
Abstract
Purpose
While robotic-assisted hernia repair has increased the popularity of minimally invasive hernia surgery, selecting between the types of approaches is a challenge for both experts and novices alike. In this study, we compared a single surgeon’s early experience transitioning from transabdominal hernia repair with sublay mesh in either the pre-peritoneal or retrorectus space (TA-SM) and enhanced-view totally extra-peritoneal (eTEP) ventral hernia repair in the peri-operative and long-term post-operative time periods.
Methods
We conducted a retrospective review of 50 eTEP and 108 TA-SM procedures to collect demographics, intraoperative details, and 30-day and 1-year post-operative outcomes. Statistical analysis was performed utilizing Chi-square analysis, Fisher’s test, and two sample t-tests with equal variances.
Results
There were no significant differences in patient demographics or comorbidities. eTEP patients had larger defects (109.1 cm2 vs. 31.8 cm2, p = 0.043) and mesh used (432.8 cm2 vs. 137.9 cm2, p = 0.001). Operative times were equivalent (158.3 ± 90.6 min eTEP and 155.8 ± 65.2 min TA-SM, p = 0.84), but conversion to alternate procedure type was higher for the transabdominal approach (4% eTEP vs. 22% TA-SM, p < 0.05). Hospital stay was less in the eTEP cohort (1.3 days vs. 2.2 days, p < 0.05). Within 30 days, there were no significant differences in emergency visits or hospital readmissions. There was a greater propensity for eTEP patients to develop seromas (12.0% vs. 1.9%, p < 0.05). At 1 year, there was no statistically significant difference in recurrence rate (4.56% eTEP vs. 12.2% TA-SM, p = 0.28) respective to average time to recurrence (9.17 months eTEP vs. 11.05 months TA-SM).
Conclusion
The eTEP approach can be adopted safely and efficiently, and may have superior peri-operative outcomes including fewer conversions and reduced hospital stay.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Ventral hernias represent a common surgical problem with a high disease burden. In the United States, over 350,000 ventral hernia repairs are performed annually with cost estimates exceeding $3.4 billion [1, 2]. Additional costs such as lost days of work due to physical impairment and worsened quality of life due to chronic pain are difficult to quantify. While surgical repair is associated with significant improvements in quality of life based on patient satisfaction surveys [3], the type of hernia repair selected may minimize complications and risk of recurrence in a patient with given hernia characteristics.
When it comes to hernia repair, the choices are many and the data are conflicting. A surgeon can choose between open, laparoscopic, and robotic approaches. Minimally invasive techniques for hernia repair can improve peri-operative outcomes; however, post-operative prescription medication use, return to work, and health-related quality-of-life outcomes may not differ substantially [4]. In addition, long-term recurrence rates vary widely depending on other fundamental tenets of hernia repair. For example, a 5% recurrence rate at 2 years after open ventral hernia repair with transversus abdominis release (TAR) has been reported [5, 6], while percentages of recurrence after laparoscopic ventral hernia repair can approach the teens in some cases [7, 8]. The type of mesh used, mesh location and overlap, primary fascial closure, and use of a component separation can all affect outcomes.
Although laparoscopic hernia repair with transabdominal pre-peritoneal mesh (TAPP), TAR, or Rives–Stoppa repair have been described [9,10,11], robotic surgery has become a more favorable minimally invasive approach, particularly for more complex abdominal wall reconstruction and when patients are obese [12]. Increased versatility of robotic instruments and enhanced three-dimensional visualization facilitate the learning curve for an otherwise challenging laparoscopic procedure. Early outcomes of robotic transabdominal retromuscular repair with TAR demonstrate that the procedure is safe and feasible, and has optimal outcomes with fewer systemic complications and a reduced length of stay by over 48 h when compared to open procedures [13, 14]. Preliminary outcomes of robotic enhanced-view totally extra-peritoneal (eTEP) ventral hernia repair are also promising with few post-operative complications and multiple groups reporting a length of stay less than 24 h [15,16,17].
Long-term outcomes for either procedure are not well established. In this study, we aim to investigate the difference in peri-operative, 30-day and long-term post-operative outcomes in patients undergoing robotic transabdominal hernia repair with sublay mesh (TA-SM) and eTEP hernia repair using our early experiences with these approaches.
Methods
After obtaining institutional review board approval, we performed a retrospective analysis of robotic ventral hernia repairs performed in a single surgeon’s early experience with TA-SM (January 2012 to March 2016) and eTEP (April 2018 to August 2019). Our search was based on CPT codes 49650, 49651, 49652, 49653, 49654, 49,655, 49656, and 49657. Electronic medical records were reviewed for patient characteristics and comorbidities according to ACS-NSQIP [18, 19], prior history of hernia repair, intraoperative details (hernia characteristics, operative time, estimated blood loss (EBL), intraoperative complications and concurrent procedures), outcomes within 30 days post-procedure (length of hospital stay, ER visits, hospital readmissions, and post-operative complications). Hernia characteristics were based on the European Hernia Society (EHS) classification system for size and location [16], and extrapolated from intraoperative findings and CT scan performed within 12 months pre-operatively. Intraoperative measurements were made using a ruler intra-abdominally after the hernia contents were reduced. CT measurements were also made based on a ruler measuring the length and width of the hernia neck. Long-term follow-up assessments included any symptoms concerning recurrence, physical/examination or imaging confirming recurrence, time to recurrence, and average follow-up time. Due to limited in-person follow-up during COVID-19, phone calls and emailed surveys were utilized with in-person visits scheduled when patients reported any symptoms consistent with a recurrence.
TA-SM and eTEP hernia repair
Our surgical approach for TA-SM repair was to enter the abdomen by placing the initial port in the mid-abdomen opposite to the largest portion of the hernia using the open Hasson technique and subsequently adding two additional working ports along the same axis laterally (Fig. 1). The da Vinci Si or Xi Surgical System (Sunnyvale, CA) was then docked and intra-abdominal adhesions were lysed to fully expose the hernia. The decision to perform a purely pre-peritoneal repair or add a transversus release was made based on the operating surgeon’s clinical judgment based on the size of the defect and the compliance of the abdominal wall. In most cases, we did not find a TAR was necessary. Intraperitoneal onlay mesh (IPOM) was performed in cases where peritoneal violations could not be salvaged, and in these cases, a microporous PTFE mesh with biologic coating was used. Otherwise, the preferential mesh for pre-peritoneal repair was a self-gripping, lightweight polyester mesh.

TA-SM operative technique starts with gaining abdominal access a and dissecting adhesions to explore the hernia b. The periperitoneal space is dissected c and the hernia defect is closed with barbed suture d. Mesh is placed in the preperitoneal space e and the flap is closed with another barbed monofilament suture f
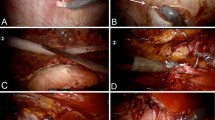
Totally extra-peritoneal robotic ventral hernia repair was performed with a unilateral, extra-peritoneal port configuration using the da Vinci Xi system (Sunnyvale, CA). The initial port is placed on either the left or right subcostal region just medial to the defect (Fig. 2). If necessary to ensure a tension-free closure, a unilateral TAR is done by continuing the dissection laterally to divide the transversus abdominis, while for a bilateral TAR three additional trocars are inserted. If a concurrent inguinal hernia was present, we added additional trocars in the upper midline and contralateral upper quadrant to allow for better dissection in the groin. This change in approach was applied for both eTEP and TA-SM surgeries.

eTEP operative technique starts with gaining extra-peritoneal access a and places ports laterally b. The retrorectus space is dissected c to expose the hernia defect d, which is then closed with barbed suture e before placing mesh
Outcomes
Peri-operative outcomes collected included operative time, intraoperative complications, procedure conversions (such as open procedure, placement of mesh in location other than what was initially intended, or non-mesh repair), and length of hospital stay. Thirty-day complications examined were emergency room visits, hospital admissions, surgical site occurrences (SSOs) included surgical site infections (SSIs), seroma, hematoma, ileus, and small bowel obstruction. Complications were categorized according to the Clavien–Dindo classification system.
Statistical analysis
Statistical analysis was performed using Stata statistical software version 15.0 (StataCorp, College Station, TX). An intention-to-treat model was applied for data in both cohorts. Fisher’s exact test and Chi-square test were used for categorical variables. Two-sample t-tests with a 95% confidence interval were used to determine significance for continuous variables. Statistical significance was defined as p < 0.05.
Results
Within the study period, there were 50 patients who underwent eTEP and 108 patients who had TA-SM. There were no statistically significant differences in ACS-NSQIP Surgical Risk Calculator medical comorbidities between the eTEP and TA-SM patient population (Table 1) other than dyspnea on exertion (p < 0.05). Mean age for both cohorts was approximately 53 years, with 62% consisting of female patients, and with a mean BMI of 33 kg/m2 (p = 0.46). Although rehabilitation efforts were made for smoking cessation within 30 days pre-procedure, this could not be easily tracked by our medical record system. Our reported tobacco usage of 16% in the eTEP cohort and 12% in the TA-SM cohort are conservative estimates and actual smoking rates 30 days pre-operatively are likely lower than what was documented. More eTEP patients had a history of prior hernia repair compared to TA-SM patients (46% vs. 30%, p = 0.07).
Operative outcomes
Of the 50 patients who underwent the eTEP approach, one (2%) was converted to open due to extensive tension despite bilateral transversus abdominus release and one (2%) was converted to TA-SM (Fig. 3). Among the 108 TA-SM procedures, only 85 patients (79%) were treated as intended. Two patients (2%) were converted to open, one secondary to devitalized skin during dissection, and the other due to an enterotomy during trocar placement. Nineteen patients (18%) had IPOM repairs due to poor integrity of the peritoneal flap after dissection. Two patients (2%) had primary repair non-mesh repair due to concern for contamination.
Mean hernia defect sizes, and subsequently mesh sizes, were larger in patients with eTEP than TA-SM (Table 2). In the eTEP cohort, the mean hernia defects were 109.1 cm2 compared to 31.8 cm2 in TA-SM (p = 0.043), reflecting a larger mesh size used for eTEP mesh (432.8 cm2 vs. 137.9 cm2 for TA-SM, p = 0.001). There was a homogenous location according to EHS classification and there were no differences in wound class, OR time, intraoperative complications, or conversion to open. The rate of concurrent procedures performed was similar in both the groups (20%, p = 0.55) with the most common being a bilateral inguinal hernia repair. In addition, 5 eTEP patients (10%) as opposed to 24 TA-SM (22%) required a unilateral or bilateral TAR tension-free midline closure (p = 0.02).

Successful eTEP or TA-SM hernia repair according to intention to treat and long-term follow-up
Short-term outcomes
Length of hospital stay was substantially shorter in the eTEP group, 1.3 days versus 2.2 days in TA-SM (p = 0.002) (Table 3). There were no differences in overall complications (6% vs. 12%, p = 0.58), 30-day emergency room visits (12% vs. 8.3%, p = 0.46) and readmission rates (4% vs. 6.5%, p = 0.26) for eTEP and TA-SM, respectively. The most common complication in eTEP patients was a seroma, with two patients requiring drainage under local anesthetic. One eTEP patient developed an SSI treated with antibiotics and another developed a hematoma treated conservatively. In the TA-SM group, four patients had complications requiring operative intervention under general anesthesia. Two patients had a bowel obstruction due to peritoneal rents requiring laparotomy and two patients had SSIs requiring debridement—one from an infected hematoma. Three other patients had hematomas, one was treated conservatively, one required transfusion as she had been on anticoagulation for a hematologic disorder, and one was treated with antibiotics due to concern for infection. Two patients had a seroma that were treated conservatively within the 30-day period but ultimately required debridement for chronic discomfort. Two patients developed an ileus: one was treated with observation and one was treated with nasogastric decompression. One patient developed thrombophlebitis and was treated with antibiotics.
Long-term outcomes
Eighty-six percent (n = 43) of eTEP patients had long-term follow-up at a mean of 1.8 years, while 98% of TA-SM patients (n = 106) with a mean of 3.18 years follow-up time (Table 4, Fig. 3). Since the change of practice in using eTEP preferentially occurred in 2019, mean follow-up time was longer in the TA-SM patients. Recurrences were based on physical exam findings or concerning clinical findings in which case a CT was obtained. There was no statistically significant difference in recurrence rates between the two types of hernia repair for their respective follow-up durations (4% for eTEP and 12% in TA-SM, p = 0.28). The average time to recurrence was 9.17 months in the eTEP group and 11.05 months in TA-SM group. In the eTEP cohort, one recurrence occurred laterally, and one occurred in a patient with history of an enterocutaneous fistula takedown. In the TA-SM cohort, a majority of the recurrences occurred in the midline, superior or inferior to the mesh, with two mesh failures reported.
Discussion
This retrospective analysis compares a single surgeon’s transition from transabdominal to totally extra-peritoneal ventral hernia repair on the robotic platform. Peri-operative data, 30-day and 1-year post-operative outcomes indicate that the extra-peritoneal approach can be adapted safely and may have several advantages. The rate of conversion (open or alternate robotic procedure) was low in the eTEP group. Only 78% of transabdominal repairs could be completed with sublay mesh placement, while 96% of eTEP procedures were executed as planned (p < 0.05). While our previous experience with TA-SM repair may have contributed to acceleration of our learning curve with eTEP and the lower rate of conversion, we found peritoneal violations were easier to manage with eTEP. With eTEP, we noted that there was more redundancy of the retrorectus flap which allowed for better salvage of any peritoneal defects, allowed for fewer conversions to IPOM. Conversion to open was low in both cohorts (approximately 2%) which in our experience is due to better visualization of robotic platform in both the extra-peritoneal and transabdominal plane.
We also found that the length of stay was 0.9 days shorter in the eTEP group at 1.3 vs 2.2 days (p = 0.002). Post-operative complications, emergency room visits and hospital readmissions at 30 days remained unchanged despite the earlier discharge. No changes to our protocol for pain management were made during the study duration. It is possible that insufflation primarily in the extra-peritoneal rather than intra-abdominal space may be responsible for improvements in recovery. A group comparing post-operative pain after eTEP and IPOM found a decrease in visual analog pain scores after eTEP [20]. They concluded mesh fixation in IPOM was the primary reason for increase in pain in the intra-abdominal cohort. While mesh fixation was not applicable in our intra-abdominal cohort, disruption of the pre-peritoneal plane may have caused similar irritation of nerve fibers in the space [21]. In the inguinal hernia literature, TA-SM and TEP have been compared, and ultimately, no difference in post-operative pain or return to activity has been found in larger scale studies [22]. However, results cannot necessarily be extrapolated to ventral hernia repair using these two approaches as mesh fixation is significant contributor to post-operative pain in inguinal hernias. Further study comparing pain response with transabdominal versus extra-peritoneal dissection for ventral hernia repairs is needed.
Long-term recurrence at approximately 2 years post-operatively trended towards lower rates in eTEP patients despite hernia defect sizes being larger, although this finding was not statistically significant. There are several possible reasons for this. Once again, our learning curve with eTEP may have been impacted by our preceding experience with robotic TA-SM, leading to more sound technique. However, we did note that several of our recurrences in the TA-SM cohort occurred after the latter half of our experience with the procedure rather than in the earlier stages. Approximation of the linea alba during eTEP helped reinforce closure of hernia defects. Dissection of the retrorectus space allowed for better mesh overlap rather than the standard 3–5 cm overlap we achieved in TA-SM cases. However, with more extensive dissection, there was a higher seroma formation in eTEP which we did not note in TA-SM. Lastly, placement of mesh consistently in the retrorectus as opposed to the pre-peritoneal space preferentially may have helped with mesh incorporation and prevention of recurrence. The Rives–Stoppa repair has long been popular for this reason with large-scale studies demonstrating low recurrence rates of 4.1% even 2 years post-operatively [23]. However, previous head-to-head comparisons of recurrence using a Rives–Stoppa repair as opposed to pre-peritoneal repair have not demonstrated much difference in recurrence [24]. Potential advantages of the Rives–Stoppa repair must be better informed to prevent overuse of the valuable retrorectus plane.
This study is the first to evaluate outcomes in both the peri-operative phase and long-term after enhanced-view totally extra-peritoneal and transabdominal hernia repair with sublay mesh using the robotic platform. Kudsi et al. have published short-term outcomes after robotic extra-peritoneal versus transabdominal hernia repair in the retromuscular plane [25]. They found eTEP could be performed more efficiently and with fewer complications intraoperatively. In contrast, our data demonstrated similar operative times for both procedures and no changes in intraoperative complications. Differences in major post-operative complications between the extra-peritoneal and transabdominal cohorts were not significant in either the Kudsi et al. study or in our experience. Minor post-operative complications (Clavien–Dindo I and II), particularly SSIs, were higher in the transabdominal group for Kudsi et al. This trend was not observed in our case and can likely be attributed to our conservative application of the retromuscular dissection and preferential application of pre-peritoneal repair, when possible, as opposed to Kusdi et al. who did not include TA-SM repair in their analysis.
The experiential nature of our study presents several limitations. While our study groups were comparable in terms of demographics and baseline medical comorbidities (aside from dyspnea), hernia characteristics were quite variable in the two cohorts observed. The incidence of recurrent hernias was higher in eTEP as opposed to TA-SM patients (approached statistical significance) and the hernia defect size was also larger in the eTEP cohort (trend was statistically significant). During the study period, we did note an increase in the referral of complex hernias to our center. In addition, we also noted an anecdotal increase in rectus diastasis which could not be controlled for as we did not document the presence of diastasis consistently in TA-SM patients. We explored using propensity score matching (PSM) to reduce bias from several of these confounding variables. However, our sample size was limited and varied too drastically in terms of characteristics to allow for appropriate replacement during PSM. Although PSM is an increasingly popular method for statistical analysis, a small sample size and selection bias in assigning treatment groups can obscure results [26]. Another limitation is inclusion of both primary and incisional hernias in the same study population due to inherent in characteristics of these hernias that can lead to differences in outcomes [27]. Our retrospective analysis of data from a single surgeon from a single institution also limits the findings of this study. A larger scale prospective study is required to find more meaningful and consistent trends for both the extra-peritoneal and transabdominal approaches. Lastly, the absence of quality-of-life metrics was another significant limitation.
Conclusions
We share results from our experience transitioning from robotic TA-SM to eTEP. While it may be intimidating to adopt extra-peritoneal hernia repair in the minimally invasive setting, our results indicate that eTEP can be performed safely and efficiently with minimal complications. While the rate of seroma formation may be higher than in transabdominal repair, long-term outcomes are promising, making earlier adaptation of eTEP more advantageous. However, the jury is still out as to whether the extra-peritoneal or transabdominal approach is the better repair. There is likely a time and place that is optimal for each repair, which has yet to be determined and requires further study.
References
Bower C, Roth JS (2013) Economics of abdominal wall reconstruction. Surg Clin North Am 93:1241–1253
Poulose BK, Shelton J, Phillips S, Moore D, Nealon W, Penson D, Beck W, Holzman MD (2012) Epidemiology and cost of ventral hernia repair: making the case for hernia research. Hernia 16:179–183
Guzman-Pruneda FA, Huang LC, Collins C, Renshaw S, Narula V, Poulose BK (2021) Abdominal core quality of life after ventral hernia repair: a comparison of open versus robotic-assisted retromuscular techniques. Surg Endosc 35:241–248
LeBlanc KA, Gonzalez A, Dickens E, Olsofka J, Ortiz-Ortiz C, Verdeja JC, Pierce R, Prospective Hernia Study G (2021) Robotic-assisted, laparoscopic, and open incisional hernia repair: early outcomes from the Prospective Hernia Study. Hernia 25:1071–1082
Novitsky YW, Elliott HL, Orenstein SB, Rosen MJ (2012) Transversus abdominis muscle release: a novel approach to posterior component separation during complex abdominal wall reconstruction. Am J Surg 204:709–716
Carbonell AM, Cobb WS, Chen SM (2008) Posterior components separation during retromuscular hernia repair. Hernia 12:359–362
LeBlanc K (2016) Proper mesh overlap is a key determinant in hernia recurrence following laparoscopic ventral and incisional hernia repair. Hernia 20:85–99
Wennergren JE, Askenasy EP, Greenberg JA, Holihan J, Keith J, Liang MK, Martindale RG, Trott S, Plymale M, Roth JS (2016) Laparoscopic ventral hernia repair with primary fascial closure versus bridged repair: a risk-adjusted comparative study. Surg Endosc 30:3231–3238
Belyansky I, Zahiri HR, Park A (2016) Laparoscopic Transversus Abdominis Release, a Novel Minimally Invasive Approach to Complex Abdominal Wall Reconstruction. Surg Innov 23:134–141
Penchev D, Kotashev G, Mutafchiyski V (2019) Endoscopic enhanced-view totally extra-peritoneal retromuscular approach for ventral hernia repair. Surg Endosc 33:3749–3756
Schroeder AD, Debus ES, Schroeder M, Reinpold WM (2013) Laparoscopic transperitoneal sublay mesh repair: a new technique for the cure of ventral and incisional hernias. Surg Endosc 27:648–654
Lu R, Addo A, Ewart Z, Broda A, Parlacoski S, Zahiri HR, Belyansky I (2020) Comparative review of outcomes: laparoscopic and robotic enhanced-view totally extra-peritoneal (eTEP) access retrorectus repairs. Surg Endosc 34:3597–3605
Martin-Del-Campo LA, Weltz AS, Belyansky I, Novitsky YW (2018) Comparative analysis of perioperative outcomes of robotic versus open transversus abdominis release. Surg Endosc 32:840–845
Bracale U, Corcione F, Neola D, Castiglioni S, Cavallaro G, Stabilini C, Botteri E, Sodo M, Imperatore N, Peltrini R (2021) Transversus abdominis release (TAR) for ventral hernia repair: open or robotic? Short-term outcomes from a systematic review with meta-analysis. Hernia. https://doi.org/10.1007/s10029-021-02487-5
Kudsi OY, Gokcal F (2021) Lateral approach totally extra-peritoneal (TEP) robotic retromuscular ventral hernia repair. Hernia 25:211–222
Muysoms FE, Miserez M, Berrevoet F, Campanelli G, Champault GG, Chelala E, Dietz UA, Eker HH, El Nakadi I, Hauters P, Hidalgo Pascual M, Hoeferlin A, Klinge U, Montgomery A, Simmermacher RK, Simons MP, Smietanski M, Sommeling C, Tollens T, Vierendeels T, Kingsnorth A (2009) Classification of primary and incisional abdominal wall hernias. Hernia 13:407–414
Andreuccetti J, Sartori A, Lauro E, Crepaz L, Sanna S, Pignata G, Bracale U, Di Leo A (2021) Extended totally extra-peritoneal Rives-Stoppa (eTEP-RS) technique for ventral hernia: initial experience of The Wall Hernia Group and a surgical technique update. Updates Surg 73:1955–1961
Bilimoria KY, Liu Y, Paruch JL, Zhou L, Kmiecik TE, Ko CY, Cohen ME (2013) Development and evaluation of the universal ACS NSQIP surgical risk calculator: a decision aid and informed consent tool for patients and surgeons. J Am Coll Surg 217:833–842
NSQIP A ACS NSQIP Surgical Risk Calculator. American College of Surgeons
Kumar N, Palanisamy NV, Parthasarathi R, Sabnis SC, Nayak SK, Palanivelu C (2021) A comparative prospective study of short-term outcomes of extended view totally extra-peritoneal (e-TEP) repair versus laparoscopic intraperitoneal on lay mesh (IPOM) plus repair for ventral hernia. Surg Endosc 35:5072–5077
Struller F, Weinreich FJ, Horvath P, Kokkalis MK, Beckert S, Konigsrainer A, Reymond MA (2017) Peritoneal innervation: embryology and functional anatomy. Pleura Peritoneum 2:153–161
Wei FX, Zhang YC, Han W, Zhang YL, Shao Y, Ni R (2015) Transabdominal Pre-peritoneal (TAPP) Versus Totally Extra-peritoneal (TEP) for Laparoscopic Hernia Repair: A Meta-Analysis. Surg Laparosc Endosc Percutan Tech 25:375–383
Hartog F, Sneiders D, Darwish EF, Yurtkap Y, Menon AG, Muysoms FE, Kleinrensink GJ, Bouvy ND, Jeekel J, Lange JF (2022) Favorable Outcomes After Retro-Rectus (Rives-Stoppa) Mesh Repair as Treatment for Noncomplex Ventral Abdominal Wall Hernia, a Systematic Review and Meta-analysis. Ann Surg 276:55–65
Dougaz MW, Chaouch MA, Cherni S, Khalfallah M, Jerraya H, Bouasker I, Nouira R (2020) Pre-peritoneal versus retromuscular mesh repair for ventral abdominal hernias: a propensity matched analysis. Indian J Surg 82:868
Kudsi OY, Chang K, Bou-Ayash N, Gokcal F (2020) Transabdominal (TA) versus totally extra-peritoneal (TEP) robotic retromuscular ventral hernia repair: a propensity score matching analysis. Surg Endosc 34:3550–3559
Bottigliengo D, Baldi I, Lanera C, Lorenzoni G, Bejko J, Bottio T, Tarzia V, Carrozzini M, Gerosa G, Berchialla P, Gregori D (2021) Oversampling and replacement strategies in propensity score matching: a critical review focused on small sample size in clinical settings. BMC Med Res Methodol 21:256
Stabilini C, Cavallaro G, Dolce P, Capoccia Giovannini S, Corcione F, Frascio M, Sodo M, Merola G, Bracale U (2019) Pooled data analysis of primary ventral (PVH) and incisional hernia (IH) repair is no more acceptable: results of a systematic review and metanalysis of current literature. Hernia 23:831–845
Funding
Not applicable.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors of this paper have no financial or non-financial interests that are directly or indirectly related to the work submitted for publication.
Ethical approval
This article does not contain studies directly with human or animal participants performed by any of the authors.
Human and animal rights
This manuscript is primarily a review of data already collected. If human participants were contacted to monitor for recurrence, their participation was within the boundaries of patient care.
Informed consent
For this type of study formal consent is not required. Patients contacted for discussion to determine recurrence were given the option to decline further contact.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zaman, J., Teixeira, L., Patel, P.B. et al. From transabdominal to totally extra-peritoneal robotic ventral hernia repair: observations and outcomes. Hernia 27, 635–643 (2023). https://doi.org/10.1007/s10029-023-02767-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-023-02767-2