
Abstract
Background
Previous studies have not fully determined whether online education materials on chronic kidney disease (CKD) for Japanese patients are easy to understand and help change their behavior. Therefore, this study quantitatively assessed the understandability and actionability of online CKD education materials.
Methods
In September 2021, we searched Google and Yahoo Japan using the keywords “kidney,” “kidney disease,” “CKD,” “chronic kidney disease,” and “renal failure” to identify 538 webpages. We used the Japanese version of the Patient Education Materials Assessment Tool (PEMAT), ranging from 0 to 100%, to evaluate the understandability and actionability of webpages. We set the cutoff point to 70%.
Results
Of the 186 materials included, the overall understandability and actionability were 61.5% (± 16.3%) and 38.7% (± 30.6%), respectively. The materials were highly technical in their terminology and lacked clear and concise charts and illustrations to encourage action. Compared to lifestyle modification materials on CKD overview, symptoms/signs, examination, and treatment scored significantly lower on the PEMAT. In addition, the materials produced by medical institutions and academic organizations scored significantly lower than those produced by for-profit companies.
Conclusion
Medical institutions and academic organizations are encouraged to use plain language and to attach explanations of medical terms when preparing materials for patients. They are also expected to improve visual aids to promote healthy behaviors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chronic kidney disease (CKD) is a growing epidemic, with 697.5 million persons worldwide experiencing kidney damage in 2017 [1]. In Japan, the number of adult patients with CKD is estimated to be 13.3 million, which means that one in eight people have CKD [2]. Studies have reported cardiovascular events, progression to end-stage renal disease, and early death as health risks for patients [3, 4]. Therefore, patients need to be able to detect CKD early and receive appropriate treatment through health checkups and follow-ups at medical institutions. To make this possible, the general public and patients must learn about CKD and its management [5,6,7].
However, several challenges are associated with health communication in patients with CKD. First, CKD is not well known to the public. A survey conducted in 2019 among the general public in Japan found that only 50.7% answered that they knew about CKD [8]. Second, many patients are unaware of their condition because CKD is asymptomatic until the advanced stage. In the National Health Survey conducted between 1999 and 2008, up to 90% of participants with 2–4 markers of CKD were unaware of the disease [9]. Third, inadequate health literacy is a concern for patient education in CKD, with 22.7% of patients with CKD reportedly having limited health literacy [10].
Previous studies have recognized that patient education is a necessary component of CKD care, with evidence that education increases patient knowledge, self-management, and activation across CKD stages [11, 12]. Approximately 70% of the Chronic Renal Insufficiency Cohort (CRIC) study participants reported using the Internet, email, and smartphones [13]. In addition, previous studies have shown that patients who collect health information online tend to make decisions based on it [14, 15].
Regarding CKD educational materials, an RCT in patients with advanced CKD showed that materials might support treatment selection [16]. However, it is questionable whether CKD educational materials can promote better health behaviors in the general public. Previous research using the Suitability Assessment of Materials (SAM) to analyze the CKD web materials found a need to improve message content, visuals/graphics, and layout/design [17]. In addition to assessing whether the material is suitable, The U.S. National Action Plan on Health Literacy lists the need to develop “actionable” health information as a key goal [18]. The Patient Education Materials Assessment Tool (PEMAT) systematically examines how the required action points are presented. The PEMAT was developed by experts under the direction of the Agency for Healthcare Research and Quality (AHRQ) and demonstrated content validity, internal consistency, and reliability [19]. A content analysis of online materials on CKD lifestyle modification using PEMAT reported that the “actionability” of the materials and the method of presenting visual aids need to be improved [20]. However, whether online CKD education materials in Japan help them understand and change patients’ behavior has not been fully discovered. In addition, the attributes and characteristics of “actionable” materials and the issues related to each topic of the materials have not been sufficiently examined. Therefore, using the PEMAT, this study aims to evaluate whether existing webpages with CKD educational materials are easy for patients and the general public to understand and encourage them to take action.
Materials and methods
Study design
This study used quantitative content analysis to review online CKD information systematically.
Inclusion and exclusion criteria
We extensively searched for CKD education materials on September 30, 2021. The search involved obtaining patient educational materials distributed in clinical practice. Japanese websites providing educational information on CKD were included. The exclusion criteria were: (1) webpages aimed at medical professionals, (2) webpages containing misinformation, (3) patient experience, (4) webpages that are irrelevant (e.g., CKD in pets), (5) news or press releases, and (6) webpages not containing educational information. We selected materials from reliable sources that healthcare professionals would generally recommend. During the screening of the webpages, a board-certified nephrologist (EF) reviewed the information for reliability.
Search strategy
We used a Japanese-language search string input into Google Japan and Yahoo Japan, which accounted for approximately 76% and 19% of all Internet searches in August 2021 [21]. We used Google Trends [22] to find the top five most frequently searched words related to CKD. The keywords “kidney,” “kidney disease,” “renal failure,” “CKD,” and “chronic kidney disease,” all of which were in Japanese, were entered into the search window, one keyword at a time. Because previous search engine analysis showed that 10–17% of users browse beyond the first three pages of the results [23], we reviewed 50 webpages per search engine for each term. To ensure comprehensiveness, we added online resources widely used in clinical practice. We performed an online search without an institutional login to avoid retrieving webpages that could only be seen with institutional credentials. To minimize bias in the search results, we logged out of our personal Google and Yahoo accounts and cleared our search history. We did not access content beyond the hyperlinks on the webpage under analysis.
Variables extracted
EF classified the content as follows: (1) overview of CKD, (2) signs and symptoms, (3) screening and testing, (4) treatment options (e.g., medication and renal replacement therapies), and (5) lifestyle modification (e.g., healthy diet and exercise). We also classified the material upload sources into one of the following categories: (1) medical institutions, (2) academic institutions, (3) for-profit companies, (4) governmental organizations, and (5) non-profit organizations. We divided the target audience into two groups: (1) patients and their families and (2) the general public. The classifications were based on previous content analyses of online health resources [24, 25].
Evaluation criteria
Understandability and actionability
The understandability and actionability of the material were rated using the Japanese version of the Patient Education Material Evaluation Tool for Printed Materials (PEMAT-P). PEMAT is intended for use by healthcare professionals, health librarians, and other professionals who provide health and medical information to patients and the general public [19, 26, 27]. As with the original PEMAT [19], the Japanese version of the PEMAT-P has been tested for reliability and validity [28]. In particular, it has proven predictive validity, which means that the assessment results are predictive of understandability and actionability for the audience. This instrument includes 23 items (16 on understandability and 7 on actionability) which were rated using a binary scale (agree = 1 or disagree = 0). We calculated the PEMAT-P scores by taking the sum of the points, dividing it by the total possible points, and multiplying the result by 100 to obtain a percentage. The author of the original version of PEMAT established the threshold for scores empirically at 70%[19]. Previous studies analyzing materials using PEMAT have followed this threshold [20, 29]. This study set the threshold of 70% to be considered understandable or actionable as well as to enable comparison of results with studies conducted in other countries.
Quality (natural flow and comprehensiveness)
The quality of each webpage was assessed using the Global Quality Score (GQS). GQS is used to assess the instructive aspects of online health resources for patients[30], which allows users to evaluate online health resources’ natural flow and comprehensiveness on a five-point Likert scale [31] (Supplementary file 1). It has been commonly used to evaluate health and medical information websites[32,33,34].
Readability
Since both PEMAT and GQS are subjective indicators, we additionally used readability, an objective measure to evaluate textual information. The text from each webpage was pasted to Microsoft Word (Microsoft Corp), and any formatting elements that might interfere with readability assessment (headings, symbols, author information, and references) were removed. The text was then assessed using jReadability [35]. This tool calculates readability based on the average length of sentences, difficulty level of words, proportion of grammatical parts of speech, and types of characters per sentence.
Statistical analysis
We used descriptive statistics to summarize the characteristics and scores of the webpages. For PEMAT-P and jReadability, we performed a one-way analysis of variance (ANOVA) when comparing topics and sources. When significant differences were found, we performed Tukey’s multiple comparison test. For comparisons by the audience, we used an unpaired t-test. If there was a significant difference, we performed Kruskal–Wallis multiple comparisons, and we corrected p-values using the Benjamini–Hochberg method. For the GQS, we used the Kruskal–Wallis rank sum test when comparing topics and sources. If significant differences were found, we performed Kruskal–Wallis multiple comparisons. We corrected p-values using the Benjamini–Hochberg method. Two physicians (EF and YN) calculated inter-rater reliability (Gwet’s AC1) for a quarter of the webpages, since previous studies that analyzed the content of healthcare information usually analyzed inter-rater reliability by having two raters score the information. The two raters had a 60-min meeting in advance to review the PEMAT and GQS evaluation methods; for the PEMAT, User’s Guide [27] was used to provide details and examples of each item. A scale for inter-rater reliability ranges from poor to almost perfect. The scale is as follows: 0.00 to 0.20; Slight, 0.21 to 0.40; Fair, 0.41 to 0.60; Moderate, 0.61 to 0.80; Substantial, and 0.81 to 1.00; Almost Perfect [36].
P-values were two-sided, and p < 0.05 was considered statistically significant. All analyses were conducted using R version 4.0.3 (2020-10-10).
Results
Webpage selection
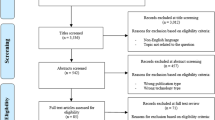
Of the 537 webpages retrieved, we included 186 in the final analysis (Fig. 1). The webpage characteristics are summarized in Table 1. There was a substantial inter-rater agreement for PEMAT-P and GQS (average Gwet's AC1: 0.76 for PEMAT, 0.70 for GQS) (Supplementary file 2).

Selection of the webpages
Understandability and actionability
The mean understandability of these webpages was 61.5 (SD 16.3), and 57 (40%) webpages were acceptable for understanding. The highest understandability achieved was 100, and the lowest was 18. The mean actionability was 38.7 (SD 30.6), and 40 (21.5%) webpages were acceptable for actionability. The highest actionability achieved was 100, and the lowest was 0. Table 2 shows the results of the PEMAT-P ratings. Most webpages (n = 159, 88%) did not have a summary of the key points. In addition, many (n = 138, 74%) had difficulty using only common, everyday language and did not explain medical terms. Most webpages (n = 141, 76%) stated that the audience took at least one action. However, several webpages (n = 144, 77%) lacked visual aids to encourage the audience to take action.
When comparing by topic, the ANOVA revealed the main effect of group assignment [F (4, 181) = 12.47, p < 0.001, η2 = 0.21]. Tukey’s multiple comparison test showed that the materials on lifestyle modification scored significantly higher in both understandability and actionability than those on symptoms and treatment options (lifestyle modification vs. signs and symptoms: M = 77.6 vs. M = 20.4, p = 0.03; lifestyle modification vs. treatment options: M = 77.6 vs. M = 31.2, p < 0.001) (Table 3). A comparison of each PEMAT-P item score showed that the material on lifestyle modification scored the highest for almost all items. Multiple comparisons of the PEMAT-P items showed that on most of the actionability items, materials on lifestyle modification had higher mean scores than those on an overview of CKD, signs and symptoms, and treatment options (Supplementary files 3 and 7).
The materials created by medical institutions and academic organizations scored lower in understandability than those created by for-profit companies. For actionability, there was no significant difference between any of the sources [F (4, 181) = 1.42, p < 0.001, η2 = 0.03] (Table 3). However, multiple comparisons of PEMAT-P items showed that for-profit companies scored higher than governmental agencies on item 25, that is, “The material uses visual aids whenever they could make it easier to act on the instructions” (for-profit companies vs. governmental agencies: M = 0.32 vs. M = 0, p = 0.02) (Supplementary files 4 and 7).
Regarding the audience, there were no significant differences in understandability and actionability (Table 3).
Quality
The mean GQS was 4.2 (SD 0.9). Regarding topics, the ANOVA revealed the main effect of group assignment [F (4, 181) = 4.90, p < 0.001, η2 = 0.098]. Webpages on lifestyle modification were more comprehensive and flowed more naturally than those on CKD overview (lifestyle modification vs. CKD overview: M = 4.67 vs. M = 3.98, p = 0.002). Regarding the source, ANOVA revealed the main effect of group assignment [F (4, 181) = 6.69, p < 0.001, η2 = 0.128]. Webpages created by governmental agencies scored lower than those created by for-profit companies or medical institutions (for-profit companies vs. governmental agencies: M = 4.47 vs. M = 3.63, p = 0.002; medical institutions vs. governmental agencies: M = 4.39 vs. M = 3.63, p = 0.004). When compared by audience (patients and their families vs. the general public = 4.28 vs. 4.08, p = 0.08), the GQS did not differ between categories (Supplementary files 5 and 7).
Readability analysis
The mean jReadability score was 2.2 (SD 0.7). This score indicates that the materials can be understood by those who comprehend technical texts and literary works. When compared by topic, the ANOVA revealed a main effect of group assignment [F (4, 181) = 3.02, p = 0.019, η2 = 0.062]. The readability scores tended to be higher for webpages focused on lifestyle modification (lifestyle modification vs. overview of CKD: M = 2.63 vs. M = 2.16, p = 0.012; lifestyle modification vs. treatment options: M = 2.63 vs. M = 2.09, p = 0.041). When compared by source, ANOVA revealed the main effect of group assignment [F (4, 181) = 2.59, p = 0.038, η2 = 0.054]. Although there were no differences in Tukey’s HSD, the materials produced by for-profit companies tended to score higher than those produced by medical institutions (for-profit companies vs. medical institutions: M = 2.38 vs. M = 2.08, p = 0.11). There was no difference in scores by audience (patients and their families vs. the general public = 2.27 vs. 2.24, p = 0.80) (Supplementary file 6).
Discussion
Characteristics of overall webpages
One of the key results of our study was the lack of understandable and actionable CKD information online. The webpages had an average understandability and actionability of 61.5% and 38.7%, respectively; approximately 60% and 80% of the materials were not understandable and actionable, respectively. Since inadequate engagement in self-management has been well-documented in CKD [37, 38], the scarcity of materials to support health behaviors makes it challenging for CKD patients.
Similar to previous studies, we found that actionability scores were lower than understandability scores [20, 39,40,41]. For understandability, the webpages contained several medical terms, and although visual aids were attached, the majority were unclear and simple. In addition, for actionability, a few webpages utilized visual aids to encourage the general public to take action. One study reported that the materials needed to focus on improving the actionability of the advice given and the way the visual aids were presented [20]. Our study reveals that the same issues exist in Japanese webpages.
Comparison of webpages by categories
The webpages on lifestyle modification were more understandable and actionable than those on signs/symptoms and treatment. Regarding quality and readability, materials on lifestyle modification scored higher than those on the other themes. These materials used fewer medical terms and effectively employed illustrations of desirable lifestyle (e.g., appropriate food intake). A study has reported that patient-centered content is associated with higher-quality materials [17]. However, similar to a previous study [25], these results showed that most websites presented a brief overview of CKD with little information about delaying disease progression. To make more actionable materials for the general public, we recommend webpage authors present not only an overview but also detailed and specific information on CKD. Additionally, webpages must use checklists and flowcharts for topics other than lifestyle modification to assist patients in seeking medical attention and following up at medical facilities.
Regarding understandability, actionability, comprehensiveness, and the natural flow of information, materials created by commercial companies scored higher than those produced by medical institutions and academic organizations. Specifically, commercial companies (mainly pharmaceutical companies) ensured that the materials’ purpose was clearly understood, did not include extra information, and made good use of visual aids. The PEMAT-P showed that medical and academic institutions used medical terminology more frequently and without definitions.
Although previous studies which analyzed English-language materials showed that materials created by public institutions were of higher quality and readability, our study showed contrasting results [41,42,43]. In Japan, the lack of enforceable guidelines for public and professional institutions, such as the Plain Language Act of 2010 [44], might be a factor affecting the results. Institutional guidelines to improve and standardize the understandability and actionability of health-related materials in Japan must be further developed. The Japanese version of the PEMAT, currently the only reliable and validated indicator for measuring the quality of health information in Japan, has the potential to improve this situation. In addition to developing guidelines, individual healthcare organizations should utilize the expertise of commercial companies to create materials for educating patients about CKD.
Strengths and limitations
This study has several limitations. First, since this study only focused on Japanese webpages, the generalizability of the results is lacking. Second, the analysis did not include materials that were unavailable on the Internet. Third, the materials were not verified for compliance with evidence-based practice guidelines; however, a board-certified nephrologist checked the contents for any misinformation. Third, for PEMAT-P and GQS, two raters evaluated and calculated IRRs, but we could not completely rule out rating bias. In addition, patient education materials need to be provided by healthcare providers on a regular and ongoing basis, not just at a single point in time. Furthermore, revisions of guidelines and advances in treatment options may change the behavior recommendations of the materials. We, therefore, consider that a longitudinal analysis of the material is critical as part of future studies. Lastly, although prior studies have shown that the PEMAT has been verified for predictive validity through surveys of the general public [19, 28], the items of the PEMAT do not fully reflect the patient’s perspective. Therefore, the opinions of the audience should be evaluated elsewhere. Future research is needed to qualitatively assess how the audience feel about the materials, or how they are likely to take actions recommended in the materials. Despite these limitations, to our knowledge, this study is the first quantitative content analysis of CKD materials widely used in Japan and has important implications. Shared Decision Making (SDM) is not yet well established in clinical practice in Japan. Patients often hesitate to discuss questions or concerns with healthcare professionals during clinical visits. We believe that patient education materials can help bridge the gap between patients and healthcare professionals by providing knowledge and information to patients and facilitating better communication with healthcare professionals. Therefore, understanding the challenges of these materials is essential to improving the quality of care for patients with CKD.
Conclusion
Although the Internet is a popular source of health information for the general public, we found that CKD information available online was neither understandable nor actionable. They lacked clear, simple visual aids designed to encourage patients to take action. Professional organizations provide poorer quality CKD information with lower actionability than for-profit companies. Furthermore, there is a need to generalize the expertise of commercial companies in preparing information and developing guidelines for communicating health and medical information in an understandable and actionable manner.
References
Bikbov B, Purcell CA, Levey AS, Smith M, Abdoli A, Abebe M, et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet. 2020;395(10225):709–33. https://doi.org/10.1016/s0140-6736(20)30045-3.
Japanese Society of Nephrology. Evidence-based Clinical Practice Guideline for CKD. Japanese Society of Nephrology. 2018. https://cdn.jsn.or.jp/data/CKD2018.pdf. Accessed 19 July 2021.
Go AS, Chertow GM, Fan D, McCulloch CE, Hsu C-Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–305. https://doi.org/10.1056/nejmoa041031.
Van Der Velde M, Matsushita K, Coresh J, Astor BC, Woodward M, Levey AS, et al. Lower estimated glomerular filtration rate and higher albuminuria are associated with all-cause and cardiovascular mortality: a collaborative meta-analysis of high-risk population cohorts. Kidney Int. 2011;79(12):1341–52. https://doi.org/10.1038/ki.2010.536.
Costantini L, Beanlands H, McCay E, Cattran D, Hladunewich M, Francis D. The self-management experience of people with mild to moderate chronic kidney disease. Nephrol Nurs J. 2008;35(2):147–55.
Levey AS, Stevens LA, Coresh J. Conceptual model of CKD: applications and implications. Am J Kidney Dis. 2009;53(3):S4–16. https://doi.org/10.1053/j.ajkd.2008.07.048.
Zhu LX, Ho SC, Wong TK. Effectiveness of health education programs on exercise behavior among patients with heart disease: a systematic review and meta-analysis. J Evid Based Med. 2013;6(4):265–301. https://doi.org/10.1111/jebm.12063.
Japan Kidney Association. Japan Kidney Association and Kyowa Kirin conduct survey on awareness of chronic kidney disease (CKD). Japan Kidney Association 2020. https://j-ka.or.jp/newsinfo/2020/02/-ckd.php. Accessed 24 Feb 2022.
Tuot DS, Plantinga LC, Hsu CY, Jordan R, Burrows NR, Hedgeman E, et al. Chronic kidney disease awareness among individuals with clinical markers of kidney dysfunction. Clin J Am Soc Nephrol. 2011;6(8):1838–44. https://doi.org/10.2215/CJN.00730111.
Fraser SD, Roderick PJ, Casey M, Taal MW, Yuen HM, Nutbeam D. Prevalence and associations of limited health literacy in chronic kidney disease: a systematic review. Nephrol Dial Transpl. 2013;28(1):129–37. https://doi.org/10.1093/ndt/gfs371.
Narva AS, Norton JM, Boulware LE. Educating patients about CKD: the path to self-management and patient-centered care. Clin J Am Soc Nephrol. 2016;11(4):694–703. https://doi.org/10.2215/CJN.07680715.
Stacey D, Legare F, Lewis K, Barry MJ, Bennett CL, Eden KB, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017;4:CD001431. https://doi.org/10.1002/14651858.CD001431.pub5.
Schrauben SJ, Appel L, Rivera E, Lora CM, Lash JP, Chen J, et al. Mobile health (mHealth) technology: assessment of availability, acceptability, and use in CKD. Am J Kidney Dis. 2021;77(6):941-50.e1. https://doi.org/10.1053/j.ajkd.2020.10.013.
Chen YY, Li CM, Liang JC, Tsai CC. Health information obtained from the internet and changes in medical decision making: questionnaire development and cross-sectional survey. J Med Internet Res. 2018;20(2):e47. https://doi.org/10.2196/jmir.9370.
Delli K, Livas C, Spijkervet FK, Vissink A. Internet information on xerostomia: what should patients expect? Oral Dis. 2015;21(1):83–9. https://doi.org/10.1111/odi.12213.
Subramanian L, Zhao J, Zee J, Knaus M, Fagerlin A, Perry E, et al. Use of a decision aid for patients considering peritoneal dialysis and in-center hemodialysis: a randomized controlled trial. Am J Kidney Dis. 2019. https://doi.org/10.1053/j.ajkd.2019.01.030.
Tuot DS, Davis E, Velasquez A, Banerjee T, Powe NR. Assessment of printed patient-educational materials for chronic kidney disease. Am J Nephrol. 2013;38(3):184–94. https://doi.org/10.1159/000354314.
National Action Plan to Improve Health Literacy. U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion.2010. https://health.gov/our-work/national-health-initiatives/health-literacy/national-action-plan-improve-health-literacy. Accessed 23 March, 2022
Shoemaker SJ, Wolf MS, Brach C. Development of the Patient Education Materials Assessment Tool (PEMAT): a new measure of understandability and actionability for print and audiovisual patient information. Patient Educ Couns. 2014;96(3):395–403. https://doi.org/10.1016/j.pec.2014.05.027.
Morony S, McCaffery KJ, Kirkendall S, Jansen J, Webster AC. Health literacy demand of printed lifestyle patient information materials aimed at people with chronic kidney disease: are materials easy to understand and act on and do they use meaningful visual aids? J Health Commun. 2017;22(2):163–70. https://doi.org/10.1080/10810730.2016.1258744.
Search Engine Market Share Japan _ StatCounter Global Stats https://gs.statcounter.com/search-engine-market-share/all/japan/#monthly-201904-201908-bar. Accessed 15 September, 2021.
Google Trend. @GoogleTrends. 2021. https://trends.google.co.jp/trends/?geo=JP. Accessed 15 September, 2021.
Jansen BJ, Spink A. How are we searching the World Wide Web? A comparison of nine search engine transaction logs. Inf Process Manag. 2006;42(1):248–63. https://doi.org/10.1016/j.ipm.2004.10.007.
Misra AR, Oermann MH, Teague MS, Ledbetter LS. An evaluation of websites offering caregiver education for tracheostomy and home mechanical ventilation. J Pediatr Nurs. 2020;56:64–9. https://doi.org/10.1016/j.pedn.2020.09.014.
Lutz E, Costello K, Jo M, Gilet C, Hawley J, Bridgman J, et al. A systematic evaluation of websites offering information on chronic kidney disease. Nephrol Nurs J. 2014;41:355–63.
The Patient Education Materials Assessment Tool (PEMAT) and User’s Guide. 2014. https://www.ahrq.gov/health-literacy/patient-education/pemat.html. Accessed 1 May, 2023
Furukawa E, Okuhara T, Okada H, Shirabe R, Yokota R, Iye R et al. User’s Guide of the Japanese version of PEMAT. 2022. https://plaza.umin.ac.jp/pemat/file/PEMAT_JAPAM_MANUAL.pdf. Accessed 1 May, 2023
Furukawa E, Okuhara T, Okada H, Shirabe R, Yokota R, Iye R, et al. Translation, cross-cultural adaptation, and validation of the Japanese version of the patient education materials assessment tool (PEMAT). Int J Environ Res Public Health. 2022;19(23):15763.
Lambert K. Designing dietary education materials for people with chronic kidney disease: recommendations for improving the quality of resources. J Ren Nutr. 2023;33(1):208–13. https://doi.org/10.1053/j.jrn.2022.06.005.
Bernard A, Langille M, Hughes S, Rose C, Leddin D, van Zanten SV. A systematic review of patient inflammatory bowel disease information resources on the World Wide Web. Am J Gastroenterol. 2007;102(9):2070–7. https://doi.org/10.1111/j.1572-0241.2007.01325.x.
Bernard S, Cooke T, Cole T, Hachani L, Bernard J. Quality and readability of online information about type 2 diabetes and nutrition. JAAPA. 2018;31(11):41–4. https://doi.org/10.1097/01.JAA.0000546481.02560.4e.
Li M, Yan S, Yang D, Li B, Cui W. YouTube™ as a source of information on food poisoning. BMC Public Health. 2019. https://doi.org/10.1186/s12889-019-7297-9.
Chen Z, Pan S, Zuo S. TikTok and YouTube as sources of information on anal fissure: a comparative analysis. Front Public Health. 2022;10:1000338. https://doi.org/10.3389/fpubh.2022.1000338.
Jung MJ, Seo MS. Assessment of reliability and information quality of YouTube videos about root canal treatment after 2016. BMC Oral Health. 2022;22(1):494. https://doi.org/10.1186/s12903-022-02540-4.
jReadability Portal. https://jreadability.net/. Accessed 10 October, 2021.
Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–74.
Ricardo AC, Anderson CA, Yang W, Zhang X, Fischer MJ, Dember LM, et al. Healthy lifestyle and risk of kidney disease progression, atherosclerotic events, and death in CKD: findings from the Chronic Renal Insufficiency Cohort (CRIC) Study. Am J Kidney Dis. 2015;65(3):412–24. https://doi.org/10.1053/j.ajkd.2014.09.016.
Muntner P, Judd SE, Gao L, Gutiérrez OM, Rizk DV, McClellan W, et al. Cardiovascular risk factors in CKD associate with both ESRD and mortality. J Am Soc Nephrol. 2013;24(7):1159–65. https://doi.org/10.1681/asn.2012070642.
Parker PD, Prabhu AV, Su LJ, Zorn KK, Greene CJ, Hadden KB, et al. What’s in between the lines: assessing the readability, understandability, and actionability in breast cancer survivorship print materials. J Cancer Educ. 2021. https://doi.org/10.1007/s13187-021-02003-4.
Lee KS, Cho YM, Oh SH, Jung MS, Yoon JY. Evaluation of the heart failure in internet patient information: descriptive survey study. Int J Environ Res Public Health. 2021;18(3):1047. https://doi.org/10.3390/ijerph18031047.
Ab Hamid MR, Mohd Isamudin M, Baderol Allam FN, Buhari SS. Understandability and actionability of web-based education materials on hypertension management. Environ-Behav Proc J. 2020;5(14):127–33. https://doi.org/10.21834/ebpj.v5i14.2230.
Cajita MI, Rodney T, Jingzhi X, Hladek M, Hae-Ra H. Quality and health literacy demand of online heart failure information. J Cardiovasc Nurs. 2017;32(2):156–64. https://doi.org/10.1097/JCN.0000000000000324.
Pearson K, Ngo S, Ekpo E, Sarraju A, Baird G, Knowles J, et al. Online patient education materials related to lipoprotein(a): readability assessment. J Med Internet Res. 2022;24(1):e31284. https://doi.org/10.2196/31284.
Federal Plain Language Guidelines. PlainLanguage.gov. 2011. https://www.plainlanguage.gov/media/FederalPLGuidelines.pdf. Accessed 12 12 2022.
Funding
Open access funding provided by The University of Tokyo. This research was funded by the Japan Society for the Promotion of Science KAKENHI, grant number 20K10397.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors have declared that there is no conflict of interest.
Ethical approval
This article does not contain any studies with human participants performed by authors. This study was exempted from the Research Ethics Committee of The University of Tokyo Graduate School of Medicine and Faculty of Medicine because the educational material on the website is publicly accessible and does not involve patient records.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Furukawa, E., Okuhara, T., Okada, H. et al. Evaluating the understandability and actionability of online CKD educational materials. Clin Exp Nephrol 28, 31–39 (2024). https://doi.org/10.1007/s10157-023-02401-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-023-02401-6