
Abstract
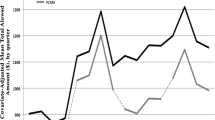
In many health care systems GPs receive fees for their services. Policymakers may use the size of these fees to try to incentivise GPs to provide more care. However, evidence is mixed on whether and how GPs respond to an increase in the fee size. This study investigates how GPs respond to an average increase of 150% in the fee for a high-effort and infrequent service such as a home visit due to patients’ illness. We consider Danish GPs’ provision of these visits to enlisted patients living outside of nursing homes. Using linear regressions with general practice fixed effects and a rich number of control variables, we estimate the association between GPs’ provision of these home visits and the fee rise. On average, we find no association between the fee rise and GPs’ provision of home visits. However, we find that GPs who previously provided the fewest home visits to eligible patients increase their provision by 13% after the fee rise compared to other GPs. This increase in visits is driven by more patients receiving multiple visits after the fee rise. We conclude that a fee rise may not yield a strong response in GPs’ provision of high-effort and infrequent services such as home visits.
Similar content being viewed by others
Availability of data and material
The data used in this paper are from pseudonymised register data held by Statistics Denmark. The data is confidential and person identifiable. Thus, we are unable to make any of the data publicly available.
Code availability
All analyses were conducted using STATA 15. The code used remains on the secure server where all the data are stored.
Notes
A regular practice consultation yields a consultation fee of around €20.
As we only know the year patients move to a nursing home, we assume that all visits to these patients in the year of the move are to a nursing home. Thus, we are likely overestimating the number of nursing home visits.
We define being active as having billed for services each year during our analysis period.
The DREAM database includes information on public transfer payments and employment status.
We also investigated whether differences in enlisted patients over 75 years olds mortality rates across practices could be driving our findings for this indicator. Appendix 4 shows no significant differences in death rates across the subgroups of GPs. The observed increase in mortality rate across GPs in 2016 may be explained by a hard flu season, which led to an increase in mortality among frail patients [22].To further support that mortality rates are not driving our findings, we find that our results are robust to controlling for mortality rates of enlisted patients over 75 years olds (see appendix 4).
One could also argue that a high activity level per enlisted patient could reflect abundant resources. However, as we in our analysis include a large array of controls, including the number of patients on the GPs’ list and their case-mix, we find it likely that the higher activity per patient over and above these factors is a measure of pressure on resources.
See the definition of this baseline group in the above presentation of each heterogeneity indicator.
As we include practice fixed effects, our baseline year (2015) is independent of each subgroup’s average service provision.
We do not control for this variable in the heterogeneity analysis where we group the GPs based on their average revenue per enlisted patient in the previous year.
A regular practice consultation yields a consultation fee of around €20.
The findings for the outcome “the number of inpatient hospitalisations” is available upon request.
References
OECD, Better Ways to Pay for Health Care. 2016.
Brekke, K.R., et al.: Do treatment decisions depend on physicians’ financial incentives? J. Public Econ. 155, 74–92 (2017)
Callison, K., Nguyen, B.T.: The effect of medicaid physician fee increases on health care access, utilization, and expenditures. Health Serv. Res. 53(2), 690–710 (2018)
Atherly, A., Mortensen, K.: Medicaid primary care physician fees and the use of preventive services among Medicaid enrollees. Health Serv Res 49(4), 1306–1328 (2014)
Carlsen, F., Grytten, J., Skau, I.: Financial incentives and the supply of laboratory tests. Eur J Health Econ Former: HEPAC 4(4), 279–285 (2003)
OECD, Realising the Potential of Primary Health Care. 2020.
Aylin, P., Majeed, F.A., Cook, D.G.: Home visiting by general practitioners in England and Wales. BMJ (Clinical research ed) 313(7051), 207–210 (1996)
van Kempen, J.A., et al.: Home visits for frail older people: a qualitative study on the needs and preferences of frail older people and their informal caregivers. Br. J. Gen. Pract. 62(601), e554–e560 (2012)
Joyce, C.M., Piterman, L.: Trends in GP home visits. Aust. Fam. Physician 37(12), 1039–1042 (2008)
Mueller Y et al.: Home visits made by general practitioners in the canton of Vaud between 2006 and 2015. Swiss Med. Wkly (2019). https://doi.org/10.4414/smw.2019.20037
van den Berg, M.J., et al.: Changing patterns of home visiting in general practice: an analysis of electronic medical records. BMC Fam. Pract. 7(1), 58 (2006)
Soh, L.L., Low, L.L.: Attitudes, perceptions and practice patterns of primary care practitioners towards house calls. J. Prim. Health Care 10(3), 237–247 (2018)
Danish Department of Health and Elderly (2018) En læge tæt på dig - En plan for fremtidens almen praksis, D.D.o.H.a. Elderly, Editor Copenhagen. Danish Department of Health and Elderly.
OECD, Primary Care in Denmark: OECD reviews of health systems. OECD Publishing, Paris (2017)
Forde I et al Primary care review of Denmark. 2016.
The Danish ministry of health, KL—local government Denmark, and The Danish regions, nationale mål for sundhedsvæsenet [The National healthcare quality programme]. 2017.
KL—local government Denmark Læger tager sjældnere på sygebesøg hos ældre [Physicians make fewer home visits related to illness at elderly patients]. 2017.
PLO, Redegørelse for forhandlingsaftalen af 14. september 2017 mellem RLTN og PLO. 2017.
Danish Department of Health and Elderly, Flere plejehjem får fast tilknytteted læger (several nursing homes get permanently attached doctors). 2017: https://www.sum.dk/Aktuelt/Nyheder/Aeldre/2017/Marts/Flere-plejehjem-faar-fast-tilknyttede-laeger.aspx.
Vass, M., et al.: Preventive home visits to older people in Denmark. Z. Gerontol. Geriatr. 40(4), 209–216 (2007)
Newbury, J., Marley, J.: Preventive home visits to elderly people in the community. Visits are most useful for people aged >/= 75. BMJ (Clinical Research ed.) 321(7259), 512–513 (2000)
Statens Serum Institut, Tidlig og hård influenzasæson 2016/17 (Early and severe flu season 2016/17). 2017: https://www.ssi.dk/aktuelt/nyheder/2017/2017-6-epinyt-24-influenza#:~:text=Influenzas%C3%A6sonen%202016%2F17%20var%20pr%C3%A6get,h%C3%A5rdt%20ud%20over%20de%20%C3%A6ldre.
Nørøxe, K.B., et al.: Mental well-being and job satisfaction among general practitioners: a nationwide cross-sectional survey in Denmark. BMC Fam Pract 19(1), 130 (2018)
Li, J., et al.: Physician response to pay-for-performance: evdience from a natural experiment. Health Econ. 23(8), 962–978 (2014)
Ornstein, K.A., et al.: Epidemiology of the homebound population in the United States. JAMA Intern. Med. 175(7), 1180–1186 (2015)
Negrón-Blanco, L., et al.: Prevalence of and factors associated with homebound status among adults in urban and rural Spanish populations. BMC Public Health 16(1), 574 (2016)
Musich, S., et al.: Homebound older adults: prevalence, characteristics, health care utilization and quality of care. Geriatr. Nurs. 36(6), 445–450 (2015)
Krasnik, A., et al.: Changing remuneration systems: effects on activity in general practice. BMJ 300(6741), 1698–1701 (1990)
Acknowledgements
We are grateful to the Novo Nordisk Foundation (Grant number: NNF18OC0033978) and the European Union’s Framework Programme for Research and Innovation Horizon 2020 (Grant number: 721402) for financial support. We also wish to thank Nicolai Fink Simonsen for help with constructing the data set and Luigi Siciliani, Pedro Pita Barros, Nils Gutacker, Karsten Vrangbæk, and Mauro Laudicella for useful comments and feedback. Any remaining errors are the authors’ responsibility.
Funding
This work was supported by the Novo Nordisk Foundation (Grant number: NNF18OC0033978) and the European Union’s Framework Programme for Research and Innovation Horizon 2020 (Grant number: 721402).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
We have no conflicts of interests to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
O’Halloran, J., Oxholm, A.S., Pedersen, L.B. et al. Home sweet home: GPs’ response to an increase in the fee size for home visits. Eur J Health Econ 22, 977–989 (2021). https://doi.org/10.1007/s10198-021-01302-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10198-021-01302-3