
Abstract
Background
Programmed death-ligand 1 (PD-L1) positivity is associated with poor prognosis in renal cell carcinoma (RCC). Because the prognostic impact and effect of confounding factors are less known, we investigated the prognostic significance of PD-L1 expression in Japanese patients with recurrent/metastatic RCC who started systemic therapy in 2010–2015.
Methods
This multicenter, retrospective study recruited patients from 29 Japanese study sites who had prior systemic therapy for RCC (November 2018 to April 2019) and stored formalin-fixed paraffin-embedded primary lesion samples. The primary outcome was overall survival (OS) by PD-L1 expression. Secondary outcomes included OS in subgroups and duration of first- and second-line therapies by PD-L1 expression. OS distributions were estimated using Kaplan–Meier methodology.
Results
PD-L1 expression (on immune cells [IC] ≥ 1%) was observed in 315/770 (40.9%) patients. PD-L1 positivity was more prevalent in patients with poor risk per both Memorial Sloan Kettering Cancer Center [MSKCC] and International Metastatic RCC Database Consortium, and high-risk pathological features (higher clinical stage, nuclear grade and sarcomatoid features). Median OS for PD-L1–positive patients was 30.9 months (95% CI 25.5–35.7) versus 37.5 months (95% CI 34.0–42.6) for PD-L1–negative patients (HR 1.04 [90% CI 0.89–1.22, p = 0.65]; stratified by MSKCC risk and liver metastases). Propensity score weight (PSW)-adjusted OS was similar between PD-L1–positive and –negative patients (median 34.4 versus 31.5 months; estimated PSW-adjusted HR 0.986).
Conclusions
This study suggests PD-L1 status was not an independent prognostic factor in recurrent/metastatic RCC during the study period because PD-L1 positivity was associated with poor prognostic factors, especially MSKCC risk status.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Targeted therapies (e.g., vascular endothelial growth factor receptor [VEGFR] tyrosine kinase inhibitors [TKIs] and mammalian target of rapamycin [mTOR] inhibitors) have been the standard of care for renal cell carcinoma (RCC) since 2008 in Japan [1]. Immunotherapies targeting the programmed death 1/programmed death-ligand 1 (PD-[L]1) pathway and anti–cytotoxic T-lymphocyte–associated antigen 4 (CTLA-4) recently remodeled the metastatic RCC (mRCC) treatment landscape. Checkpoint inhibitors (CPIs) have demonstrated promising efficacies in the first-line (1L) setting in combination with anti–CTLA-4 or VEGFR TKIs [2,3,4].
PD-L1 is an established biomarker for antitumor T-cell response in other cancers but not in mRCC [5]. Although better outcomes were noted in PD-L1–positive populations, anti-tumor effects were also observed in PD-L1–negative populations compared with controls[2,3,4]. Thus, routine PD-L1 testing is not standard for treating mRCC with CPIs. The prognostic role of PD-L1 expression in RCC has been investigated in several studies. High PD-L1 expression (on tumor cells [TC] or tumor-infiltrating immune cells [IC]) correlated with shorter overall survival (OS) and worse prognostic features (high nuclear grade, sarcomatoid differentiation, higher T stage, and poor International Metastatic RCC Database Consortium [IMDC] risk status) [6,7,8,9]. Hence, PD-L1 expression was recently recognized as a negative prognostic factor in RCC [10].
Several patient characteristics can affect clinical outcomes in RCC. Two-year survival rates (per IMDC risk classification) were unsatisfactory for patients with poor risk mRCC (7% versus 75% and 53% [favorable and intermediate]) [11]. Poor outcomes have also been reported for patients with mRCC and sarcomatoid components [12]. Tumor immune phenotype is another potential prognostic biomarker; prognosis for clear cell RCC worsens with cluster of differentiation 8–positive (CD8 +) T-cell infiltration into tumor tissue and checkpoint molecule expression [13].
PD-L1 expression may not only be a predictive biomarker for CPI treatment, but also a negative prognostic marker in RCC. Thus, clarifying the mechanism behind its potential prognostic significance is important in understanding RCC biology. In this multicenter, retrospective study, we investigated the prognostic significance of PD-L1 expression on OS in a large cohort of Japanese patients treated with systemic therapy for recurrent/metastatic RCC before CPIs became the standard of care for 1L treatment. We also explored whether PD-L1 would remain an independent prognostic factor after adjusting for baseline characteristics, which would increase its clinical significance.
Materials and methods
Patients
Samples were collected between November 2018 and June 2019 from 29 Japanese study sites that provided guideline-based, standard-of-care treatment. Patients aged ≥ 20 years underwent nephrectomy, had stored formalin-fixed paraffin-embedded (FFPE) surgical samples of the primary lesion, and started systemic therapy for recurrent/metastatic RCC between January 2010 and December 2015. Since long-term storage of paraffin blocks generally does not significantly impact immunohistochemistry, there was no limitation on the sample collection time of FFPE surgical samples [14]. Exclusion criteria were coexisting malignancies (from nephrectomy to death) or first-line (1L) treatment with anti–CTLA-4/anti–PD-(L)1 for recurrent/metastatic RCC. Patients with tumor tissue samples were recruited and informed consent was obtained. This study is registered under UMIN (UMIN000034131) and was performed after approval by each institutional review board (IRB) of the 29 study sites. Approval from the IRB of MINS, a non-profit organization, was also obtained.
More details on patients can be found in the supplementary methods in the Online Resource.
Study design and outcomes
This multicenter, retrospective study compared OS by PD-L1 expression status to determine its prognostic effect. The primary outcome was OS, which is defined as the time from initiation of 1L therapy to death from any cause, according to PD-L1 status (positive versus negative). Secondary outcomes included OS in subgroups by PD-L1 status, expression level (four IC levels), and duration of 1L and second-line (2L) therapy by PD-L1 status.
Pathology and immunohistochemistry
Representative FFPE samples were selected by pathologists in each institution and evaluated by a central pathologist. Samples had to be of good quality and had to have an adequate number of tumor cells for PD-L1 evaluation. Pathological assessments were conducted to determine the histologic type such as Fuhrman grade (1–4), World Health Organization (WHO)/International Society of Urologic Pathologists (ISUP) grade (1–4), tumor necrosis, lymphovascular infiltration, sarcomatoid component, and growth pattern [15, 16].
All samples were sent to the central laboratory (SRL, Inc.) for hematoxylin and eosin staining and immunohistochemistry staining using standardized protocols. PD-L1 expression was evaluated independently by two central pathologists by immunohistochemistry using the VENTANA SP142 assay (Ventana Medical Systems, Inc., 740–4859). Based on IC expression levels, patients were classified as either PD-L1 negative (IC0; IC < 1%), or PD-L1 positive (IC1 [IC: ≥ 1% but < 5%], IC2 [IC: ≥ 5% but < 10%] or IC3 [IC ≥ 10%]).
Immune phenotype assessment was performed using CD8 immunostaining [17]. Based on three characterizations of T-cell activity from tumor biopsies, patients were categorized into immune-desert (T-cell absence), immune-excluded (T-cell accumulation but not in tumor core), and immune-inflamed (T-cells infiltration but not functioning) phenotypes [18, 19].
Details on pathology and immunohistochemistry can be found in the Supplementary methods.
Statistical analyses
The full analysis set used for this study included all enrolled patients, except those with indeterminate PD-L1 expression. Based on previous reports and clinical significance, a median OS of 26 months for the PD-L1–negative group and 20 months for the PD-L1–positive group was assumed, leading to a hypothesized true HR of 1.3 for this study [4, 6]. When 80% power is guaranteed at a significance level of 10%, two-sided, the required number of events would be 359. To ensure the required number of events, and accounting for specimens with indeterminate PD-L1 status as well as dropouts due to consent withdrawal, enrollment of approximately 600 patients was planned. nQuery Advisor 7.0 (Statistical Solutions Ltd, Ireland) was used to calculate the number of events.
OS distributions were estimated using the Kaplan–Meier (KM) method, and CI of the median was estimated using the Brookmeyer-Crowley technique [20]. The superiority hypothesis was tested with a two-sided significance level of 10% using log-rank test, stratified by MSKCC risk criteria (favorable, intermediate, or poor) and liver metastases. These stratification factors were selected based on expected substantial effects on OS and a previous clinical trial, which evaluated PD-L1 status by SP142, considering the non-randomized nature of this study [2]. Stratified HRs and their 90% CIs were estimated using the stratified Cox regression model (PD-L1 positive: test arm; PD-L1 negative: control arm). Unstratified and subgroup analyses were also performed. In addition, propensity score weight (PSW) analysis was conducted to evaluate the robustness of the primary analysis [21]. A logistic regression model was used to predict the score for each patient, defined as the probability of being PD-L1 positive (explanatory variables in Supplementary Tables S2, S3). After confirming sufficient overlap in propensity score distribution, matching weights method was applied [22].
Results
Clinicopathological characteristics by PD-L1 status at initial diagnosis and nephrectomy
Of 777 samples collected, seven samples were not PD-L1–evaluable. Hence, only 770 patients were recruited (PD-L1 positive: 315; PD-L1 negative: 455). Characteristics between groups were generally balanced for sex, histological type, lymphovascular invasion, and growth pattern (Table 1). Fewer patients in the PD-L1–positive group had undergone radical nephrectomy than in the PD-L1–negative group (38.1% versus 57.4%).
Immune phenotype (CD8-infiltration type) composition differed between PD-L1–positive (excluded: 74.3%; inflamed: 16.5%; desert: 9.2%) and PD-L1–negative groups (excluded: 31.6%; inflamed: 1.5%; desert: 66.8%; Table 1). Furthermore, PD-L1 positivity was numerically higher in patients with higher clinical stage, higher nuclear grade (WHO/ISUP grade and Fuhrman grade), and sarcomatoid disease. The two groups were imbalanced in sample collection year; PD-L1 positivity was lower in older samples.
Clinical characteristics by PD-L1 status at the time of 1L therapy
PD-L1 positivity was similar based on age and metastatic site, including liver metastases (Table 1). A higher proportion of PD-L1–positive than –negative patients had poor prognostic features at 1L therapy: poor MSKCC risk, 17.5% versus 7.3%; poor IMDC risk, 29.2% versus 14.9%. Fewer PD-L1–positive patients had the following good prognostic features at 1L therapy: favorable MSKCC risk, 11.4% versus 29.7%; favorable IMDC risk, 10.8% versus 26.2%.
Systemic therapy for metastatic/recurrent RCC
Sunitinib (VEGFR TKI) was the most common 1L therapy for PD-L1–positive and –negative groups (51.7 and 53.4%; Table 2). Second-line therapies were received by 70.8% of PD-L1–positive and 75.6% of –negative patients. Axitinib (VEGFR TKI) was the most common 2L therapy (28.3 and 34.3%). Third-line therapy was received by 39.0% of PD-L1–positive and 44.8% of –negative patients (Table 2). Everolimus (mTOR inhibitor) was the most common third-line therapy (11.1 and 13.8%), and nivolumab was the only CPI received (5.1 and 7.0%). Fourth-line therapies were received by 15.9% of PD-L1–positive and 23.3% of –negative patients.
OS by PD-L1 expression (stratified log-rank test)
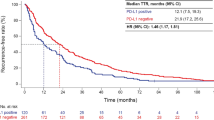
Median OS in PD-L1–positive and –negative patients was 30.9 (95% CI 25.5–35.7) and 37.5 (95% CI 34.0–42.6) months, respectively (stratified HR = 1.04 [90% CI 0.89–1.22, p = 0.65], unstratified HR 1.21 [90% CI 1.04–1.40]; Fig. 1). No statistically significant difference in OS distribution was observed; thus, the primary analysis suggested that PD-L1 status alone had no prognostic significance on outcomes in RCC.

KM curves of OS by PD-L1 status. CI confidence interval; HR hazard ratio; KM Kaplan–Meier; mo months; OS overall survival; PD-L1 programmed death-ligand 1
OS by PD-L1 expression (PSW–adjusted analysis)
Sufficient overlap was observed in the distribution of estimated propensity scores. Histograms of pre- and post-PSW-adjusted distributions for PD-L1–positive and –negative groups are shown in Supplementary Fig. S1. No significant difference in PSW-adjusted OS was observed between the two groups, supporting the interpretation of the stratified analysis (Fig. 2). Median PSW-adjusted OS in the PD-L1–positive and –negative groups were 34.4 and 31.5 months, respectively (estimated PSW-adjusted HR 0.99). Additionally, HR stratified by propensity score per quartile was 1.045. Data pertaining to PSW analysis are shown in Supplementary Tables S4 and S5.

KM curves of PSW-adjusted OS. HR hazard ratio; KM Kaplan–Meier; mo months; OS overall survival; PD-L1 programmed death-ligand 1; PSW propensity score-weighted
OS by PD-L1 expression in subgroups
In subgroups based on MSKCC risk at 1L therapy, there was no significant difference in OS distribution based on PD-L1–positive or –negative status for favorable (median 58.6 versus 59.8 months; unstratified HR 0.92; 95% CI 0.54–1.56), intermediate (median 31.6 versus 33.5; HR 1.06; 95% CI 0.85–1.32) or poor (median 6.6 versus 12.8; unstratified HR 0.89; 95% CI 0.55–1.43) categories (Figs. 3 and 4). Subgroup analysis of OS by liver metastases status at the time of 1L therapy showed a trend towards shorter OS for PD-L1–positive versus PD-L1–negative patients (median OS for absent: 31.6 versus 40.2 months; unstratified HR 1.24; 95% CI 1.02–1.50, present: 9.0 versus 25.3; unstratified HR 1.27; 95% CI 0.72–2.23; Fig. 3, Supplementary Fig. S2). Results from other subgroups (based on nuclear grade, IMDC risk criteria, or immune phenotype; Fig. 3, Supplementary Fig. S3–S7) are also reported.

Forest plot of OS by PD-L1 status and patient subgroups. CI confidence interval; FAS full analysis set; HR hazard ratio; IMDC International Metastatic RCC Database Consortium; mo months; MSKCC Memorial Sloan Kettering Cancer Center; OS overall survival; PD-L1 programmed death-ligand 1; WHO/ISUP World Health Organization/International Society of Urologic Pathologists


KM curves of OS by PD-L1 status in subgroups after treatment. Subgroups were MSKCC risk criteria A favorable, B intermediate, and C poor, and patients who D used and E did not use immune checkpoint inhibitor after 2L therapy. 2L second-line; CI confidence interval; HR hazard ratio; KM Kaplan–Meier; mo months; NE not evaluable; OS overall survival; PD-L1 programmed death-ligand 1
OS by CPI treatment and PD-L1 status
Of 559 patients who received ≥ 2L therapy, 108 received nivolumab after 2L therapy (CPI-treated). Median OS observed for PD-L1–positive versus –negative patients in the CPI-treated group was 71.5 versus 69.4 months (unstratified HR 0.61; 95% CI 0.31–1.21) and 27.2 versus 34.0 months (unstratified HR 1.24; 95% CI 1.00–1.55) in the CPI-untreated group. In these two groups, KM curves showed a reverse trend (Fig. 4D, E). The analyses in patients who never received CPI throughout their treatment are shown in Supplementary Fig. S8.
Treatment duration in 1L and 2L settings by PD-L1 status
Treatment duration in the 1L setting was slightly shorter in the PD-L1–positive group than in the PD-L1–negative group (median 5.1 months [95% CI 4.3–5.9] versus 6.0 months [95% CI 5.3–7.0]; unstratified HR 1.102 [95% CI 0.95–1.28]; stratified HR 1.01 [95% CI 0.87–1.17]; Supplementary Fig. S9a).
Treatment duration of 2L therapy was also shorter in the PD-L1–positive group compared with the PD-L1–negative group (median 4.2 months [95% CI 3.4–5.1] versus 5.7 months [95% CI 4.9–6.7]; unstratified HR 1.22 [95% CI 1.03–1.46]; stratified HR 1.17 [95% CI 0.97–1.40]; Supplementary Fig. S9b).
Discussion
Baseline patient characteristics and treatment patterns were similar to those previously reported in a real-world setting in Japan. MSKCC risk status distribution was better than that in the previous report (favorable: 22.2% versus 13.2%; intermediate: 66.4% versus 68.1%; poor: 11.4% versus 18.7%) [23].
The proportion of PD-L1–positive patients (40.9%) is within the range reported previously (40–54%) [2, 24]. A higher prevalence of PD-L1 positivity was observed in patients with poor prognostic features (i.e., poor MSKCC/IMDC risk) and high-risk pathological features (higher clinical stage, higher nuclear grade, and sarcomatoid features). These observations are consistent with other reports in patients with high nuclear grade, sarcomatoid component, or high IMDC risk status; patients with clear cell RCC and poor risk status were more likely to express PD-L1 on TC than those with intermediate or favorable status (poor: 43%; intermediate: 29%; favorable: 17%; in METEOR study [NCT01865747]) [8, 9, 25]. PD-L1–positive patients showed more CD8-infiltrated phenotype than PD-L1–negative patients, which aligns with studies describing the correlation of IC status with T-effector gene signature [24].
Median OS after 1L treatment was 6 months shorter in the PD-L1–positive than in the –negative group, consistent with previous studies [9]. However, no statistically significant difference in OS distribution was observed between PD-L1–positive and –negative groups when stratified by MSKCC risk and liver metastases. The robustness of this primary analysis was supported by PSW–adjusted analysis. Additionally, in subgroups based on MSKCC risk, OS distributions were very similar for PD-L1–positive and –negative patients and were similarly shortened depending on risk status (Fig. 4a–c). This result aligns with those from the multivariable logistic regression model used to estimate the propensity score, which showed the highest odds ratio with MSKCC risk status, meaning it had the most relevant clinical covariates with PD-L1 expression (Supplementary Tables S2 and S3). MSKCC risk status distribution in PD-L1–positive patients was biased towards a poorer prognosis than in PD-L1–negative patients, suggesting that the OS difference between PD-L1–positive and –negative populations was mainly caused by difference of MSKCC risk status distribution. Therefore, PD-L1 status of primary lesion may not have clinical value when MSKCC/IMDC risk assessment is performed in recurrent/metastatic RCC in the era before CPIs became the standard of care for 1L treatment.
The role of PD-L1 expression as a biomarker for CPI response in RCC is not yet established due to its biological complexity (intra/inter patient-heterogeneity and dynamic nature of the marker). Recent studies and a meta-analysis found significantly improved OS and progression-free survival in CPI-treated PD-L1–positive patients [2, 3, 26]. In this study, OS was longer in PD-L1–positive patients who received ≥ 2L CPI therapy versus PD-L1–negative patients; the results were reversed in CPI-untreated patients.
New findings in the subgroup analysis by pathological features were observed. Previous studies have shown that low nuclear grades and low CD8 + T-cell infiltration are associated with better outcomes in RCC [13, 27]. This study found a trend towards shorter OS in PD-L1–positive patients with lower Fuhrman grades (e.g., Grade 2; median OS: 44.3 versus 55.1 months; unstratified HR 1.35 [95% CI 0.90–2.01]) and immune desert phenotype (median OS: 19.8 versus 37.1 months; unstratified HR 1.53 [95% CI 0.96–2.42]). Interestingly, this observation was not seen in the WHO/ISUP Grade 2 population (Supplementary Fig. S3a and S4a). Nonetheless, this finding suggests that prognosis worsens for patients with RCC if PD-L1–positive ICs infiltrate the tumor, even if other pathological characteristics were favorable. However, among patients with an inflamed phenotype and in subgroups with higher pathological grade, PD-L1–positive patients had similar OS compared with PD-L1-negative patients. These results suggest that a comprehensive examination of PD-L1 (IC) status, malignancy, and CD8 infiltration in surgical specimens may be needed when predicting prognosis.
Due to the retrospective nature of the study, unmeasured confounding factors could have had an effect. This study was based on mRCC after nephrectomy, which is representative of patients with RCC in the real world who have undergone nephrectomy but excludes those who have not. Because central pathologists only reviewed selected representative slides, some pathological features could have been underdiagnosed. Before 2009, the proportion of PD-L1–negative samples was greater than PD-L1–positive ones; however, the trend reversed between 2013 and 2015. A recent study found a strong correlation between high PD-L1 expression and tumor grade in non-small cell lung cancer [28]. In this study, PD-L1 positivity was higher in patients with high-risk pathological features (higher clinical stage, higher nuclear grade, and sarcomatoid features; Table 1), and the proportion of patients in Stage I/II was higher during the earlier collection period (Supplementary Table S6). Thus, the difference in PD-L1 positivity across sample collection years was likely to be a result of uneven clinical stage distribution rather than sample storage duration.
These results are clinically relevant in understanding the prognostic value of PD-L1 expression on recurrent/metastatic RCC before CPIs became the standard of care for 1L treatment. Overall, this retrospective study was the first to investigate potential associations between clinical outcomes and PD-L1 status in patients with previously treated RCC. Despite the retrospective nature of this study, our results suggest that PD-L1 status is not an independent prognostic factor in recurrent/metastatic RCC because, PD-L1 positivity was associated with other prognostic factors, especially MSKCC risk status.
Change history
27 August 2021
A Correction to this paper has been published: https://doi.org/10.1007/s10147-021-02008-5
References
Yoshimura K, Uemura H (2016) Pharmacotherapies for renal cell carcinoma in Japan. Int J Urol 23(3):194–202. https://doi.org/10.1111/iju.13008
Rini BI, Powles T, Atkins MB et al (2019) Atezolizumab plus bevacizumab versus sunitinib in patients with previously untreated metastatic renal cell carcinoma (IMmotion151): a multicentre, open-label, phase 3, randomised controlled trial. Lancet 393(10189):2404–2415. https://doi.org/10.1016/S0140-6736(19)30723-8
Rini BI, Plimack ER, Stus V et al (2019) Pembrolizumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Eng J Med 380(12):1116–1127
Motzer RJ, Tannir NM, McDermott DF et al (2018) Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N Engl J Med 378(14):1277–1290. https://doi.org/10.1056/NEJMoa1712126
Gong J, Chehrazi-Raffle A, Reddi S et al (2018) Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration trials and future considerations. J Immunother Cancer 6(1):8-018-0316-z. https://doi.org/10.1186/s40425-018-0316-z
Iacovelli R, Nolè F, Verri E et al (2016) Prognostic role of PD-L1 expression in renal cell carcinoma. A systematic review and meta-analysis. Target Oncol 11(2):143–148. https://doi.org/10.1007/s11523-015-0392-7
Carlsson J, Sundqvist P, Kosuta V et al (2020) PD-L1 expression is associated with poor prognosis in renal cell carcinoma. Appl Immunohistochem Mol Morphol 28:213–220
Joseph RW, Millis SZ, Carballido EM et al (2015) PD-1 and PD-L1 expression in renal cell carcinoma with sarcomatoid differentiation. Cancer Immunol Res 3(12):1303–1307. https://doi.org/10.1158/2326-6066.CIR-15-0150
Flaifel A, Xie W, Braun DA et al (2019) PD-L1 expression and clinical outcomes to cabozantinib, everolimus, and sunitinib in patients with metastatic renal cell carcinoma: analysis of the randomized clinical trials METEOR and CABOSUN. Clin Cancer Res 25(20):6080–6088. https://doi.org/10.1158/1078-0432.CCR-19-1135
Kammerer-Jacquet S-F, Deleuze A, Saout J et al (2019) Targeting the PD-1/PD-L1 pathway in renal cell carcinoma. Int J Mol Sci 20(7):1692
Heng DY, Xie W, Regan MM et al (2009) Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: results from a large, multicenter study. J Clin Oncol 27(34):5794–5799. https://doi.org/10.1200/JCO.2008.21.4809
Golshayan AR, George S, Heng DY et al (2009) Metastatic sarcomatoid renal cell carcinoma treated with vascular endothelial growth factor-targeted therapy. J Clin Oncol 27(2):235–241. https://doi.org/10.1200/JCO.2008.18.0000
Giraldo NA, Becht E, Pagès F et al (2015) Orchestration and prognostic significance of immune checkpoints in the microenvironment of primary and metastatic renal cell cancer. Clin Cancer Res 21(13):3031–3040. https://doi.org/10.1158/1078-0432.CCR-14-2926
Bass BP, Engel KB, Greytak SR et al (2014) A review of preanalytical factors affecting molecular, protein, and morphological analysis of formalin-fixed, paraffin-embedded (FFPE) tissue: how well do you know your FFPE specimen? Arch Pathol Lab Med 138(11):1520–1530. https://doi.org/10.5858/arpa.2013-0691-RA
Nishikimi T, Tsuzuki T, Fujita T et al (2011) The post-operative pathological prognostic parameters of clear cell renal cell carcinoma in pT1a cases. Pathol Int 61(3):116–121. https://doi.org/10.1111/j.1440-1827.2010.02633.x
Delahunt B, Eble JN, Egevad L et al (2019) Grading of renal cell carcinoma. Histopathology 74(1):4–17. https://doi.org/10.1111/his.13735
Mariathasan S, Turley SJ, Nickles D et al (2018) TGFβ attenuates tumour response to PD-L1 blockade by contributing to exclusion of T cells. Nature 554(7693):544–548. https://doi.org/10.1038/nature25501
Mariathasan S, Turley SJ, Nickles D et al (2017) 8O_PR TGF-β signalling attenuates tumour response to PD-L1 checkpoint blockade by contributing to retention of T cells in the peritumoural stroma. Ann Oncol 28(suppl_11):mdx760.001
Binnewies M, Roberts EW, Kersten K et al (2018) Understanding the tumor immune microenvironment (TIME) for effective therapy. Nat med 24(5):541–550. https://doi.org/10.1038/s41591-018-0014-x
Brookmeyer R, Crowley J (1982) A confidence interval for the median survival time. Biometrics 38:29–41
Rosenbaum P (1983) The central role of the propensity score in observational studies for causal effects. Biometrika 70:41–55
Li L, Greene T (2013) A weighting analogue to pair matching in propensity score analysis. Int J Biostat 9(2):215–234. https://doi.org/10.1515/ijb-2012-0030
Harada K, Nozawa M, Uemura M et al (2019) Treatment patterns and outcomes in patients with unresectable or metastatic renal cell carcinoma in Japan. Int J Urol 26(2):202–210. https://doi.org/10.1111/iju.13830
McDermott DF, Huseni MA, Atkins MB et al (2018) Clinical activity and molecular correlates of response to atezolizumab alone or in combination with bevacizumab versus sunitinib in renal cell carcinoma. Nat Med 24(6):749–757. https://doi.org/10.1038/s41591-018-0053-3
Thompson RH, Gillett MD, Cheville JC et al (2004) Costimulatory B7–H1 in renal cell carcinoma patients: indicator of tumor aggressiveness and potential therapeutic target. Proc Natl Acad Sci USA 101(49):17174–17179
Roviello G, Corona S, Nesi G et al (2019) Results from a meta-analysis of immune checkpoint inhibitors in first-line renal cancer patients: does PD-L1 matter? Ther Adv Med Oncol 11:1758835919861905. https://doi.org/10.1177/1758835919861905
Lang H, Lindner V, de Fromont M et al (2005) Multicenter determination of optimal interobserver agreement using the Fuhrman grading system for renal cell carcinoma: assessment of 241 patients with > 15-year follow-up. Cancer 103(3):625–629. https://doi.org/10.1002/cncr.20812
Kerr KM, Thunnissen E, Dafni U et al (2019) A retrospective cohort study of PD-L1 prevalence, molecular associations and clinical outcomes in patients with NSCLC: results from the European Thoracic Oncology Platform (ETOP) Lungscape project. Lung Cancer 131:95–103. https://doi.org/10.1016/j.lungcan.2019.03.012
Acknowledgements
The authors would like to thank the patients who participated in the trial, their families, as well as the investigators and staff at all participating centers (Supplementary Table S1). Ohe Chisato, MD (Department of Pathology and Laboratory Medicine, Kansai Medical University, Japan) contributed to this study by assessing PD-L1 expression of samples. This study was funded by Chugai Pharmaceuticals Co. Ltd. Third-party writing assistance for this manuscript was provided by Bena Lim, PhD, of Health Interactions, and supported by Chugai Pharmaceuticals Co. Ltd.
Funding
This study was funded by Chugai Pharmaceuticals Co. Ltd.
Author information
Authors and Affiliations
Contributions
Conceptualization: TT, NM, TF, and HU; Data acquisition: MU, NN, NS, KT, KH, and TY; Data analysis: MO, NS, HU, and TT; Funding acquisition: TF; Statistical analysis: TY, and YN; Writing–draft: MU, NM, TF, and HU; Writing–review and editing: All authors; Supervision: HU.
Corresponding author
Ethics declarations
Conflict of interest
Fukuyama T, Nakagawa Y, and Yoshimoto T are employees of Chugai Pharmaceutical. All honoraria received by the following authors were outside of the submitted work: Uemura H (Pfizer, MSD, Janssen, BMS, Ono Pharmaceutical, Astellas Pharma, and Bayer), Tsuzuki T (Novartis, Chugai Pharmaceutical, AstraZeneca, Janssen, BMS, Ono Pharmaceutical, Nippon Kayaku, Astellas Pharma, Bayer, Takeda, and Daiichi Sankyo), Oya M (Pfizer, Novartis, AstraZeneca, Janssen, BMS, Ono Pharmaceutical, Astellas Pharma, Bayer, Takeda, and Sanofi), Shinohara N (Pfizer, Novartis, Janssen, BMS, Ono Pharmaceutical, Astellas Pharma, Takeda, and Sanofi).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised due to a retrospective Open Access order.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Uemura, M., Nakaigawa, N., Sassa, N. et al. Prognostic value of programmed death-ligand 1 status in Japanese patients with renal cell carcinoma. Int J Clin Oncol 26, 2073–2084 (2021). https://doi.org/10.1007/s10147-021-01993-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10147-021-01993-x