
Abstract
Background
The recurrence rate after groin hernia repair (GHR) has been estimated to be between 1–10% in adult patients. Neither national rates nor trends in recurrence over time have been reliably established for Medicare patients in the USA.
Materials
We evaluated patients undergoing GHR (inguinal = IHR; femoral = FHR) from 2011 to 2014 from the Medicare Provider Analysis and Review database. Patients were identified using ICD-9 diagnosis and ICD-9 and CPT procedure codes, stratified both by primary vs. recurrent hernia repair and by sex. One-tailed Cochran–Armitage tests evaluated trends over time and a generalized estimating equation model estimated factors associated with recurrent IHR or FHR.
Results
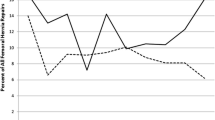
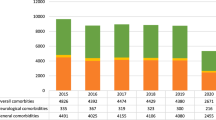
We identified 407,717 patients (87.0%, ≥ 65 years) who underwent an IHR and 11,578 (91.0%, ≥ 65 years) who underwent a FHR. The proportion of IHRs for recurrence decreased statistically from 14.3% in 2011 to 13.9% in 2014 (p < 0.01) in males and was increased, but not statistically so (7.0–7.4%) in females (p = 0.08). The proportion of FHRs for recurrence was decreased, but not statistically so (16.3–14.8%, p = 0.29) in males and increased in females (5.3–6.3%, p = 0.02). On multivariable analysis, males were more than twice as likely as females to undergo recurrent repair (IHR or FHR, both p < 0.01).
Conclusions
Within the Medicare population, recurrence rates after groin hernia repairs were found to be higher than previously reported but have remained clinically stable over time. Establishing and reducing this rate is important for patient outcomes and expectations.


Similar content being viewed by others

References
Rutkow IM (2003) Demographic and socioeconomic aspects of hernia repair in the United States in 2003. Surg Clin N Am 83(5):1045–1051, v-vi
Bittner R, Sauerland S, Schmedt CG (2005) Comparison of endoscopic techniques vs Shouldice and other open nonmesh techniques for inguinal hernia repair: a meta-analysis of randomized controlled trials. Surg Endosc 19(5):605–615
Burcharth J (2014) The epidemiology and risk factors for recurrence after inguinal hernia surgery. Dan Med J 61(5):B4846
Andresen K, Friis-Andersen H, Rosenberg J (2016) Laparoscopic repair of primary inguinal hernia performed in public hospitals or low-volume centers have increased risk of reoperation for recurrence. Surg Innov 23(2):142–147
Bendavid R (1989) Femoral hernias: primary versus recurrence. Int Surg 74(2):99–100
Burcharth J, Andresen K, Pommergaard HC, Bisgaard T, Rosenberg J (2014) Direct inguinal hernias and anterior surgical approach are risk factors for female inguinal hernia recurrences. Langenbeck’s Arch Surg 399(1):71–76
Haapaniemi S, Nilsson E (2002) Recurrence and pain three years after groin hernia repair. Validation of postal questionnaire and selective physical examination as a method of follow-up. Eur J Surg 168(1):22–28
Nilsson E, Kald A, Anderberg B, Bragmark M, Fordell R, Haapaniemi S, Heuman R, Lindhagen J, Stubberod A, Wickbom J (1997) Hernia surgery in a defined population: a prospective three year audit. Eur J Surg 163(11):823–829
Center for Medicare and Medicaid Services, Medicare Program—general information (2017). https://www.cms.gov/Medicare/Medicare-General-Information/MedicareGenInfo/index.html. Accessed 7 Aug 2017
Nilsson E, Haapaniemi S, Gruber G, Sandblom G (1998) Methods of repair and risk for reoperation in Swedish hernia surgery from 1992 to 1996. Br J Surg 85(12):1686–1691
Cox TC, Huntington CR, Blair LJ, Prasad T, Heniford BT, Augenstein VA (2017) Quality of life and outcomes for femoral hernia repair: does laparoscopy have an advantage? Hernia 21(1):79–88
Amid PK (2004) Lichtenstein tension-free hernioplasty: its inception, evolution, and principles. Hernia 8(1):1–7
Huerta S, Patel PM, Mokdad AA, Chang J (2016) Predictors of inguinodynia, recurrence, and metachronous hernias after inguinal herniorrhaphy in veteran patients. Am J Surg 212(3):391–398
Neumayer LA, Gawande AA, Wang J, Giobbie-Hurder A, Itani KM, Fitzgibbons RJ Jr, Reda D, Jonasson O (2005) Proficiency of surgeons in inguinal hernia repair: effect of experience and age. Ann Surg 242(3):344–348 (discussion 348–352)
Ramshaw B, Abiad F, Voeller G, Wilson R, Mason E (2003) Polyester (Parietex) mesh for total extraperitoneal laparoscopic inguinal hernia repair: initial experience in the United States. Surg Endosc 17(3):498–501
Thompson JS, Gibbs JO, Reda DJ, McCarthy M Jr, Wei Y, Giobbie-Hurder A, Fitzgibbons RJ Jr (2008) Does delaying repair of an asymptomatic hernia have a penalty? Am J Surg 195(1):89–93
Zendejas B, Onkendi EO, Brahmbhatt RD, Lohse CM, Greenlee SM, Farley DR (2011) Long-term outcomes of laparoscopic totally extraperitoneal inguinal hernia repairs performed by supervised surgical trainees, Am J Surg 201(3):379–383 (discussion 383–384)
Rogers FB, Guzman EA (2011) Inguinal hernia repair in a community setting: implications for the elderly. Hernia 15(1):37–42
Abi-Haidar Y, Sanchez V, Itani KM (2011) Risk factors and outcomes of acute versus elective groin hernia surgery. J Am Coll Surg 213(3):363–369
Smink DS, Paquette IM, Finlayson SR (2009) Utilization of laparoscopic and open inguinal hernia repair: a population-based analysis. J Laparoendosc Adv Surg Techn Part A 19(6):745–748
Nolsoe A, Andresen K, Rosenberg J (2016) Repair of recurrent hernia is often performed at a different clinic. Hernia 20(6):783–787
Murphy BL, Ubl DS, Zhang J, Habermann EB, Farley D, Paley K (2018) Proportion of femoral hernia repairs performed for recurrence in the United States. Hernia 22(4):593–602
Burcharth J, Pommergaard HC, Bisgaard T, Rosenberg J (2015) Patient-related risk factors for recurrence after inguinal hernia repair: a systematic review and meta-analysis of observational studies. Surg Innov 22(3):303–317
Andresen K, Bisgaard T, Kehlet H, Wara P, Rosenberg J (2014) Reoperation rates for laparoscopic vs open repair of femoral hernias in Denmark: a nationwide analysis. JAMA Surg 149(8):853–857
El-Dhuwaib Y, Corless D, Emmett C, Deakin M, Slavin J (2013) Laparoscopic versus open repair of inguinal hernia: a longitudinal cohort study. Surg Endosc 27(3):936–945
Keller JJ, Muo CH, Lan YC, Sung FC, Lo FE, Chiang KY, Lyu SY, Tsai ST (2015) A nation-wide population-based study of inguinal hernia repair incidence and age-stratified recurrence in an Asian population. Hernia 19(5):735–740
Voorbrood CE, Burgmans JP, Clevers GJ, Davids PH, Verleisdonk EJ, van Dalen T (2015) Totally extraperitoneal (TEP) endoscopic hernia repair in elderly patients. Hernia 19(6):887–891
Wu JJ, Baldwin BC, Goldwater E, Counihan TC (2017) Should we perform elective inguinal hernia repair in the elderly? Hernia 21(1):51–57
Vigneswaran Y, Gitelis M, Lapin B, Denham W, Linn J, Carbray J, Ujiki M (2015) Elderly and octogenarian cohort: comparable outcomes with nonelderly cohort after open or laparoscopic inguinal hernia repairs. Surgery 158(4):1137–1143 (discussion 1143–1144)
Kald A, Nilsson E, Anderberg B, Bragmark M, Engstrom P, Gunnarsson U, Haapaniemi S, Lindhagen J, Nilsson P, Sandblom G, Stubberod A (1998) Reoperation as surrogate endpoint in hernia surgery. A three year follow-up of 1565 herniorrhaphies. Eur J Surg 164(1):45–50
Acknowledgements
The authors would like to acknowledge and thank the Mayo Clinic Department of Surgery, the Kern Center for the Science of Health Care Delivery, and Medtronic as substantial contributors of resources to this project.
Funding
The Mayo Clinic Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery provides salary support for Dr. Habermann, Dr. Murphy, and Mr. Ubl. Dr. Jianying Zhang is an employee of Medtronic and provided the analysis of the MedPAR Database. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to disclose. Dr. Zhang is an employee of Medtronic and completed the analysis of the MedPAR database. We teamed with Medtronic to help perform the statistical analyses of the MedPAR database due to their expertise in analyzing this extensive data source. Medtronic shared in our goals of identifying the current state of hernia repairs in the United States as a whole and offered to partner with us for this study. Dr. Zhang performed the statistical analysis of the MedPAR data, which was critically evaluated and discussed among all authors. All authors were involved in data interpretation. Our agreement with Medtronic precluded financial considerations for this project.
Ethical approval
This study was reviewed by the Mayo Clinic IRB and found to be exempt as it involved de-identified data from national databases and they determined that it does not constitute research involving human subjects as defined under 45 CFR 46.102.
Human and animal rights
This article does not contain any studies directly involving human participants, as it is a review of data already collected in a database.
Informed consent
For this type of study, formal consent was not necessary.
Rights and permissions
About this article

Cite this article
Murphy, B.L., Zhang, J., Ubl, D.S. et al. Surgical trends of groin hernia repairs performed for recurrence in medicare patients. Hernia 23, 677–683 (2019). https://doi.org/10.1007/s10029-018-1852-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-018-1852-7