
Abstract
Background
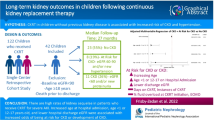
Acute kidney injury (AKI) is commonly seen in the PICU and is associated with poor short-term and long-term outcomes, especially in patients who required continuous kidney replacement therapy (CKRT). However, as the trajectory of kidney recovery in these patients remain uncertain, determination of the timing to convert to permanent kidney replacement therapy (KRT) remains a major challenge. We aimed to examine the frequency and timing of kidney recovery in pediatric AKI survivors that required CKRT.
Methods
We performed a retrospective study of patients under 18 years old who received CKRT for AKI in a tertiary-care PICU over 6 years. Primary outcomes were the rate of KRT withdrawal due to kidney recovery and KRT-dependent days for those who survived to hospital discharge. Secondary outcomes were all-cause mortality, dialysis dependence, and occurrences of estimated glomerular filtration rate (eGFR) < 90 mL/min/1.73m2 and eGFR < 60 mL/min/1.73m2 one year after initiation of the index CKRT in survivors.
Results
Thirty-nine patients were included. Of the 28 children who survived to hospital discharge, 26 (93%) withdrew from dialysis due to kidney recovery, all within 30 days. Twenty-three patients were followed up. One had died, five had an eGFR of 60 mL/min/1.73m2 or more but less than 90 mL/min/1.73m2, and two had an eGFR < 60 mL/min/1.73m2, of which one required peritoneal dialysis.
Conclusions
Over 90% of the survivors withdrew CKRT within 30 days. However, the frequency of abnormal eGFR one year after initiation of CKRT in survivors exceeded 30% and supports the recommendation of post-AKI follow-up.




Similar content being viewed by others


Availability of data and material
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
References
Jetton JG, Boohaker LJ, Sethi SK, et al. Incidence and outcomes of neonatal acute kidney injury (AWAKEN): a multicentre, multinational, observational cohort study. Lancet Child Adolesc Health. 2017;1:184–94.
Kataria Y. Epidemiology of acute kidney injury in critically ill children and young adults. Ann Clin Biochem. 2017;54:416.
Sutherland SM, Ji J, Sheikhi FH, et al. AKI in hospitalized children: epidemiology and clinical associations in a national cohort. Clin J Am Soc Nephrol. 2013;8:1661–9.
Hayes LW, Oster RA, Tofil NM, et al. Outcomes of critically ill children requiring continuous renal replacement therapy. J Crit Care. 2009;24:394–400.
Symons JM, Chua AN, Somers MJ, et al. Demographic characteristics of pediatric continuous renal replacement therapy: a report of the prospective pediatric continuous renal replacement therapy registry. Clin J Am Soc Nephrol. 2007;2:732–8.
Kari JA, Alhasan KA, Shalaby MA, et al. Outcome of pediatric acute kidney injury: a multicenter prospective cohort study. Pediatr Nephrol. 2018;33:335–40.
Alkandari O, Eddington KA, Hyder A, et al. Acute kidney injury is an independent risk factor for pediatric intensive care unit mortality, longer length of stay and prolonged mechanical ventilation in critically ill children: a two-center retrospective cohort study. Crit Care. 2011;15:R146.
Hessey E, Morissette G, Lacroix J, et al. Long-term mortality after acute kidney injury in the pediatric ICU. Hosp Pediatr. 2018;8:260–8.
Mammen C, Al Abbas A, Skippen P, et al. Long-term risk of CKD in children surviving episodes of acute kidney injury in the intensive care unit: a prospective cohort study. Am J Kidney Dis. 2012;59:523–30.
Greenberg JH, Coca S, Parikh CR. Long-term risk of chronic kidney disease and mortality in children after acute kidney injury: a systematic review. BMC Nephrol. 2014;15:184.
Robinson CH, Jeyakumar N, Luo B, et al. Long-term kidney outcomes following dialysis-treated childhood acute kidney injury: a population-based cohort study. J Am Soc Nephrol. 2021;32:2005–19.
Riley AA, Watson M, Smith C, et al. Pediatric continuous renal replacement therapy: have practice changes changed outcomes? A large single-center ten-year retrospective evaluation. BMC Nephrol. 2018;19:268.
Leteurtre S, Duhamel A, Salleron J, et al. PELOD-2: an update of the PEdiatric logistic organ dysfunction score. Crit Care Med. 2013;41:1761–73.
KDIGO CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3:1–150.
Uemura O, Honda M, Matsuyama T, et al. Is the new Schwartz equation derived from serum creatinine and body length suitable for evaluation of renal function in Japanese children? Eur J Pediatr. 2012;171:1401–4.
Nagai T, Uemura O, Ishikura K, et al. Creatinine-based equations to estimate glomerular filtration rate in Japanese children aged between 2 and 11 years old with chronic kidney disease. Clin Exp Nephrol. 2013;17:877–81.
Uemura O, Ishikura K, Gotoh Y, et al. Creatinine-based estimated glomerular filtration rate for children younger than 2 years. Clin Exp Nephrol. 2018;22:483–4.
Goldstein B, Giroir B, Randolph A, et al. International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med. 2005;6:2–8.
von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg. 2014;12:1495–9.
Cortina G, McRae R, Hoq M, et al. Mortality of critically Ill children requiring continuous renal replacement therapy: effect of fluid overload, underlying disease, and timing of initiation. Pediatr Crit Care Med. 2019;20:314–22.
Buccione E, Guzzi F, Colosimo D, et al. continuous renal replacement therapy in critically Ill children in the pediatric intensive care unit: a retrospective analysis of real-life prescriptions, complications, and outcomes. Front Pediatr. 2021;9: 696798.
Uchino S, Kellum JA, Bellomo R, Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators, et al. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294:813–8.
Bagshaw SM, Laupland KB, Doig CJ, et al. Prognosis for long-term survival and renal recovery in critically ill patients with severe acute renal failure: a population-based study. Crit Care. 2005;9:R700–9.
Bell M, Granath F, et al. Continuous renal replacement therapy is associated with less chronic renal failure than intermittent haemodialysis after acute renal failure. Intensive Care Med. 2007;33:773–80.
Thakar CV, Christianson A, Himmelfarb J, et al. Acute kidney injury episodes and chronic kidney disease risk in diabetes mellitus. Clin J Am Soc Nephrol. 2011;6:2567–72.
De Corte W, Dhondt A, Vanholder R, et al. Long-term outcome in ICU patients with acute kidney injury treated with renal replacement therapy: a prospective cohort study. Crit Care. 2016;20:256.
RENAL Replacement Therapy Study Investigators, Bellomo R, Cass A, et al. Intensity of continuous renal-replacement therapy in critically ill patients. N Engl J Med. 2009;361:1627–38.
Nisula S, Kaukonen KM, Vaara ST, et al. Incidence, risk factors and 90-day mortality of patients with acute kidney injury in Finnish intensive care units: the FINNAKI study. Intensive Care Med. 2013;39:420–8.
Bagshaw SM, Mortis G, Doig CJ, et al. One-year mortality in critically ill patients by severity of kidney dysfunction: a population-based assessment. Am J Kidney Dis. 2006;48:402–9.
Ahlström A, Tallgren M, Peltonen S, et al. Survival and quality of life of patients requiring acute renal replacement therapy. Intensive Care Med. 2005;31:1222–8.
Korkeila M, Ruokonen E, Takala J. Costs of care, long-term prognosis and quality of life in patients requiring renal replacement therapy during intensive care. Intensive Care Med. 2000;26:1824–31.
Van Berendoncks AM, Elseviers MM, Lins RL, et al. Outcome of acute kidney injury with different treatment options: long-term follow-up. Clin J Am Soc Nephrol. 2010;5:1755–62.
Schiffl H. Renal recovery from acute tubular necrosis requiring renal replacement therapy: a prospective study in critically ill patients. Nephrol Dial Transplant. 2006;21:1248–52.
Silver SA, Goldstein SL, Harel Z, et al. Ambulatory care after acute kidney injury: an opportunity to improve patient outcomes. Can J Kidney Health Dis. 2015;2:36.
Harel Z, Wald R, Bargman JM, et al. Nephrologist follow-up improves all-cause mortality of severe acute kidney injury survivors. Kidney Int. 2013;83:901–8.
Author information
Authors and Affiliations
Contributions
KT drafted and revised the initial manuscript; NT, KN, JN, YS, and SN critically revised the manuscript for important intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
All the authors have declared no competing interest.
Human and animal rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee at which the studies were conducted (IRB approval number 2021–187) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Patient consent for publication
Need for consent from individual patients was waived by the Institutional Review Board.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
About this article

Cite this article
Tsuboi, K., Tsuboi, N., Nishi, K. et al. Trajectory of kidney recovery in pediatric patients requiring continuous kidney replacement therapy for acute kidney injury. Clin Exp Nephrol 26, 1130–1136 (2022). https://doi.org/10.1007/s10157-022-02246-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-022-02246-5