
Abstract
Purpose
To determine the incidence of missed cervical spine injuries by radiology registrars in a major trauma centre and to identify any common blind spots.
Materials and methods
All patients with an acute traumatic injury who underwent a CT scan of the cervical spine in our unit, which serves a population of approximately 900,000, between September 2016 and December 2017 and whom had a separate radiology trainee report and final neuroradiology consultant report available were included in the study. We recorded the date and time of the scan, the registrar error and the registrar grade. An error was defined as follows: (1) a missed fracture; (2) a missed ligamentous injury; (3) overcall of a fracture (e.g. degenerative calcification or nutrient vessel). Groups were compared with the chi-square test.
Results
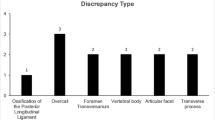
Five hundred seventy-three CT scans of the cervical spine fitted the inclusion criteria and were analysed. There were a total of 149 injuries over eight levels in 96 patients. There were 12 registrar errors (2.1% discrepancy rate), of which 11 were missed acute injuries (9 fractures and 2 disco-ligamentous injuries). The grade of the registrar was not significant (p = 0.603). Seventy-three percent (8/11) missed injuries were disproportionately at the cranio-cervical junction, where only 11.6% of traumatic cervical spine injuries occur p < 0.0001. Forty-five percent of the missed injuries included occipital condyle fractures, which occurred in only 12/149 injuries (8%).
Conclusions
Radiology registrars safely report emergency CT scans of the cervical spine performed following trauma with a low discrepancy rate. Missed cervical spine injuries commonly occur at the cranio-cervical junction, which should become a standard review area.



Similar content being viewed by others


References
McCaughey EJ et al (2016) Changing demographics of spinal cord injury over a 20-year period: a longitudinal population-based study in Scotland. Spinal Cord 54(4):270–276
McDaid D, La Park A, Gall A, Purcell M, Bacon M (2019) Understanding and modelling the economic impact of spinal cord injuries in the United Kingdom. Spinal Cord 57(9):778–788
Cross CE, Kapoor V, Todd B (2012) The litigation burden to the NHS from spinal injuries and surgery: analysis of consecutive closed claims. Orthop Proc 94-B(Supp_XXVI):387
Stiell IG et al (2001) The Canadian C-spine rule for radiography in alert and stable trauma patients. J Am Med Assoc 286(15):1841–1848
National Institute for Health and Care Excellence (NICE) (2016) Spinal injury: assessment and initial management, NICE guidelines SG41. NICE, London
Briggs RH, Rowbotham E, Johnstone AL, Chalmers AG (2010) Provisional reporting of polytrauma CT by on-call radiology registrars. Is it safe? Clin Radiol 65(8):616–622
Fredø HL, Rizvi SA, Lied B, Rønning P, Helseth E (2012) The epidemiology of traumatic cervical spine fractures: a prospective population study from Norway. Scand J Trauma Resusc Emerg Med 20:85
Bruno MA, Walker EA, Abujudeh HH (2015) Understanding and confronting our mistakes: the epidemiology of error in radiology and strategies for error reduction. Radiographics 35(6):1668–1676
Robinson PJ (1997) Radiology’s Achilles’ heel: error and variation in the interpretation of the Röntgen image. Br J Radiol 70(839):1085–1098
Bahrami S, Yim CM (2009) Quality initiatives: blind spots at brain imaging. Radiographics 29(7):1877–1896
Kim YW, Mansfield LT (2014) Fool me twice: delayed diagnoses in radiology with emphasis on perpetuated errors. AJR Am J Roentgenol 202(3):465–470
Anderson PA, Montesano PX (1988) Morphology and treatment of occipital condyle fractures. Spine (Phila Pa 1976) 13(7):731–736
Joaquim AF, Ghizoni E, Tedeschi H (2014) Upper cervical injuries - a rational approach to guide surgical management. J Spinal Cord Med 37(2):139–151
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Werndle, M.C., Myers, J. & Mortimer, A. Missed cervical spine injuries: aim for the top. Emerg Radiol 29, 491–497 (2022). https://doi.org/10.1007/s10140-022-02026-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10140-022-02026-4