
Abstract
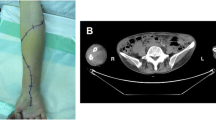
Muscle pain and weakness in a rheumatoid arthritis (RA) patient has a broad differential, and myositis should be considered early in the disease course as serious limb and life-threatening sequelae may occur. A 55-year-old woman with a past medical history of methotrexate-controlled RA presented with right leg pain for 4 days. The patient suffered sensory loss in the right foot and decreased strength in the toes. Lab tests revealed elevated creatine kinase, ESR, and anti-rheumatoid factor antibody titers. CT scan revealed myositis of posterior compartment muscles. Progressive edema, pain, and neuromuscular deficits persisted despite steroid and antibiotic therapy, so the patient was taken for urgent fasciotomy for acute compartment syndrome. The muscle biopsy showed diffuse mononuclear cell infiltration as well as perivascular and perineural involvement consistent with rheumatoid myositis (RM). The patient did well post-op on a prednisone taper. This case underlines the systemic nature of RA and exemplifies the severity of inflammation that may lead to grave consequences such as compartment syndrome. The histopathology is diagnostic when there is evidence of mononuclear cell infiltration; however, this is not entirely specific. Early, aggressive therapy with immunosuppressives is warranted in such patients. RM has not, to our knowledge, been recorded to cause acute compartment syndrome. Clinicians should be aware of this uncommon manifestation of RA keeping the various presentations of rheumatoid disease in mind when faced with these patients.


Similar content being viewed by others


References
Firestein G (2013) Rheumatoid arthritis. In: Firestein GS, Budd RS, Gabriel SE (eds) Kelley’s textbook of rheumatology. Elselvier Saunders, Philadelphia
Halla JT, Koopman WJ, Fallahi S, Oh SJ, Gay RE, Schrohenloher RE (1984) Rheumatoid myositis. Clinical and histologic features and possible pathogenesis. Arthritis Rheum 27(7):737–743
Miro O, Pedrol E, Casademont J, Garcia-Carrasco M, Sanmarti R, Cebrian M et al (1996) Muscle involvement in rheumatoid arthritis: clinicopathological study of 21 symptomatic cases. Semin Arthritis Rheum 25(6):421–428
Haslock DI, Wright V, Harriman DG (1970) Neuromuscular disorders in rheumatoid arthritis. A motor-point muscle biopsy study. Q J Med 39(155):335–358
Brooke MH, Kaplan H (1972) Muscle pathology in rheumatoid arthritis, polymyalgia rheumatica, and polymyositis: a histochemical study. Arch Pathol 94(2):101–118
Ali Z, Ranganathan P, Perry A, Gelbart M (2007) Localized striated muscle vasculitis in rheumatoid arthritis. J Clin Rheumatol Pract Rep Rheum Musculoskelet Dis 13(1):35–37
Chatterjee S, Kupsky WJ (2005) Severe proximal myopathy and mononeuritis multiplex in rheumatoid arthritis: manifestations of rheumatoid vasculitis. J Clin Rheumatol Pract Rep Rheum Musculoskelet Dis 11(1):50–55
Nakamura H, Okada A, Kawakami A, Yamasaki S, Ida H, Masuda T et al (2010) Rheumatoid vasculitis of crural muscles confirmed by muscle biopsy in the absence of inflammatory myopathy: histologic and MRI study. Rheumatol Int 30(10):1381–1383
Kim RC, Collins GH (1981) The neuropathology of rheumatoid disease. Hum Pathol 12(1):5–15
Canale S (2013) Traumatic disorders. In: Canale ST, Beaty JH (eds) Campbell’s operative orthopedics. Elsevier Mosby, Philadelphia, pp 2311–2313
Cone LA, Lamb RB, Graff-Radford A, Rudder J, Bach SA et al (1997) Pyomyositis of the anterior tibial compartment. Clin Infect Dis 25(1):146–148
Disclosures
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Jo, D., Pompa, T., Khalil, A. et al. Rheumatoid myositis leading to acute lower extremity compartment syndrome: a case-based review. Clin Rheumatol 34, 1813–1816 (2015). https://doi.org/10.1007/s10067-014-2657-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-014-2657-4