
Abstract
Anti-N-methyl-d-aspartate receptor encephalitis (anti-NMDAR encephalitis) is the most common type of immune-mediated encephalitis. This study aimed to assess the incidence and mortality of anti-NMDAR encephalitis in intensive care unit (ICU) to evaluate the clinical manifestations, laboratory findings, managements and outcomes, and to compare these characteristics with patients with non-anti-NMDAR encephalitis admitted to ICU. Patients admitted to the neurological ICU with suspected encephalitis were included between January 1, 2012 and July 31, 2015. Cerebrospinal fluid (CSF) of enrolled patients was screened for anti-NMDAR antibodies using a cell-based assay. 72 critically ill patients with encephalitis of uncertain etiology were investigated, and 16 patients were positive for anti-NMDAR antibodies in CSF. Compared to patients with non-anti-NMDAR encephalitis, patients with anti-NMDAR encephalitis were younger, more likely to present with the psychiatric symptoms, dyskinesia, and autonomic dysfunction, and had longer ICU stays. The abnormal movements were so difficult to control that complicated the management. The outcome was favorable in ten patients 1 year after the disease onset, and the mortality was as high as 25 % overall. The incidence of anti-NMDAR encephalitis is high among critically ill patients with encephalitis of uncertain etiology. Controlling dyskinesia proved to be a challenge. Persistent dysautonomias were additional difficult to manage confounders. Same points being highlighted in this study may aid clinicians in the management of patients with anti-NMDAR encephalitis in intensive care practice.
Similar content being viewed by others

Introduction
Anti-N-methyl d-aspartate receptor (anti-NMDAR) encephalitis, first identified in 2007 by Dalmau et al. [1], has been increasingly identified as an important cause of autoimmune and paraneoplastic encephalitis. This acute autoimmune neurological disorder is characterized by a complex presentation with several stages. The majority of patients present with a prodrome of flu-like symptoms, and typically within 2 weeks, patients rapidly develop schizophrenia-like psychiatric symptoms and seizures. Other symptoms, including orofacial dyskinesias, abnormal movements, speech abnormalities, central hypoventilation, autonomic instability, memory deficits, and cognitive decline may also develop during the course of the disease [2]. The diagnosis is confirmed by detection of autoantibodies against the GluN1 subunit of the NMDAR in the cerebrospinal fluid (CSF) and/or serum. Treatment is focused on first-line immunotherapy and tumor resection, but second-line immunotherapy may be required in nonresponders [3]. The majority of patients enters into a gradual recovery phase, and recovers completely or has mild sequelae, but some patients demonstrate persistent severe disability or even death [3].
Anti-NMDA-R encephalitis could be a differential diagnosis of infectious encephalitis, and the previous intensive care literatures are limited. We therefore analyzed the presence of anti-NMDAR antibodies in CSF samples from patients in the intensive care units (ICU) with encephalitis of unknown etiology. We systemically characterized the clinical presentation, frequency of tumor association, laboratory findings, response to immunotherapy, and outcomes in those encephalitis patients harboring these autoantibodies, and compared with patients without anti-NMDAR antibodies.
Methods
Patients and methods
Patients suspected of having encephalitis of undetermined cause and hospitalized between January 1, 2012, and July 31, 2015 at neurological ICU, Department of Neurology, West China Hospital, were enrolled. The CSF samples of each patient were sent to Peking Union Medical College Hospital, China, for examining the anti-NMDAR antibodies as we previously reported [4]. Antibodies against a-amino-3-hydroxy-5-methyl-4-isoxazol-propionic acid (AMPA) receptors 1 and 2, contact in associated protein 2 (CASPR2), leucine-rich glioma inactivated protein 1 (LGI1) and c-amino-butyric acid receptors (GABAR B1/B2) were also examined. We categorized our patients into two groups: an anti-NMDAR encephalitis group and a non-anti-NMDAR encephalitis group. This study was approved by the Ethical Committee of West China Hospital of Sichuan University. Informed consent was obtained from all individual participants included in the study. Clinical information was obtained by the referring physicians upon admission and every 3 months during the follow-up, including prodromal symptoms, psychiatric symptoms, speech disturbances, seizures, movement disorders, loss of consciousness, autonomic dysfunction, cognitive impairment [2, 3, 5]. Indications for ICU admission, ICU course, and complications were also recorded. All patients underwent extensive diagnostic studies, including brain magnetic resonance imaging (MRI), electroencephalography (EEG), and CSF examinations. The effect and outcome of treatment were assessed using the modified Rankin Scale (mRS) at 4 weeks and every 3 months after the initiation of immunotherapy [6–8].
Statistical analysis
Descriptive statistics were used to determine the characteristics of the clinical features. The comparisons between the two groups were done with the Mann–Whitney U test, and contingency table examinations were evaluated by fisher exact or Chi-square test. SPSS version 18.0 (SPSS Inc, Chicago, IL) was used for all analyses, and p < 0.05 was considered to indicate statistical significance, but we acknowledged the unlikelihood of positive p values with a small sample size.
Results
From January 1, 2012, to July 31, 2015, 72 critically ill patients with encephalitis of uncertain etiology were referred to our neurological ICU, and received examination of anti-NMDAR antibodies in CSF, 16 (22.2 %) were positive. Among the 56 patients non-anti-NMDAR encephalitis, 11 patients were found to have a herpes simplex virus type I/II virus antibody IgM, five patients were suspected to have tuberculous meningoencephalitis, two patients were identified to have antibodies against the gamma-aminobutyric acid-B receptor (GABABR), and one patient was proved to have antibodies against the leucine-rich glioma inactivated protein 1 (LGI1), the rest 37 cases were tested to have unknown disease etiology.
Clinical features
There were ten (62.5 %) female and six (37.5 %) male patients who were identified to have anti-NMDAR encephalitis. Two (12.5 %) patient was ≤15 years old, four patients (25 %) were 16–20 years old, five (31.2 %) patients were 21–25 years old, two (12.5 %) patients were 26–30 years old, and three patients were 31–38 (18.8 %) years old.
In the prodromal phase, patients experienced a range of symptoms including headache, and nonspecific infectious-like symptoms of nausea, vomiting, and upper respiratory symptoms. These symptoms that occurred within 2 weeks before admission to ICU were present in 11/16 cases.
The most predominant presentations at admission were seizure, psychiatric or behavioral symptoms, and cognitive dysfunctions. Six patients presented with seizure at onset, among them two patients experienced partial seizures, one patient had partial seizure followed by generalized tonic–clonic seizures (GTCS), and three patients presented with GTCS at onset. Followed the seizures, five patients presented with psychiatric or behavioral symptoms over a median time of 8 days (range 3–15 days), and one patient had a fluctuating level of consciousness 12 days later. Seven patients presented with psychiatric or behavioral symptoms at onset, including agitation and aggressive behavior, mood lability and catatonia, anxiety and emotional disturbances, bizarre behavior paranoia, and psychosis (delusional thinking and auditory or visual hallucinations). Three patients experienced cognitive dysfunctions at onset, including shorter term memory loss and confusion associated with speech disturbances (decreased speech intelligibility, speech reduction, and mutism). Followed these cognitive first symptoms, two patients rapidly moved to hallucinations and psychosis 2 days later, one patient had GTCS 3 days later.
Eleven patients developed movement disorders and dyskinesia after a median time of 12 days (range 8–23 days) of hospitalization, including orofacial twitching, dystonic postures, choreoathetoid movements, rigidity, and a range of eye signs (eye deviation, nystagmus, and ocular dipping). Twelve patients developed autonomic dysfunction, including cardiac dysrhythmias, hyperthermia, hypoventilation, and unstable blood pressure. Four patients had clinically significant hypotension, two patients showed clinically significant bradycardia, and three patients had clinically significant tachycardia. Hyperthermia was a common feature, observed in 11 patients. Seven patients had central hypoventilation. Six patients had marked hypersalivation. Seven patients were also noted to have sleep dysfunction.
Table 1 showed all clinical features when we compared the two groups. Patients with anti-NMDAR encephalitis were significantly younger than patients with non-anti-NMDAR encephalitis. Furthermore, greater percentage of patients with anti-NMDAR encephalitis presented with the psychiatric symptoms, dyskinesia, and autonomic dysfunction.
Indications for ICU admission, and ICU course
Mechanical ventilation, the predominant ICU support was applied to all patients with anti-NMDAR encephalitis, and thirteen of them received tracheostomy. The mean duration of mechanical ventilation was 30 days (range 1–92 days) and the ICU length of stay (LOS) ranged from 6 to 139 days (mean 58 days). The ICU support and course were compared between the anti-NMDAR antibodies-positive and anti-NMDAR antibodies-negative encephalitis cases. The proportion of cases who received tracheostomy was higher in anti-NMDAR antibodies-positive cases than that in the anti-NMDAR antibodies-negative encephalitis cases. For the ICU course, patients with anti-NMDAR encephalitis had longer ICU LOS than patients with non-anti-NMDAR encephalitis (Table 2).
Investigations
Four patients were positive and twelve patients were strongly positive for anti-NMDAR antibodies in CSF. The neuroimaging results were generally normal in six patients. The abnormalities included focal or generalized meningitis changes, increased signal located at unilateral or bilateral temporal lobe on fluid-attenuated inversion recovery or T2 weighted sequences, and bilateral extensive brain atrophy. Although clinical suspicion of seizure activity was found in the majority of patients, only two patients had epileptiform activity in short-term EEG monitoring. Two patients had normal EEG results, and the EEG results of others included predominantly frontotemporal or generalized slow activity. The leukocyte counts, total protein levels, glucose levels in CSF were within the normal physiological range in five patients. Four patients had CSF pleocytosis only, three patients had increased total protein levels only, and four patients had both. The histological-confirmed ovarian teratoma was identified in two female patients. An unusual presentation that mixed malignant mediastinal germ cell tumor (MGCT) (choriocarcinoma + teratoma) was found in a male patient. Table 3 showed the abnormalities of laboratory features when we compared the two groups. The abnormalities of findings in CSF analysis, EEG monitoring, MRI scanning, and tumor frequency were not significantly different between these two groups.
Treatments
The abnormal movements, such as dystonic postures and rigidity, were particularly problematic and difficult to control. In addition, patients commonly exhibited prolonged abnormal behaviors. Antiepileptic drugs (AEDs) were used in all patients. Furthermore, anticonvulsant medicines, neuromuscular blocking agents, antipsychotics, and continuous-infusion sedatives were given to the majority of patients, aiming to limit seizures or abnormal movements. However, these medicines were not effective enough to control the dystonic movements. Patients with significant hypotension all required vasopressor support. One patient experienced episodes of extreme bradycardia and asystole, and repeated periods of cardiopulmonary resuscitation were applied. Of the 16 patients with anti-NMDAR encephalitis, 14 patients received first-line immunotherapy consisting of immunoglobulins and/or corticosteroids, and the time from disease onset to start immunotherapy ranged from 1 to 25 days (median 11.6 days) after being admitted to hospital. Ten patients received combination therapy consisting of immunoglobulins and corticosteroids, and five patients had immunoglobulins alone. The plasma exchanges were performed in one patient. As a second immunomodulatory treatment, cyclophosphamide was given to one patient, and rituximab was given to another patient after failing first-line immunotherapy. The remaining one patient did not receive immunotherapy due to death before the autoantibody results were obtained. Two patients underwent surgical salpingo-oophorectomy, and histopathology showed ovarian mature teratoma. One patient received mediastinal tumor resection, and MGCT was confirmed by the postoperative pathological examination.
Outcomes and relapses
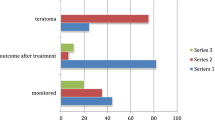
The patients were followed up for vital status to the end of 2015. The follow-up period ranged from 11 to 26 months. The outcome was favorable in ten patients with anti-NMDAR encephalitis 1 year after the disease onset (mRS 0–2), including six patients with complete recovery (mRS 0), and four patients having symptoms of cognitive dysfunctions after 1 year, including anterograde amnesia, emotional lability, and attention deficit (mRS 1–2). Two patients with minimal changes in neurological status were in the rehabilitation center or at home at the time of this report (mRS 3–5). One patient died in the ICU because of multiple organ dysfunction syndromes (MODS). Three patients with severe neurological disability, including loss of consciousness, dysautonomia, and central hypoventilation remained hospitalized for more than 2 months after the onset of symptoms, and they died of infection with respiratory failure after they were discharged from the hospital (mRS 6). One female patient had a fully neurological improvement (mRS 0) after having the teratoma removed, but the male patient with the presence of MGCT died of respiratory failure, even though he undertook tumor resection. Another female patient with teratoma had a neurological relapse in a period of 13 months after the resection. Table 4 showed comparison of the outcomes in the two groups. The outcomes in patients with anti-NMDAR encephalitis were not significantly different from those in patients with non-anti-NMDAR encephalitis.
Discussion
Among 72 critically ill patients with encephalitis of uncertain etiology admitted in the ICU, we identified 16 patients positive for anti-NMDAR encephalitis, representing 22.2 % of patients’ admissions. In one retrospective analysis, 505 patients aged 18–35 years admitted to the ICU were reviewed for criteria of encephalitis of unknown etiology, and six of them (1.2 %) were identified to have NMDAR antibodies [9]. Our study indicated that anti-NMDAR encephalitis was not uncommon, particularly among ICU patients with encephalitis of unknown etiology. Similarly, a study from UK analyzed of an observational cohort study of 31 patients with nonbacterial meningoencephalitis admitted to a tertiary neurological ICU, and identified NMDAR antibodies in six patients (19.3 %) [10]. The great proportion of anti-NMDAR encephalitis in patients with encephalitis in the ICU could be partially explained by the fact that some patients with anti-NMDAR encephalitis experiencing dramatic neuropsychiatric changes required extensive critical care management, and some patients progressed rapidly to severe deterioration of consciousness and central hypoventilation, leading to respiratory failure. In this study, we found that the number of patients who received tracheostomy was much bigger in patients with anti-NMDAR encephalitis group compared to that of the group with non-anti-NMDAR encephalitis, indicating that patients with anti-NMDAR encephalitis frequently required ICU management, and they were more likely to received tracheostomy and probably prolonged ventilator support due to deterioration of respiratory function. The frequent occurrence also called our attention to distinguish anti-NMDAR from key viral entities, because the promote diagnosis would permit more timely treatment, and a more rapid recovery. Study had showed that those patients with anti-NMDAR encephalitis who were treated earlier may be more likely to make complete recoveries [11].
In line with previous studies, anti-NMDAR encephalitis was predominantly found in female patients. Our patients with anti-NMDAR encephalitis were mostly young adults (with a average age of 23.75 years), and they were younger than patients with non-anti-NMDAR encephalitis. A study which enrolled 577 patients with anti-NMDAR encephalitis also reported a median age of 21 years [2]. For young patients admitted to ICU with severe unknown encephalitis, anti-NMDAR encephalitis should be suspected.
The clinical features of the patients in our case series were quite similar to those described in previous studies. It usually presented with viral infection-like symptoms, and 68.75 % patients showed symptoms of prodromal phase. The next phase was seizure and/or psychotic phase, and a total of 14 patients had psychiatric manifestations, which accounted for 87.5 % cases. Greater percentage of patients with anti-NMDAR encephalitis showed the psychiatric or behavioral symptoms, compared to patients with non-anti-NMDAR encephalitis. The first case series of anti-NMDAR encephalitis, which mostly analyzed adult patients, reported that 85 % of the patients initially presented with psychiatric or behavioral symptoms [1]. Prominent and long-term lasting neuropsychiatric symptoms in adults could be identifying characteristics to distinguish patients with anti-NMDAR encephalitis from patients with non-anti-NMDAR encephalitis. Seizures and status epilepticus could develop at early stage or anytime during the course of the disease. In this study, one patient presented with status epilepticus at disease onset, and his persistent seizure was hard to control, leading to ICU admission and intubation. For other six patients, seizures were diagnosed through clinical symptoms; only one patient had epileptiform changes on EEG. However, the first case series observed epileptiform activity in 21 of 92 patients [1]. First, the patients may well have had true seizures that were not captured on EEG. Second, the frequency and intensity of the seizures tended to decrease as the diseases progressed. Third, the difficulty of distinguishing the abnormal movements and epileptic seizures, the overlapping could lead to under-recognition of seizures or improper escalation of antiepileptic medications for dyskinesia, which was considered as a seizure. In this study, 68.75 % patients with anti-NMDAR encephalitis developed movement disorders and dyskinesia, the percentage was much greater than that in patients with non-anti-NMDAR encephalitis. A study also showed that seven/nine patients in ICU with anti-NMDAR encephalitis presented with treatment-refractory movement disorder [12]. These findings indicated that dyskinesia was a common clinical feature among patients with anti-NMDAR encephalitis. The dystonic postures and rigidity for the patients in ICU were difficult to control and so violent that sometimes put the patients at risk for tracheostomy dislodgment. Although many kinds of medications were used, these medicines were not effective enough to limit the dyskinesia. We also noticed that patients with anti-NMDAR encephalitis had longer ICU LOS than patients with non-anti-NMDAR encephalitis, and this phenomenon may be related to the treatment-refractory dyskinesia and autonomic dysfunction, which made the ongoing care difficult. This issue had not been highlighted according to previous studies focusing on patients in the ICU.
The ovarian teratoma was identified in two female patients, and a mixed germ cell tumor (choriocarcinoma & teratoma) was found in a male patient. Previous studies observed the rate of ovarian teratoma in a large study cohort (577 cases) of anti-NMDAR encephalitis, and reported that 38 % of patients had tumors and 94 % of the tumors were ovarian teratoma [2]. Moreover, an underlying ovarian teratoma was detected more often in female patients >18 years [13]. Another case series of 400 patients reported that only 2 % had a tumor other than an ovarian teratoma [3]. In this study, we only found that two of ten (20 %) female patients had ovarian teratoma, one was 19 years old, the other was 18 years old. Similarly, in another case series from China, only three patients had ovarian teratoma out of the 21 female patients (14.3 %) [14]. Three of ten (30 %) female patients in Taiwan [15], and six of 22 (27.3 %) female patients in Korea [7] were identified to have ovarian teratoma. Furthermore, it was reported that black women were more likely to have an underlying ovarian teratoma than patients from other ethnic groups [3]. Combined these findings, we think that the different proportion of concomitant ovarian teratoma in anti-NMDAR encephalitis patients may due to the race-specific factor, perhaps involving the human leucocyte antigen or other genetic factors. After checking the literatures, we found that it was the first report of male patient with MGCT. A case report identified a 16-year-old boy with Klinefelter syndrome had anti-NMDAR encephalitis and a mediastinal mass, and which was pathologically proven to be a teratoma [16]. It was reported that the frequency of paraneoplastic etiology in the male population was low, approximately 3–15 % of cases, including testicular germ cell tumors, small cell lung carcinoma, and Hodgkin lymphoma [1–3, 17].
Conclusions
Anti-NMDAR encephalitis should be suspected in any patients with encephalitis of uncertain etiology, especially in young adult patients who developed prominent psychiatric symptoms, dyskinesia, and autonomic dysfunction. Distinguishing between seizures and dyskinesia and controlling of these symptoms proved to be a challenge. Genetic or racial predisposition was needed to be addressed in future studies. Together, some learning points highlighted in this study may aid clinicians in the management of critically ill patients with anti-NMDAR encephalitis in intensive care practice.
References
Dalmau J, Gleichman AJ, Hughes EG et al (2008) Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies. Lancet Neurol 7:1091–1098
Titulaer MJ, McCracken L, Gabilondo I et al (2013) Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study. Lancet Neurol 12:157–165
Dalmau J, Lancaster E, Martinez-Hernandez E et al (2011) Clinical experience and laboratory investigations in patients with anti-NMDAR encephalitis. Lancet Neurol 10:63–74
Wang W, Li JM, Hu FY et al (2016) Anti-NMDA receptor encephalitis: clinical characteristics, predictors of outcome and the knowledge gap in southwest China. Eur J Neurol 23:621–629
Iizuka T, Sakai F, Ide T et al (2008) Anti-NMDA receptor encephalitis in Japan: long-term outcome without tumor removal. Neurology 70:504–511
Gable MS, Gavali S, Radner A et al (2009) Anti-NMDA receptor encephalitis: report of ten cases and comparison with viral encephalitis. Eur J Clin Microbiol Infect Dis 28:1421–1429
Lim JA, Lee ST, Jung KH et al (2014) Anti-N-methyl-d-aspartate receptor encephalitis in Korea: clinical features, treatment, and outcome. J Clin Neurol 10:157–161
van Swieten JC, Koudstaal PJ, Visser MC et al (1988) Interobserver agreement for the assessment of handicap in stroke patients. Stroke 19:604–607
Pruss H, Dalmau J, Harms L et al (2010) Retrospective analysis of NMDA receptor antibodies in encephalitis of unknown origin. Neurology 75:1735–1739
Davies G, Irani SR, Coltart C et al (2010) Anti-N-methyl-d-aspartate receptor antibodies: a potentially treatable cause of encephalitis in the intensive care unit. Crit Care Med 38:679–682
Luca N, Daengsuwan T, Dalmau J et al (2011) Anti-N-methyl-d-aspartate receptor encephalitis: a newly recognized inflammatory brain disease in children. Arthritis Rheum 63:2516–2522
Young PJ, Baker S, Cavazzoni E et al (2013) A case series of critically ill patients with anti-N-methyl-d-aspartate receptor encephalitis. Crit Care Resusc 15:8–14
Florance NR, Davis RL, Lam C et al (2009) Anti-N-methyl-d-aspartate receptor (NMDAR) encephalitis in children and adolescents. Ann Neurol 66:11–18
Huang X, Fan C, Wu J et al (2015) Clinical analysis on anti-N-methyl-d-aspartate receptor encephalitis cases: Chinese experience. Int J Clin Exp Med 8:18927–18935
Lin JJ, Lin KL, Hsia SH et al (2014) Anti-N-methyl-d-aspartate receptor encephalitis in Taiwan—a comparison between children and adults. Pediatr Neurol 50:574–580
Sommeling C, Santens P (2014) Anti-N-methyl-d-aspartate (anti-NMDA) receptor antibody encephalitis in a male adolescent with a large mediastinal teratoma. J Child Neurol 29:688–690
Irani SR, Bera K, Waters P et al (2010) N-methyl-d-aspartate antibody encephalitis: temporal progression of clinical and paraclinical observations in a predominantly non-paraneoplastic disorder of both sexes. Brain 133:1655–1667
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
All procedures performed in the studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
This study was funded by the National Natural Science Foundation of China (Grant No. 81301093).
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
X. Chen and J.-M. Li equal contributors.
Rights and permissions
About this article

Cite this article
Chen, X., Li, JM., Liu, F. et al. Anti-N-methyl-d-aspartate receptor encephalitis: a common cause of encephalitis in the intensive care unit. Neurol Sci 37, 1993–1998 (2016). https://doi.org/10.1007/s10072-016-2702-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-016-2702-y