this sample. Compared to the general Spanish population, some differences arise in terms of educational achievements and income earnings.
The data set
Each of the 56 health states presented in Table 4 was assessed an average of 64 times, with a minimum of 56 participants and a maximum of 119 participants providing valuations. Mean values range from 0.139 to 0.988, exhibiting substantial standard deviations. Notably, the distribution of intended sample sizes for valuation is bimodal—60 for a subset of health states and 120 for the remainder. Consequently, relying exclusively on mean values may not adequately capture the full distributional properties of the data. The utility scores themselves demonstrate non-normal distributional attributes, as characterized by a negative skewness of -0.840 and elevated kurtosis of 5.077, indicative of a platykurtic and left-skewed distribution. The median utility score stands at 0.6, and the 25th and 75th percentiles are 0.38 and 0.8, respectively. Notably, no median values below zero were observed, which aligns with findings reported by Brazier and Roberts [25]. Approximately, 23% of the health states received negative utility values from at least one participant, contrasting with Brazier and Roberts' study, which reported a lower occurrence of negative utilities [25].
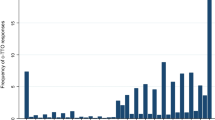
Figure 1 completes the picture shown in Table 4. It displays a histogram and some descriptive statistics for the whole distribution of SF-6D (SF-12) individual valuations.

Utility histogram of SF-6D (SF-12) and SF-6D (SF-36)
Table 5 shows coefficients estimated for five models. All the models predict SF-6D (SF-12) utilities except for model (5) which is based on the SF-36 [14]. Models (1) and (2) are RE models, while models (3), (4), and (5) are OLS models using mean values with corrective weights proportional to the number of individuals valuing each health state. ‘Raw models’ are models without the removal of non-significant variables, whereas ‘efficient models’ were constructed by eliminating non-significant regressors from ‘raw models’ and by grouping the variables of any two consecutive levels when their coefficients are not significantly different from each other according to the value of the Wald statistic. We did not find any significant interaction term, so all our algorithms only reflect the main effects.
The lowest MAE among the five models corresponds to model (4), which is slightly lower (0.075) than that (0.079) attached to the recommended SF-6D (SF-12) model for the UK [25]. Notwithstanding, all five models exhibit small, unbiased, and normally distributed MAE values. When comparing models (4) and (5) each other, RL and SF dimensions are weighted heavier in the former rather than the latter one. Across all five models, PAIN appears to be the most influential dimension in determining health state values. The PF dimension has a greater importance in generating health state values in the SF-6D (SF-36) algorithm for Spain but loses relevance in all the SF-6D (SF-12) models.
The results presented in Table 5 can be used to estimate utility weights for each health state. For example, the estimated value for state 344444 is 0.183 according to the SF-6D (SF-12) model 4 (calculated as 1–0.096–0.084–0.207–0.186–0.090–0.154), and 0.242 from the SF-6D (SF-36) model 5.
In comparing the utility weights assigned to each health state according to the SF-6D (SF-36) and SF-6D (SF-12) frameworks (Fig. 1), a higher prevalence of utilities falling below zero is discernible in the SF-6D (SF-36) version [14]. Although both value sets display negative skewness, this is more accentuated in the SF-6D (SF-12) version, which also records a higher frequency of utilities equating to unity. Notably, while both utility distributions share identical minimum and maximum values, the SF-6D (SF-12) value set registers higher median and mean values.
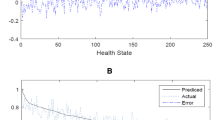
Figure 2 illustrates the strong correlation between the utilities predicted by our preferred model (model 4) and those directly elicited from the respondents by the PLE for the same health states. In contrast to the Brazier and Roberts’ model for the SF-6D (SF-12) (see Fig. 1 in their article [25]) our model does not tend to overpredict the value for poor health states as their model does. This fact suggests that the Spanish tariff is not affected by floor effects. The conclusion is further substantiated by Fig. 3, which demonstrates that the Spanish tariff yields lower utility values in comparison to its UK counterpart.

Plot of actual and predicted values for model 4

A comparison of the SF-6D (SF-12) Spanish and UK tariffs’ predicted values
Discussion
This paper provides the first estimation of an SF-6D (SF-12) tariff ever done for Spain. It adds to the unique two previous estimations of the SF-6D value set from the SF-12 reported elsewhere [30] for the British [25] and Dutch [31] populations. The estimates reported in this article will allow analysts and practitioners to attach utility weights to patients’ health states described in the SF-12 survey.
The approach followed in the study reported in this paper to estimate an SF-6D (SF-12) value set is similar to that carried out in the UK [25]. In both cases, the valuation survey was designed to value health states defined by the SF-6D (SF-36), and the data from these surveys were used for the estimation of the SF-6D tariff from the SF-12. In addition, regression approaches used in the two studies are also quite similar. Differences arise between the two studies, however, in the set of health states selected, the number of them valued by each respondent, and the sample size. Brazier and Roberts [25] used a set of 249 health states, over four times our selection of 56 states. Respondents of our larger sample (998 vs 611), in return, valued a maximum of 5 health states each, one less than the number valued by each participant in the UK’s sample. Nevertheless, the biggest difference between both studies is due to the valuation technique used to value the health states. Whereas in the British study [25] valuations were elicited by means of the SG, a PLE method was used in ours.
This later difference is relevant because the distribution of predicted values by the model recommended in this paper extends utilities over a wider range than the UK tariff, ‘lowering’ the SF-6D (SF-12) floor. This mitigation of floor effects is due, as explained with regard to the SF-6D (SF-36) by Abellán-Perpiñán et al. [14], to the LE method used [32], i.e., the PLE, avoids the so-called ‘certainty effect’ (34), a bias that distorts SG measurements. Otherwise, the SF-6D (SF-12) model recommended in this paper has a slightly better predictive ability than Brazier and Roberts’ [25] preferred model while it does not tend to overpredict poor health states. Our tariff outperforms the UK’s one in terms of a closer correlation between predicted and actual valuations.
On the contrary, our study is not easily comparable to Jonker et al. [31] because both empirical designs are very different. The aim of the Jonker et al.’s [31] study is to estimate a time-preference corrected QALY tariff, the reason why they combine SF-6D (SF-12) health states with different life years in the pairwise choices that respondents have to make. The inclusion of life duration as an additional attribute allows the authors to accommodate nonlinear time preferences in DCE studies. As Jonker et al. [31] argue the assumption of linear time preferences can explain, at least partially, the relatively low QALY values usually reported in DCE duration studies compared to those based on TTO. It has to be noted, however, that in contrast to the TTO the PLE method used in our study is free from utility curvature biases, so our utilities do not have to be corrected to prevent that bias.
The ranking in terms of the importance of different dimensions is known to have cultural roots, and significant differences have been observed between countries and cultures (Wang and Poder (2023)) [30]. The order obtained in this study is not markedly different from that observed in previous studies for SF-6D (SF-12). Indeed, both the British study, with a ranking headed by PAIN and followed by MH, SF, VIT, PF, RL, and the Dutch study, with a ranking described by PAIN, MH, VIT, SF, PF, RL, show similarities to the one obtained in this study (PAIN, SF, MH, VIT, PF, RL). As in the two previous studies, PAIN and MH play a prominent role, while PF and RL occupy the lower positions. The comparison of the estimated tariff in this article with the Spanish tariff of the SF-6D (SF-36) [14] highlights the shifting impact on health dimensions. Indeed, in the SF-6D (SF-36) algorithm, it was PF the dimension that could potentially lead to the highest decrease in utility, whereas in the one presented here, it is PAIN the dimension placing such a position. In our view, this diminishing significance is primarily explained by the alteration in the instrument's structure, particularly the reduction from 6 to 3 levels in the PF dimension.
A limitation of this study resides in the sample size. It is important to acknowledge that our sample size of 1020 participants falls slightly below the optimal threshold for achieving full representativeness, as a minimum of 1,067 participants is typically required for a representative sample with 95% confidence and a 3% margin of error. Nonetheless, the sample size used in this study is clearly larger than the one used for the study in the UK [25], but smaller than that of the study conducted in the Netherlands [31]. Another limitation of this work is that the database used was generated more than a decade ago [14], however, it does not seem an unrealistic assumption to think that preferences for health states enjoy some temporal stability. Indeed, the best proof of this is that the tariffs of Brazier et al. [8] or Dolan [12] continue to be used, despite being substantially older. Another limitation of this study pertains to the slight discrepancies in income and educational level between our sample and the adult Spanish population. This constraint could be addressed in a manner akin to the approach employed by Méndez et al. [34]. However, in the interest of facilitating comparability with the extant tariff calculated using the same dataset [14], we have opted for an analogous analysis.
The survey did not incorporate any tasks to assess the numerical skills of the participants, which is unfortunate. This represents a limitation of the study, as elicitation through Probability-Lottery Equivalent (PLE) is a complex task that involves risk communication. Nevertheless, the survey did include some explanations about the risk and how to articulate it. Effective risk communication strategies described in the literature were employed: visual aids were utilized for risk communication [35] and the risks were presented as natural frequencies, a format known to enhance understanding [36]
A natural extension of this work involves estimating the SF-6Dv2 [9] tariff for the Spanish population. The SF-6Dv2 score is derived from 10 items of the SF-36v2. Compared to the SF-6Dv1, the SF-6Dv2 delineates more discrete health levels and diminishes floor effects. To the best of our knowledge, a tariff for SF-6Dv2 has been estimated only for a limited number of countries: UK [37], China [38], and Australia [11]
The availability of an SF-6D (SF-12) value set free from floor effects as that reported in this paper offers at least two advantages. First, it ensures that the instrument is sensitive enough to capture even the poorest health states, allowing for accurate assessment of severe health conditions and disabilities. Furthermore, a floor-free SF-6D tariff from the SF-12 enables comprehensive and reliable comparisons of health outcomes across different populations and interventions. This facilitates unbiased cost-effectiveness analyses and, hence, a more efficient resource allocation.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Code availability
Not applicable.
References
National Institute for Health and Care Excellence (NICE). Guide to the methods of technology appraisal 2013. London (2013).
Brazier, J., Ratcliffe, J., Saloman, J., & Tsuchiya, A. (2016). Measuring and Valuing Health Benefits for Economic Evaluation (2nd ed.). Oxford University Press. https://doi.org/10.1093/med/9780198725923.001.0001
Brooks, R.: EuroQol: The current state of play. Health Policy 37(1), 53–72 (1996). https://doi.org/10.1016/0168-8510(96)00822-6
Herdman, M., Gudex, C., Lloyd, A., Janssen, M., Kind, P., Parkin, D., Bonsel, G., Badia, X.: Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 20(10), 1727–1736 (2011). https://doi.org/10.1007/s11136-011-9903-x
Hawthorne, G., Richardson, J., Day, N.A.: A comparison of the Assessment of Quality of Life (AQoL) with four other generic utility instruments. Ann. Med. 33(5), 358–370 (2001). https://doi.org/10.3109/07853890109002090
Torrance, G.W., Feeny, D.H., Furlong, W.J., Barr, R.D., Zhang, Y., Wang, Q.: Multiattribute utility function for a comprehensive health status classification system: Health Utilities Index Mark 2. Med. Care 34(7), 702–722 (1996). https://doi.org/10.1097/00005650-199607000-00004
Feeny, D., Furlong, W., Torrance, G.W., Goldsmith, C. H., Zhu, Z., DePauw, S., ... Boyle, M. (2002). Multiattribute and single-attribute utility functions for the Health Utilities Index Mark 3 system. Medical Care, 40(2), 113–128. https://doi.org/10.1097/00005650-200202000-00006
Brazier, J., Roberts, J., Deverill, M.: The estimation of a preference-based measure of health from the SF-36. J. Health Econ. 21(2), 271–292 (2002). https://doi.org/10.1016/S0167-6296(01)00130-8
Brazier, J.E., Mulhern, B.J., Bjorner, J.B., Gandek, B., Rowen, D., Alonso, J., Vilagut, G., Ware, J.: Developing a new version of the SF-6D health state classification system from the SF-36v2: SF-6Dv2. Med. Care 58(6), 557–565 (2020). https://doi.org/10.1097/MLR.0000000000001325
Wu, J., Xie, S., He, X., Chen, G., Bai, G., Feng, D., Hu, M., Jiang, J., Wang, X., Wu, H., Wu, Q., Brazier, J.E.: Valuation of SF-6Dv2 health states in China using time trade-off and discrete-choice experiment with a duration dimension. Pharmacoeconomics 39(5), 521–535 (2021). https://doi.org/10.1007/s40273-020-00997-1
Mulhern, B., Norman, R., Brazier, J.: Valuing SF-6Dv2 in Australia using an international protocol. Pharmacoeconomics 39(10), 1151–1162 (2021). https://doi.org/10.1007/s40273-021-01043-4
Dolan, P.: Modeling valuations for EuroQol health states. Med. Care 35(11), 1095–1108 (1997). https://doi.org/10.1097/00005650-199711000-00002
Devlin, N.J., Shah, K.K., Feng, Y., Mulhern, B., van Hout, B.: Valuing health-related quality of life: An EQ-5D-5L value set for England. Health Econ. 27(1), 7–22 (2018). https://doi.org/10.1002/hec.3564
Abellán Perpiñán, J.M., Sánchez Martínez, F.I., Martínez Pérez, J.E., Méndez, I.: Lowering the ‘floor’ of the SF-6D scoring algorithm using a lottery equivalent method. Health Econ. 21(10), 1271–1285 (2012). https://doi.org/10.1002/hec.1792
Ware, J.E., Snow, K., Kosinski, M., Gandek, B. : SF-36 Health Survey Manual and Interpretation Guide.The Health Institute, New England Medical Center, Boston (1993)
Ware, J.E., & Sherbourne, C.D. (1992). The MOS 36-Item Short-Form Health Survey (SF-36): I. Conceptual framework and item selection. Medical Care, 30(6), 473–483.
Ware, J.E., Kosinski, M., Dewey, J.E.: How to Score Version 2 of the SF-36 Health Survey. Lincoln, QualityMetric Incorporated (2000)
Norwegian Medicines Agency: The National System for the Introduction of New Health Technologies Within the Specialist Health Service, Oslo (2014).
Health Information and Quality Authority (HIQA): Guidelines for the Economic Evaluation of Health Technologies in Ireland, Dublin (2020)
Aaronson, N.K., Acquadro, C., Alonso, J., Apolone, G., Bucquet, D., Bullinger, M., Bungay, K., Fukuhara, S., Gandek, B., Keller, S., Razavi, D., Sanson-Fisher, R., Sullivan, M., Wood-Dauphinee, W., Wagner, A., Ware, J.E.: International quality of life assessment (IQOLA) project. Qual. Life Res. 1(5), 349–351 (1992). https://doi.org/10.1007/BF00434949
Ware, J.E., Kosinski, M., Keller, S.D.: A 12-item short-form health survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 34(3), 220–233 (1996). https://doi.org/10.1097/00005650-199603000-00003
Ware, J.E., Kosinski, M., Turner-Bowker, D.M: How to Score Version 2 of the SF-12 Health Survey. QualityMetric Incorporated, Lincoln (2002).
Ware, J.E., Kosinski, M., Keller, S.D.: SF-12: How to score the SF-12 physical and mental health summary scales. QualityMetric Incorporated, Boston (2002)
Gandek, B., Ware, J.E., Aaronson, N.K., Apolone, G., Bjorner, J.B., Brazier, J.E., Bullinger, M., Kaasa, S., Leplege, A., Prieto, L., Sullivan, M.: Cross-validation of item selection and scoring for the SF-12 Health Survey in nine countries: Results from the IQOLA Project. J. Clin. Epidemiol.Clin. Epidemiol. 51(11), 1171–1178 (1998). https://doi.org/10.1016/s0895-4356(98)00109-7
Brazier, J.E., Roberts, J.: The estimation of a preference-based measure of health from the SF-12. Med. Care 42(9), 851–859 (2004). https://doi.org/10.1097/01.mlr.0000135827.18610.0d
Ferreira, L.N., Ferreira, P.L., Pereira, L.N., Brazier, J., Rowen, D.: Portuguese value set for the SF-6D. Value in Health 13(5), 624–630 (2010). https://doi.org/10.1111/j.1524-4733.2010.00701.x
Lam, C.L., Brazier, J., McGhee, S.M.: Valuation of the SF-6D health states is feasible, acceptable, reliable, and valid in a Chinese population. Value in Health 11(2), 295–303 (2008). https://doi.org/10.1111/j.1524-4733.2007.00233.x
Brazier, J.E., Fukuhara, S., Roberts, J., Kharroubi, S., Yamamoto, Y., Ikeda, S., Doherty, J., Kurokawa, K.: Estimating a preference-based index from the Japanese SF-36. J. Clin. Epidemiol.Clin. Epidemiol. 62(12), 1323–1331 (2009). https://doi.org/10.1016/j.jclinepi.2009.01.022
Cruz, L.N., Camey, S.A., Hoffmann, J.F., Rowen, D., Brazier, J.E., Fleck, M.P., Polanczyk, C.A.: Estimating the SF-6D value set for a population-based sample of Brazilians. Value in Health 15(5), S108–S114 (2011). https://doi.org/10.1016/j.jval.2011.05.012
Wang, L., Poder, T.G.: A systematic review of SF-6D health state valuation studies. J. Med. Econ. 26(1), 584–593 (2023). https://doi.org/10.1080/13696998.2023.2195753
Jonker, M.F., Donkers, B., de Bekker-Grob, E.W., Stolk, E.A.: Advocating a paradigm shift in health-state valuations: The estimation of time-preference corrected QALY tariffs. Value in Health 21(8), 993–1001 (2018). https://doi.org/10.1016/j.jval.2018.01.016
McCord, M., de Neufville, R.: Lottery equivalents: Reduction of the certainty effect problem in utility assessment. Manage. Sci. 32(1), 56–60 (1986). https://doi.org/10.1287/mnsc.32.1.56
Kahneman, D., Tversky, A.: Prospect theory: An analysis of decision under risk. Econometrica 47(2), 263–291 (1979). https://doi.org/10.2307/1914185
Méndez, I:, Abellán, J.M, Sánchez, F.I., Martínez, J.E. (2011). Inverse probability weighted estimation of social tariffs: an illustration using the SF-6D value sets. Journal of Health Economics 30(6), 1280–92. https://doi.org/10.1016/j.jhealeco.2011.07.013
García-Retamero, R., Okan, Y., Cokely, Y. (2012). Using visual aids to improve communication of risks about health: a review. Scientific World Journal:562637. https://doi.org/10.1100/2012/562637
Gigerenzer, G.: What are natural frequencies? Doctor need to find better ways to communicate risk to patients. BMJ 343, d6386 (2011). https://doi.org/10.1136/bmj.d6386
Mulhern, B.J.,Bansback, N.,Norman, R., Brazier, J.(2020).Valuing the SF-6Dv2 classification system in the United Kingdom using a discrete choice experiment with duration. MedicalCare 58(6):566573
Xie,S.,Wu,J.,He,X., Chen, G, Brazier, J.(2020).Do discrete choice experiments approaches perform better than time trade-off in eliciting health state utilities? Evidence from SF-6Dv2 in China. Value in Health. 2020;23(10):1391–1399. https://doi.org/10.1016/j.jval.2020.06.010
Acknowledgements
The research leading to these results received funding from the Spanish State Research Agency under Grant Agreement No PID2019-104907GB-I00
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature. Grant PID2019-104907 GBI00 funded by MCIN/AEI/ 10.13039/501100011033. Jorge-Eduardo Martínez-Perez; Fernando-Ignacio Sánchez-Martínez; José-María Abellán-Perpiñán.
Author information
Authors and Affiliations
Contributions
JEMP: study concept and design; data analysis and interpretation; writing-original draft; writing-review and editing. JMAP: study concept and design; data analysis and interpretation; writing–review and editing. FISM: study concept and design; data analysis and interpretation; writing–review and editing JJRL: study concept and design; data analysis and interpretation; writing-original draft; writing–review and editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent to publish
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Martínez-Pérez, JE., Abellán-Perpiñán, JM., Sánchez-Martínez, FI. et al. A Spanish value set for the SF-6D based on the SF-12 v1. Eur J Health Econ (2024). https://doi.org/10.1007/s10198-023-01657-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10198-023-01657-9