
Abstract
Introduction
Collecting clinical data is viewed as the gold standard for assessing health-care quality. However, considerable investment is needed if the quality of care is to be recorded over a long period of time. Accordingly, the question arises as to whether routine administrative data may be used for quality assurance purposes if certain methodological standards are followed. This present study now compares the outcomes of inguinal hernia repair from the Herniamed Hernia Registry with routine data from Germany’s largest sickness fund, the Local General Sickness Fund “AOK”.
Materials and methods
Included in the study were the hospital inpatient cases for the years 2011–2013 with inguinal hernia surgical repair whose data had been prospectively entered into the voluntary Herniamed Hernia Registry by 318 participating hospitals. These collectives were then compared, on the basis of the routine administrative data available, with patients from the AOK sickness fund who had been operated on during the same time period. The outcome criteria selected were the perioperative complication rates within 30 days as well as the recurrence rate and the pain rate requiring treatment at 1-year follow-up.
Results
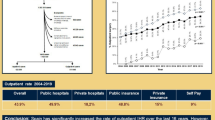
The data records examined comprised 64,748 cases from the Herniamed Registry and 130,121 AOK cases. Since in the Herniamed collective, the proportion of bilateral procedures was significantly higher, only the collectives of elective primary unilateral inguinal hernias in men (Herniamed n = 37,667; AOK n = 78,973) were compared. The most pronounced difference between these two collectives was in the proportion of laparo-endoscopic procedures (Herniamed 61.3% vs AOK 49.0%; p < 0.001). Accordingly, the Herniamed collective was found to have a significantly lower postoperative surgical complication rate (Herniamed 1.5% vs AOK 2.6%; p < 0.001) and surgical site infection (SSI) rate (Herniamed 0.3% vs AOK 0.6%; p < 0.001) within 30 days after the operation. On the other hand, the pain rates requiring treatment in the Herniamed collective were somewhat higher (Herniamed 3.0% vs AOK 2.6%; p < 0.001). No difference was found in the recurrence rate at 1-year follow-up (Herniamed 1.0% vs AOK 0.9%; ns).
Conclusion
Subject to critical evaluation of the limitations of data acquisition in this study, it does appear possible to use the routine administrative data from the AOK Sickness Fund for assessment of the quality of inguinal hernia surgery in Germany. Voluntary participation in the Herniamed Registry appears to be characterized by the fact that the participating hospitals conduct a higher proportion of laparo-endoscopic inguinal hernia repair. That could possibly explain the differences in outcome. However, in large patient collectives, statistical significance should not always be equated with clinical relevance. Univariate analysis does not take account of differences in the hernia findings, risk factors or operative details. Further efforts should be employed in future to improve the accuracy and granularity of routine administrative data for assessing the quality of care and to decrease the cost of gathering such data.
Similar content being viewed by others


References
Statistisches Bundesamt Bonn (2018) Fallpauschalenbezogene Krankenhausstatistik (DRG-Statistik). https://www.destatis.de/DE/Startseite.html
Statistisches Bundesamt Bonn (2018) Die 50 häufigsten Operationen der vollstationären patienten in Krankenhäusern. https://www.destatis.de/DE/Startseite.html
American College of Surgeons (2015) ACS NSQIP data is more accurate than administrative data for surgical patients outcomes. https://www.sciencedaily.com/releases/2015/07/150726200044.htm
Bufalino V, Peterson ED, Burke GL, LaBresh KA, Jones DW, Faxon DP et al (2006) Payment for quality: guiding principles and recommendations principles and recommendations from the american heart association’s reimbursement, coverage, and access policy development workshop. Circulation 113:1151–1154. https://doi.org/10.1161/CIRCULATIONAHA.105.171760
Maier B, Wagner K, Behrens S, Bruch L, Busse R, Schmidt D et al (2016) Comparing routine administrative data with registry data for assessing quality of hospital care in patients with myocardial infarction using deterministic record linkage. BMC Health Serv Res 16:605. https://doi.org/10.1186/s12913-016-1840-S
Krumholz HM, Brindis RG, Brush JE, Cohen DJ, Epstein AJ, Furie K et al (2006) Standards for statistical models used for public reporting of health outcomes an American Heart Association Scientific Statement from the Quality of Care and Outcomes Research Interdisciplinary Writing Group. Circulation 113:456–462. https://doi.org/10.1161/CIRCULATIONAHA.105.170769
Nimptsch U (2016) Disease-specific trends of comorbidity coding and implications for risk adjustment in hospital administrative data. Health Serv Res 51(3):981–1001
Statistisches Bundesamt Bonn (2019) Bevölkerung und Erwerbstätigkeit. https://www.destatis.de/DE/Publikationen/Thematisch/Bevoelkerung/Bevoelkerungsstand/Bevoelkerungsfortschreibung.html
Heller G, Günster C (2008) Mit Routinedaten Qualität in der Medizin sichern: Aktuelle Entwicklungen und weitere Perspektiven. Heft 1:26–34
Behrendt CA, Heidemann F, Rieß HC, Stoberock K, Debus SE (2017) Registry and health insurance claims data in vascular research and quality improvement. Vasa 46(1):11–15. https://doi.org/10.1024/0301-1526/a000589
Aylin P, Lees T, Baker S, Prytherch D, Ashley S (2007) Descriptive study comparing routine hospital administrative data with the vascular Society of Great Britain and Ireland’s National Vascular Database. Eur J Vasc Endovasc Surg 33:461–465. https://doi.org/10.1016/j.ejvs.2006.10.033
Wessling M, Gravius S, Gebert C, Smektala R, Günster C, Hardes J, Rhomberg I, Koller D (2015) Quality in revision arthroplasty: a comparison between claims data analysis and external quality assurance. Z Orthop Unfallchirurgie 154(1):63–71
Stechemesser B, Jacob DA, Schug-Paß Köckerling F (2012) Herniamed: an internet-based registry for outcome research in hernia surgery. Hernia 16:269–276. https://doi.org/10.1007/s10029-012-0908-3
Kyle-Leinhase I, Köckerling F, Jørgensen LN, Montgomery A, Gillion JF, Rodriguez JAP, Hope W, Muysoms F (2018) Comparison of hernia registries: the CORE project. Hernia 22:561–575. https://doi.org/10.1007/s10029-017-1724-6
Köckerling F, Stechemesser B, Hukauf M, Kuthe A, Schug-Pass C (2016) TEP versus Lichtenstein: which technique is better for the repair of primary unilateral inguinal hernias in men? Surg Endosc 30:3304–3313. https://doi.org/10.1007/s00464-015-4603-1
Köckerling F, Bittner R, Kofler M, Mayer F, Adolf D, Kuthe A, Weyhe D (2017) Lichtenstein versus total extraperitoneal patch plasty versus transabdominal patch plasty technique for primary unilateral inguinal hernia repair. Ann Surg 269:351–357. https://doi.org/10.1097/SLA.0000000000002541
The HerniaSurge Group (2018) International guidelines for groin hernia management. Hernia 22:1–165. https://doi.org/10.1007/s10029-017-1668-x
Hoffmann F, Icks A (2012) Differences in der Versichertenstruktur von Krankenkassen und deren Auswirkungen für die Versorgungsforschung: Ergebnisse des Bertelsmann-Gesundheitsmonitors. Gesundheitswesen 74:291–297. https://doi.org/10.1055/s0031-1275711
Weyhe D, Tabriz N, Sahlmann B, Uslar VN (2017) Risk factors for perioperative complications in inguinal hernia repair—a systematic review. Innov Surg Sci 2:47–52
Öberg S, Andresen K, Klausen TW, Rosenberg J (2018) Chronic pain after mesh versus nonmesh repair of inguinal hernias: a systematic review and a network meta-analysis of randomized controlled trials. Surgery 163(5):1151–1159. https://doi.org/10.1016/j.surg.2017.12.017
Registret för Ljumskbråcksoperationer.Östersund (2016) Svenskt Brackregister. https://www.svensktbrackregister.se
Reinpold W (2017) Risk factors of chronic pain after inguinal hernia repair: a systematic review. Innov Surg Sci 2:61–68. https://doi.org/10.1515/iss-2017-0017
Haapaniemi S, Nilsson E (2002) Recurrence and pain three years after groin hernia repair Validation of postal questionnaire and selective physical examination as a method of follow-up. Eur J Surg 168:22–28. https://doi.org/10.1080/110241502317307535
Fry BT, Campbell DA, Englesbe MJ, Vu JV (2019) Using patient-reported outcomes to enhance appropriateness in low-risk elective general surgery. Ann Surg 269:41–42
Funding
Grants to fund the Herniamed registry from Johnson&Johnson, Norderstedt; Karl Storz, Tuttlingen; pfm medical, Cologne; Dahlhausen, Cologne; B. Braun, Tuttlingen; Menke Med, Munich; Bard, Karlsruhe.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors have no conflicts of interest or financial disclosures.
Ethical approval
As only routine treatment of the patients was documented, no ethical approval was necessary.
Human and animal rights
No studies with human participants or animals were performed.
Informed Consent
All patients documented in the Herniamed registry gave their informed consent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Köckerling, F., Maneck, M., Günster, C. et al. Comparing routine administrative data with registry data for assessing quality of hospital care in patients with inguinal hernia. Hernia 24, 143–151 (2020). https://doi.org/10.1007/s10029-019-02009-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-019-02009-4