
Abstract
This study aimed to review the existing published and grey literature describing the concepts of self-management, self-care, and self-help, and to capture strategies or techniques related to these concepts, for adolescents with emotional problems. Emotional problems are rising amongst adolescents, yet timely access to specialist mental health treatment is limited to those with greater severity of mental health difficulties. Self-management, self-care, and self-help strategies may be used by adolescents with emotional problems both in terms of those waiting for treatment and to prevent relapse. Given the overlap in existing definitions and the lack of clarity around these concepts in an adolescent mental health context, a scoping review of the literature is warranted to provide clarity. Eligible studies were those involving adolescents aged 10 to 19 years with symptoms of emotional problems. Studies referenced self-management, self-care, or self-help, not involving a professional, in this population. Quantitative, qualitative, economic, and mixed methods studies, as well as systematic, scoping, and literature reviews, from 2000 onwards and in the English language, were eligible for inclusion. A systematic search was conducted of both published and grey literature. Databases searched included PsycINFO, Medline, Embase, Web of Science, and CINAHL Plus. Mednar was also searched for unpublished studies and grey literature. Tables of themes, terms, and associated strategies are presented alongside a thematic analysis of the results. 62 articles were included. These were 20 quantitative studies, 14 systematic reviews, 10 qualitative studies, five review papers, four book chapters, four mixed methods studies, two dissertations, two meta-analyses and one scoping review and systematic review. Most of the included articles referenced self-help (n = 51), followed by self-management (n = 17) and self-care (n = 6). A total of 12 themes were identified from a reflexive thematic analysis of descriptions (and associated strategies) of self-management, self-help, or self-care in included texts. This scoping review provides clarity on the similarities and differences between how these concepts are discussed, and the strategies which are associated with each of these concepts in the relevant literature. Implications for policy and intervention development for adolescents’ self-management, self-help, and self-care of their mental health are discussed. There is considerable overlap in both the ways in which these concepts are described, and the strategies or approaches proposed in relation to them, supporting previous research suggesting these strategies should be grouped under a single term, such as “self or community approaches.” More research is needed for self-management, self-help, and self-care amongst marginalized groups as these adolescents may have the highest unmet need for mental health support.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
One in six young people aged five to 16 in the United Kingdom (UK) has a probable mental health disorder, and there is evidence that the likelihood of this increases with age [1]. Emotional problems in particular are rising amongst adolescents in the UK [2,3,4], and epidemiological studies suggest that the onset of adolescence itself is associated with increased depressive symptoms [5]. Emotional problems can range from mild to severe and include panic disorder, generalized anxiety disorder (GAD), separation anxiety, social phobia, specific phobias, obsessive compulsive disorder (OCD), post-traumatic stress disorder (PTSD) and depression [6]. Anxiety and depression are the most prevalent emotional problems amongst adolescents in the UK [2]. Despite this, only a third (32%) of children and young people with a probable mental health need access specialist mental health treatment [7].
Timely access to specialist child and adolescent mental health treatment is becoming more challenging due to resource constraints, long waiting lists, and a large proportion of referrals that are rejected by services [7, 8]. Access to specialist services is particularly challenging for adolescents with less severe symptoms [9]. Moreover, if children and young people’s referrals are accepted by specialist mental health services, they wait an average of two months for treatment [10]. Once treatment is accessed, the modal number of appointments attended by children and young people is one, with half of all cases being closed after three or fewer appointments were attended [11]. This may indicate that specialist mental services alone do not meet the needs or preferences of many referred young people, despite the severity of the mental health difficulties they are experiencing or the length of time they have waited for treatment [12].
There has been a shift in the UK towards the concepts of self-management, self-care, and self-help appearing more frequently in published research [13], good practice guidance [14], UK policy [15], and think tank or other organizational reports [16]. Self-management, self-care, and self-help interventions or strategies, such as exercise, meditation or journaling, could help adolescents to prevent the onset or re-emergence of a mental health problem, manage the symptoms of an existing problem, or provide them support while they wait for an appointment for specialist treatment, during treatment, or post-treatment [13, 17,18,19]. Strategies may be promoted to adolescents through professionally-led interventions in schools and the community [13]. Digital access to help or support has also been proposed as a way of supporting mental health self-management [20]. This includes strategies delivered online or in an app format, such as Headspace, a guided mindfulness, sleep, and meditation app [21], or Calm Harm, an app that teaches adolescents techniques to stop self-harming behavior [22]. Digital self-management has increased in popularity alongside other digital health interventions and e-health more generally [23]. Evidence suggests that adolescents actively consume health-related information online, including user-generated content such as online message boards [24], and this may be driving the use of digital self-management resources.
An important caveat is that self-management, self-help, and self-care strategies may not be appropriate for or desired by all adolescents seeking help or support for emotional problems. Self-care has a particularly weak evidence base, which could be due to the lack of a clear definition of self-care in the literature [25]. Some researchers argue that societal emphasis on self-management (rather than treatment by a mental health professional or support from one’s community) is influenced by a neoliberal agenda which prioritizes individualism over social support in addressing mental health problems [26]. It is important also to note that the self-help industry is extremely profitable, which may bias some of the evaluations of the efficacy of self-help interventions, as well as hinder the investigation of potential negative effects of self-help to maximize financial gains [27, 28].
At the same time, there is evidence that specialist treatment is not a magic bullet for treating mental health problems, and that treatment or support based on need or preference may be more efficacious, particularly for young people and families [29]. This is supported by high rates of relapse even after successful specialist treatment for young people across many mental health disorder diagnoses, indicating that specialist treatment may not permanently “fix” mental health problems [30]. Rather than taking a one-size-fits-all approach, UK policy and research is currently promoting and investigating shared decision making, patient empowerment, and choice to better meet the mental health needs of adolescents and their families in the places hey ordinarily go [29, 31]. This highlights that self-management strategies should not be considered a “stop gap” or simulacrum for “gold-standard” specialist mental health treatment, but instead could be adequate or even preferable to meet the mental health needs of many adolescents, even whilst they are accessing specialist treatment or once specialist treatment has ended.
Existing definitions for the concepts of self-care, self-management, and self-help are lacking in detail and applicability to adolescent mental health. Self-care has been defined as “caring for self when ill or positive actions and adopting behaviors to prevent illness” [32]. Self-management has been defined as an “individual’s ability to manage the symptoms, treatment, physical and psychosocial consequences and lifestyle changes inherent in living with a chronic condition” [32]. The MeSH term “self-help groups” is defined as “organizations which provide an environment encouraging social interactions through group activities or individual relationships” [32]. None of these definitions refer specifically to adolescents, who may experience self-management, self-help, or self-care differently from adults. For example, adolescents are in the unique position of having multiple stakeholders involved in their healthcare (e.g., parents or carers, other family members, school, GPs, or social workers), whilst this is not the case with most adults [33]. Therefore, to make a shared decision about treatment or support (which could include self-management, self-care, or self-help strategies or interventions), multiple perspectives about the adolescent’s difficulties must be considered [33].
Additionally, terms such as self-management, self-care, and self-help might be suffering from the “jingle-jangle fallacy”, which refers to two or more psychological concepts that sound the same or have similar-sounding names but mean different things, or vice versa [34]. The jingle-jangle fallacy has resulted in murky distinctions between these similar-sounding concepts, e.g., as in the case of self-concept and self-efficacy [35]. Imprecise terms can waste research time, create redundancies or unnecessary relabeling of constructs, and “prevent the recognition of correspondences that could help build cumulative knowledge” [34, p. 210].
Therefore, a synthesis of current research covering the topics of self-care, self-help, and self-management for adolescents with emotional problems would lead to several important outcomes. Firstly, if there are similarities across all three concepts in terms of definitions, descriptions, and associated strategies or techniques, policy should refer to these techniques under an umbrella term such as “self or community approaches” [13]. This would avoid the possibility of making incorrect assumptions about non-existent or irrelevant differences between these concepts (e.g., due to the jingle-jangle fallacy). It would also prevent a focus on one concept as a better source of support over another, when they may all have equal potential for meeting the needs and preferences of adolescents with emotional problems. Secondly, if there are indeed key differences between these concepts and their associated strategies or techniques, arguments could be made in favor of certain concepts and their associated strategies or techniques to address certain emotional problems. These could be promoted to adolescents with emotional problems through evidence-informed policy or good practice guidance. Additionally, these differences would affect the ways in which each concept is measured, e.g., if self-management, self-care, and self-help are operationalized differently, then they may require different measurements to accurately address their underlying constructs. However, if the terms can be used interchangeably, this may imply that they may be better operationalized, measured, and promoted through interventions under a single term. Finally, synthesis of the current research would help to identify any gaps in terms of under-researched concepts and related strategies or techniques amongst adolescents with emotional problems, which would pave the way for future research in these areas.
The first aim of the current scoping review is to draw on the literature to illuminate the ways in which the concepts of self-management, self-care and self-help are described in the context of adolescents with emotional problems. Secondly, this review seeks to categorize the descriptions of these concepts as well as the strategies or techniques which have been proposed to facilitate self-management, self-care, or self-help for this group. A third aim is to compare the existing descriptions of self-management, self-care, and self-help for adolescents with emotional problems (e.g., anxiety, depression), with the aim of clarifying or creating a comprehensive description of these terms in the context of adolescent mental health based on the existing literature. This will enhance general understanding of how self-management, self-help, or self-care strategies can be effectively used by adolescents to promote their mental health, enabling the development of effective needs-based interventions. These descriptions have been explored narratively in this review and have been linked to the strategies and techniques proposed to facilitate each concept.
This review aims to explore these concepts broadly across the existing literature to better understand the essential components of self-management, self-care, and self-help and to develop a typology of related descriptions and strategies [36]. A typology is “a hierarchical system of categories used to organize objects according to their similarities and dissimilarities” [36]. One of the advantages of this approach is that it employs categorization to organize a variety of different or disparate ideas [36]. For the purposes of this study, categories have been displayed as a Venn diagram (see Fig. 2). Where overlap exists between descriptions, or if terms are used interchangeably, this has been addressed in the results section and discussed narratively.
An initial search using Google Scholar, the PsycINFO database (using the Ovid platform), and the Cochrane Database of Systematic Reviews was conducted using related keywords to determine (1) if there are studies that have been published related to the review questions, and (2) that there are no existing scoping or systematic reviews which already address the review questions. While there was one study identified which related to these concepts [13], it was established that there are currently (to our knowledge) no systematic or scoping reviews which focus broadly on self-management, self-care, and self-help for adolescents with emotional problems.
Methods
This scoping review was conducted in line with the Joanna Briggs Institute (JBI) methodology for scoping reviews [37], and it was consistent with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) [38]. This review was conducted in accordance with an a priori protocol [39]. A scoping review methodology was selected as it allowed for clarification of the key concepts (self-management, self-help, and self-care) in the literature, examination of how research is conducted around these concepts in the context of adolescents with emotional problems, and identification of key strategies relating to these concepts [40]. In line with previous research, the authors of this paper define scoping reviews as “a process of mapping the existing literature or evidence base” [41, p. 147].
Review question(s)
The objective of this scoping review was to locate and describe the existing published and grey literature defining the concepts of self-management, self-care, and self-help, as well as strategies or techniques related to these concepts for adolescents with emotional problems.
Specifically, the review questions were:
-
1.
How are the concepts of self-management, self-care, and self-help described in the context of adolescents with emotional problems?
-
2.
What strategies or techniques have been proposed to facilitate self-management, self-care, and self-help in adolescents with emotional problems?
Inclusion criteria
See Table 1 for a brief outline of the eligibility criteria for this scoping review, including inclusion and exclusion criteria.
Participants
Participants were adolescents aged 10–19 with emotional problems (also referred to as “emotional disorders”), including those with subclinical or self-reported symptoms (e.g., low mood) and those with a formal diagnosis (e.g., depression). Papers which involved co-morbid physical or mental health problems alongside an emotional problem were also included in this review. Emotional problems were selected for the focus of this scoping review for two reasons. Firstly, emotional problems are among the most prevalent mental health problems globally [42]. Secondly, there is evidence that depression and anxiety carry the greatest global burden of all mental disorders in terms of disability-adjusted life years, and as such, form a worldwide public health challenge [43].
Emotional problems have been associated with the onset of adolescence, which has been defined as the age range between 10 and 19 years [44]. Studies with younger or older participants were included if the age range overlapped with 10–19 years of age and the mean of the sample fell within this bracket. Emotional problems include clinical or sub-clinical symptoms of “panic disorder, generalized anxiety disorder (GAD), separation anxiety, social phobia, specific phobias, OCD and depression” [6, p. 12] and PTSD [6]. For the purposes of this scoping review, these problems did not require a formal diagnosis and could be based on self-report or self-evaluation measures, which included symptom-based descriptions of emotional problems (e.g., the Strengths and Difficulties Questionnaire “Emotional Difficulties” sub-scale) [45].
Concept
This review considered studies that explored self-management, self-care, and self-help in the context of adolescents with emotional problems.
It has been noted that there is no universally accepted definition of self-management [46], and some descriptions of self-management use the term interchangeably with self-care or self-help, despite some papers describing self-management and self-care as discrete concepts [47]. In a recent scoping review, self or community approaches were described as “non-professionally mediated” [13], and professionals were described as, “any person trained to use a treatment or intervention for the purposes of improving mental health or emotional wellbeing” [13]. This was the first attempt to group these concepts under a comprehensive umbrella [13]. However, the focus of the aforementioned review was on strategies in relation to anxiety and depression rather than emotional problems more broadly. This means that additional strategies, interventions, or techniques for emotional problems may have been missed.
One justification for an amalgamative term is the lack of clarity in the literature about which strategies or techniques specifically make up self-management, self-care, and self-help. For example, it has been argued that while self-care should be considered a preventative strategy, self-management should be employed to address the impact of a current difficulty or disease [47]. However, other studies acknowledge crossover between self-management and self-care strategies in mental health by creating overarching ways of describing these related techniques, such as “self or community approaches” [13].
Non-professionally mediated interventions are any kind of activity, intervention, or action a young person could engage in with the aim of improving their mental health without the need to involve a mental health professional [13]. However, self-initiated strategies introduced to a young person by a professional (e.g., breathing techniques) could also be considered to contain elements of self-management, self-care, or self-help, and therefore they merit further investigation in this review to identify any key similarities or differences. Additionally, how adolescents come to implement these strategies may be different depending on need, such as managing pre-existing long-term difficulties or stopping the re-emergence of mental health difficulties. Self or community approaches [13] and unguided self-help interventions [17] both reference the “self” and indicate a measure of agency which should also be researched further, specifically from the viewpoint of adolescents and their initiation of these strategies or techniques.
Therefore, clarity is needed here to ensure that interventions to improve self-management, self-help, or self-care are appropriate, targeted and needs-based, that they address intended mechanisms of change, and that they employ strategies which help to improve adolescents’ mental health. In addition, the efficacy of using these strategies for their intended purpose is difficult to measure without first understanding the concepts they stem from. This has implications for psychological measurement of self-management, self-care, and self-help amongst adolescents.
Context
The context of the literature in this scoping review includes research where self-management, self-care, or self-help strategies or techniques have been introduced to adolescents or can be located or accessed by them as methods for improving the symptoms of emotional problems. Specific contexts include specialist mental health settings where these strategies are proposed as alternatives or correlates to specialist mental health treatment; in schools or community-based settings; or within a young person’s own home as they find information about or access a self-management strategy on a computer, phone, or tablet. A key issue in this review was determining whether professionally-initiated help was guided or unguided. Studies were included if the strategy was taught by a professional or if it was discovered independently by a young person. However, studies were excluded if there was a professional involved in the administration of the self-management, self-care, or self-help strategy (e.g., guided self-help, therapist phone calls, etc.), as this type of help or support can be considered “guided” or “professionally-mediated” and is conceptually and functionally demarcated in the literature [13, 17]. For example, the Stressbusters computerized cognitive behavioral therapy (cCBT) intervention was not included in this scoping review, as a professional (in this case, a researcher|) provided support with using the program throughout the sessions [48]. However, in the same paper, adolescents were introduced to self-help websites by a professional as a control, which they went on to browse independently [48]. Therefore, the self-help websites control arm of this intervention was included in this scoping review [48].
Types of sources
This scoping review considered all quantitative, qualitative, economic, and mixed methods studies and evaluations, as well as systematic, scoping, and literature reviews, for inclusion with the aim of obtaining a comprehensive overview of the literature. Conference abstracts and presentations were not included, as evidence suggests that information contained in conference abstracts may not be dependable or adequate [49,50,51]. However, the authors of one relevant conference abstract were successfully queried to request any published literature related to the research questions of this scoping review. No additional literature was added to the review following this contact. Commentaries and opinion pieces were not included as they are not empirical studies. To capture the full range of the literature, grey and unpublished literature (e.g., empirical reports) were included and obtained by searching Mednar. Reference lists from seminal articles were searched for missing literature, and this did not yield any additional literature not already identified by the search.
Search strategy
An initial search was conducted using a selection of keywords on PsycINFO, Embase, and Medline using the Ovid platform. The text words in the title and abstract of these publications were analyzed along with any relevant keywords and index terms. After consulting with a university research librarian, additional keywords and index terms broadening this search were added resulting in a new list, which was used to undertake a second search through all chosen databases. This was done to ensure that an index article by Wolpert et al. [13] was found by the search. With the help of the research librarian, the search strategy was then translated from the Ovid platform databases to the bespoke Web of Science platform and CINAHL’s EBSCO platform. The reference lists of all studies from the second search which met the inclusion criteria for additional studies were reviewed, and appropriate studies were added to this review. Studies which were mentioned in systematic or scoping reviews but not picked up by the search were included for another round of review, resulting in 11 additional identified studies. The search strategy, including all identified keywords and index terms, was adapted for each included information source, and a second search was undertaken from 15th February to 22nd February 2021. The full search strategies are provided in Appendix 1.
Only studies published in English or with an accessible English translation were considered for this review. Additionally, only studies published from 1st January 2000 onward were included in this scoping review. This was for the following two reasons: (1) The NHS Plan, published in 2000, was the first major policy document in the UK to reference self-care in the context of managing chronic health conditions [15], and (2) due to changes in technology and understanding of e-health or digital health interventions around the millennium, which led to greater proliferation of health-related resources online [23].
The databases searched included PsycINFO, Medline and Embase (using the Ovid platform); Web of Science (using their bespoke platform); and CINAHL Plus (using the EBSCO platform). Mednar was searched for unpublished studies and grey literature. Websites targeting mental health for adolescents (e.g., https://headspace.org.au/, https://www.annafreud.org/on-my-mind/self-care/) were also searched for relevant literature. However, no additional empirical literature that met inclusion criteria was discovered following this website search.
Study selection
Following the search, a two-stage process of study selection was undertaken.
In stage one, all identified records were collated and uploaded into EndNote X9 and duplicates were removed. To maximize the limited availability and resources of the research team, the titles and abstracts of the first 20% of the literature identified as result of this search were independently screened by the first reviewer (RT) and the second reviewer (AM) to determine whether these data met the inclusion criteria of this scoping review. The interrater reliability between the reviewers was then calculated using the kappa statistic [52] and was found to be 0.87. This statistic demonstrates the extent to which two people assign the same value to the same variable in a review process, and it can range from -1 (no agreement) to + 1 (perfect agreement) [52]. The value 0.87 falls between 0.80 and 0.90, which is considered strong agreement [52]. Given this, the first reviewer continued to screen the remaining titles and abstracts.
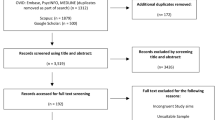
In stage two, following the conclusion of the title and abstract screening, full texts were retrieved. The second reviewer screened 10% of retrieved full texts, and their screening was compared with the first reviewer’s screening. All disagreements that arose between the reviewers at each stage of the selection process were resolved through discussion. The interrater reliability between the reviewers was again calculated using the kappa statistic and was found to be 0.62, indicating moderate agreement [52]. Any disagreements at this stage were resolved through discussion. The first reviewer screened the remaining full texts. Reasons for exclusion of full-text papers that did not meet the inclusion criteria were recorded and are reported in Fig. 1. The results of the search are reported in full in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram in Fig. 1 [38, 53].

Search results and study selection and inclusion process [53]
Data extraction
Data were extracted from the papers identified by the title and abstract screening by RT using a draft data extraction grid which was modified from a JBI data extraction tool to include categories relevant to the current scoping review [54]. This draft data extraction grid was submitted as part of the protocol for this scoping review [39]. To check that this tool worked as intended, the first and second reviewers piloted the grid by extracting data from the first five included papers (8.1% of the total) to check that the same data was extracted by each reviewer. This process resulted in small changes to the wording on the data extraction grid (e.g., adding more rows to detail specific methodologies and analytic techniques used, replacing “phenomena of interest” with a row naming the construct – self-help, self-care, or self-management —and another row describing the emotional problem addressed by this construct, adding a row for participant age standard deviation, and adding a row for limitations as stated by the authors). See Appendix 2 for the final extraction instrument that was used in this review. As the two reviewers extracted the same data and due to the research team’s resource constraints, the first reviewer extracted data from the remaining 57 papers.
Text was extracted from just before and after the point in each paper where self-help, self-care, or self-management was first mentioned. Authors of papers were contacted to request missing or additional data, where required. All contacted authors (n = 3) responded with the requested information, which included clarification on age range or mean and information about publications resulting from conference presentations.
Data analysis and presentation
To create this typology and the resulting Venn diagram, extracts from included texts referencing the concepts were uploaded into NVivo Version 12, where they were analyzed following the process for reflexive thematic analysis outlined by Braun and Clarke [55, 56]. This primarily inductive method follows six phases. Phase 1: The first reviewer became familiar with the data by reading and re-reading all extracts from included texts, facilitating reflection on and engagement with the data [56]. Phase 2: Initial codes were created and applied systematically across the dataset. This coding was organic and recursive, adhering to reflexive thematic analysis, and codes aimed to reflect important features of the data and were derived inductively (i.e., they were not limited by the research questions) [56]. Phase 3: These codes were condensed into overarching themes, with some of the codes becoming themes themselves. Themes were grouped according to conceptual overlap to allow for comparison of repeated themes across different concepts (as captured in Fig. 2). Phase 4: The themes were reviewed to determine if all coded extracts corresponded to the essence of the theme, as well as the entire dataset. At this stage, two additional authors involved in this review (DH and ES) reviewed the themes and their coded extracts to add an extra layer of reliability to this analysis. This was done by checking that the themes adequately reflected the totality of the extracts assigned to each theme. Phase 5: The themes were clearly defined and named by the first reviewer (RT). Phase 6: A report was produced, where themes were presented in a Venn diagram and a typology and discussed narratively alongside quotations derived from the coded abstracts [55].

Venn diagram showing similarities and differences between themes and related concepts
This report is presented in the “Review findings” section of this scoping review. In it, the similarities and differences in how self-management, self-care, and self-help are described in the context of adolescents with emotional problems is discussed narratively in alignment with the objectives and scope of this review, with quotations or examples of strategies relating to each description given where possible.
Results
Study inclusion
A diverse range of studies was included, covering both descriptive and experimental studies (e.g., qualitative and quantitative studies, clinical trials, population studies, and cohort studies). There were 6813 records whose titles and abstracts were screened for this review (see Fig. 1). Of these, 6572 were excluded as they were ineligible, resulting in 241 full-text articles being screened for inclusion. One hundred and ninety of these articles were excluded for the following reasons: not unguided (n = 63); age range too old or too young (n = 50); not an empirical study (n = 44); self-management, self-help, or self-care not mentioned (n = 19); and other (e.g., missed in an earlier screening, duplicate, etc. (n = 14). As many of the included studies at this phase were reviews which mentioned multiple self-management, self-help, or self-care studies (e.g., systematic reviews, metanalyses, etc.), an additional round of screening was conducted using the references cited in these reviews. From this, 69 additional full-text articles were identified and assessed for eligibility. Fifty-eight of these articles were excluded for the following reasons: self-management, self-care, or self-help not mentioned (n = 29); not unguided (n = 19); age range too old or too young (n = 5); not an empirical study (n = 4); and intervention is not for the purpose of self-management, self-help, or self-care of an emotional problem (n = 1). The remaining 62 records which met inclusion criteria were subjected to data extraction. The final included articles were composed of 20 quantitative studies, 14 systematic reviews, 10 qualitative studies, five review papers (review type was not specified), four book chapters, four mixed method studies, two dissertations, two meta-analyses, and one scoping review and systematic review.
See Fig. 1 for the results of this search and the details of the process used for article selection and inclusion in this scoping review [53].
Characteristics of included studies
The included articles showed wide geographic spread of high-income countries, primarily English-speaking, with participant representation spanning Australia [57], New Zealand [58], Canada [59], the UK [48], Ireland [60], the United States of America (US) [61], South Korea [62], and the Netherlands [63]. Articles included participants from both rural and urban areas, and several socially excluded or marginalized groups were featured — e.g., sexual minority youth [58], Latina adolescents [64], adolescents with visible physical differences [65], Mexican–American adolescents [66], individuals with autism spectrum disorder (ASD) [62], rural Australian young people [67], adolescent mothers [68], and LGBTQ + young people [69]. A wide range of ages (within the inclusion criteria) and ethnicities was present in the included articles.
Included studies referenced at least one of the key terms (self-management, self-help, or self-care) in the abstract or main body text (e.g., not only in the references) [13]. Most of the included articles referenced self-help (n = 51), followed by self-management (n = 17), and self-care (n = 6). In terms of multiple concepts, seven articles referenced self-management and self-help [70,71,72,73,74,75,76], two referenced self-care and self-help [13, 77], one referenced self-care and self-management [62], and one referenced self-care, self-help, and self-management [78].
Review findings
A total of 16 themes were identified from the reflexive thematic analysis of the introduction of or definition given for self-help, self-management, or self-care in included texts, and these are presented as a typology in Table 2 [36, 55, 56]. Themes are also displayed as a Venn diagram (see Fig. 2) to highlight the extent of the overlap between the descriptions of these concepts. A table of associated strategies was also produced (see Table 3), which links strategies to the concepts they were associated with in included texts. This typology and resulting Venn diagram were refined iteratively by the first author (RT) and another reviewer (ES) throughout the analytic process, and they are employed to describe how the results of this scoping review respond to the original review questions.
A total of 12 themes were derived from the analysis of the included texts. These themes are displayed in Fig. 2 as a Venn diagram and in Table 2. Themes that applied to multiple concepts are shown in the overlapping portions of the circles. The only theme that was common across self-management, self-help, and self-care was “Digitally available”. Themes contained in the non-overlapping sections are not necessarily unique aspects of these concepts, but they were those which diverged from the other concepts in the included text excerpts for this review. For example, “Looking after yourself” may not be unique to the concept of “self-care” in general, but it was unique to self-care in the analysis performed for the purposes of this review. The aim of displaying points of overlap and divergence is to demonstrate how these concepts, which have considerable conceptual and definitional overlap, are discussed in the existing literature around adolescents with emotional problems. This has been done with the goal of introducing clarity when discussing how these concepts and related strategies could be promoted to adolescents to improve emotional oblems.
The themes are organized in a typology by coverage categories (see Table 2 above) and are presented alongside illustrative quotes below. Associated strategies aligning with each concept are presented in Table 3 and discussed narratively in the text.
Self-help, self-care, and self-management
Theme 1: Digitally available
Many included articles (n = 28) mentioned that self-help can be available on a digital platform, and they referred to related self-help strategies or interventions using a variety of different terms. These included the following: technology-empowered CBT (tCBT) programs [79], e.g., any CBT-based interventions involving technology, such as a telephone or computer; digital mental health interventions [80]; web-, computer-, online- or internet-based interventions [57, 58, 71, 72, 74, 81,82,83,84,85,86,87,88,89]; websites [76, 90]; e-therapy programs [88]; CD-ROMS or DVDs [74, 76, 83, 91]; ecounselling [90]; applications or “apps” [74, 79, 89, 92]; independent self-help multimedia therapy programs [91]; telemental health (TMH) [89]; and cCBT [58, 79, 93,94,95]. See Table 3 for further information relating to these interventions or strategies.
Similarly, self-management was linked to digitally available interventions or strategies, such as computer programs or internet-based interventions, in two articles. For example, one study described the need for an internet-based depression self-management intervention to support adolescent mothers living in rural locations [68]. The other described a CBT-based self-management intervention, “Breathe”, for adolescents experiencing anxiety that was accessible over the internet [59]. Likewise, self-care was linked with digitally available strategies such as connecting with others on the Internet and finding information or informal help for mental health problems online [69].
Self-help and self-care
Theme 2: Monitoring, managing, and preventing symptoms
Self-help was described by multiple included texts (n = 5) as relating to the monitoring, management, and prevention of symptoms of a mental health problem. Similarly, several included studies (n = 4) explained that self-care involved a process of monitoring, managing, and preventing symptoms related to one’s health, either mental or physical.
Self-help and self-management
Theme 3: Associated with clinical treatments or interventions
Several included articles (n = 10) mentioned interventions, clinical treatments, or clinical skills in relation to self-help. Types of interventions, treatments, and skills included bibliotherapy or computer-based interventions [77, 96, 97], unguided or guided self-help interventions [17], computer-based interventions or apps [67, 70, 98], standalone self-help interventions [98], CBT techniques [92, 98], dialectical behavioral therapy (DBT) skills [98], gamified therapeutic tools [67], exposure and response prevention [98], and cognitive restructuring [96]. See Table 3 for further information about these self-help strategies or techniques.
Similarly to self-help, self-management was often associated with clinical treatments or interventions in included texts (n = 7). This included self-management in terms of adherence to a treatment regimen, in relation to treatment seeking and service utilization, and as part of a psychosocial or self-help intervention. For example:
“[I]ndividuals may benefit from psychosocial interventions that promote self-management skills to tackle stigmatisation and body dissatisfaction (Bessell and Moss, 2007; Muftin and Thompson, 2013)” [66, p. 2].
Theme 4: Can involve social elements
Despite the emphasis of the “self” inherent to the term “self-help”, two articles explained that self-help interventions can be group-based, include parents or carers, or involve wider social support.
Aligning with self-help, self-management was also described by two included texts in relation to social interaction with others, including peer or social support. For example, MoodHwb, a digital intervention in both English and Welsh for adolescents with depression, “aims to promote self help, help-seeking where appropriate, and social support” [71, p. 2].
Self-care and self-management
Theme 5: Daily activities to improve health
Self-management was described in three included texts as a daily or regular activity which was performed with the intention of improving ones’ health, either mental or physical.
Self-care was also linked to activities which were regularly performed to improve one’s health, such as rest, diet, and exercise.
“Throughout treatment, depressive mood is targeted via activities that bring pleasure or mastery, by enhancing relationship skills and interpersonal connectedness, and via daily self-care (e.g., rest, diet, exercise)” [78, p. 66].
Self-care only
Theme 6: Looking after yourself
One included text described self-care as looking after one’s physical self by engaging in safe sexual practices and avoiding risky situations.
“Engage in physical self-care. Avoid “high-risk” activities such as drug use, risky sexual activities, antisocial delinquent activities, and the like” [100, p. 221].
Theme 7: Seeking professional help when needed
The same article explained that self-care could include seeking help when it was needed, and it linked this with “emotional self-care.”
“Engage in emotional self-care (seek help when needed, use relaxation, mindfulness, and meditation procedures, and seek opportunities to experience positive emotions of empathy, compassion, forgiveness, joy, gratitude, and the like)” [100, p. 221].
Self-help only
Theme 8: Can be static (e.g., website or bibliotherapy)
Self-help was often described in included articles (n = 12) as something static or unchanging, which did not involve tailoring or adolescents’ input to be used effectively for self-help. This involved self-help books which participants read on their own [97], self-help websites with information about mental health or psychoeducation [90], and CD-ROMS or DVDs delivering CCBT [83].
Several (n = 4) of these static self-help interventions served as a control alongside a more interactive intervention, or they were described as something that could be used alongside therapy with a professional.
“We aimed to assess the feasibility of delivering an RCT comparing Stressbusters (CCBT) with an attention control (accessing low mood self-help websites) for adolescents with low mood/depression” [48, p. 2].
Theme 9: Reduces stigma, cost, and burden, and increases access
Several included texts (n = 6) argued that self-help has the capacity to reduce stigma, lower costs, and lighten the burden for young people with mental health difficulties. This was linked, in turn, to increased access to mental health support, particularly for adolescents who may not be willing or able to attend specialist services. For example:
“Young people are reluctant to seek professional mental health care. Self-help therapies may, therefore, be critical to effectively intervening to address young people’s anxiety without the need for professional service use” [74, p. 25].
Theme 10: Tailored and engaging
Self-help was generally described by multiple included texts (n = 7) as personalized, tailored, and particularly engaging to adolescents in this regard. This engagement could be driven through personalizing content according to participants’ preferences and needs, e.g., a program tailored to adolescents’ developmental needs,[100] or by delivering an intervention in a format that might be preferable to adolescents, e.g., using a video game format to appeal to young men [63].
However, one included study noted that despite efforts to tailor their self-help intervention for a target audience, adherence to the programme was poor. These authors acknowledged that this was often the case for self-help interventions [75]. Previous research has suggested that various pre-intervention factors predict better self-help programme adherence, such as being of a younger age, living in a rural location, having higher depressive symptoms, and having higher self-esteem [101].
Self-management only
Theme 11: Agency and empowerment
Some included texts (n = 3) described self-management interventions in relation to developing adolescents’ capacity, competency, and agency in self-management.
One internet-based depression intervention for improving rates of treatment for rural adolescent mothers focused on the “strong propensity for self-reliance and a preference for self-managing health problems in rural populations” [69, p. 4]. This was used as a justification for developing an intervention targeting rural adolescent mothers, despite comparability in the rates of mental ill health in rural and urban populations [68].
Another intervention, “Breathe”, focused on the importance of empowering adolescents to self-manage rather than signposting them to another intervention. This internet-based cognitive behavioral therapy program specifically aimed to “[help] adolescents develop their capacity and competency for self-management rather than redirecting them to alternative resources” [73, p. 16].
Theme 12: Learning from feedback and problem-solving
Several included texts (n = 4) described how self-management involved a process of problem solving and learning from feedback. This was evident in mobile interventions which promoted self-awareness, monitored symptoms, and provided feedback [75], as well as in therapeutic games using varied motivators, realistic learning scenarios, and incorporated feedback to improve self-management [102].
Strategies or interventions
Table 3 details the proposed strategies in included articles for the following concepts: self-care, self-help, and self-management. Strategies appeared particularly sparse for self-care, with only three of six included articles referencing any associated strategies. One digital self-care strategy was identified: Rainbow SPARX [69]. Rainbow SPARX is a computerized cognitive behavioral therapy program developed for lesbian, gay, bisexual, and transgender young people, as well as other young people with diverse sexual orientation or gender identity (LGBT) [69]. In this article, self-care was described in relation to the Internet and psychosocial support for mental health problems [69]. The other three included articles in this scoping review that referenced self-care either did so in relation to another concepts [62, 78], e.g., self-care in the context of a self-help intervention for young people with type 1 diabetes [78], or in relation to professionally-mediated strategies only [13].
In contrast, self-help was associated with the largest number of strategies or techniques, ranging from personal, individual, or lifestyle-oriented strategies, e.g., “Eat a healthy, balanced diet” [60], “Work through on one’s own” [103], to strategies involving peers or family members, e.g., “Spending time with friends and family” [66], “Ask a trusted friend or relative to help you get out and about or do activities” [60]. A wealth of digital interventions and strategies were associated with self-help in the included literature. Self-help interventions that primarily targeted depression or low mood formed the majority of the digital strategies or interventions, e.g., SPARX [63, 67, 93, 94], Rainbow SPARX [58], Blues Blaster website [86], low mood self-help websites [48], The Journey [100], MEMO [75], and MoodHwb [70].
Self-management was also associated with multiple strategies or interventions, including individual strategies, such as “Reading”, “Sleep”, or “Watching TV” [64], those involving others, such as “Peer relationships or involving others in management” [61, 64, 104], and digital strategies or interventions, such as FACE IT, an online psychosocial intervention designed to help young people self-manage anxiety associated with having a visible physical difference [65].
There was significant overlap across the strategies and interventions associated with self-care, self-help, and self-management in this review. For example, the following strategies or interventions spanned all three terms: sleep or rest [60, 64, 77, 103], talking to others such as peers, family, or a professional when needed [60, 61, 64, 66, 99, 103, 104], activities involving physical movement [64, 66, 77], and digital strategies [68, 69, 105].
Definitions of concepts
Most articles in this scoping review did not include an identifiable definition of the concept that was being discussed. Only self-help and self-management were explicitly defined, with five definitions for self-help and one definition for self-management. See Table 4 below for these definitions.
As is evident in Table 4, most included articles (n = 56, 90.3%) did not include an explicit definition of the concept being discussed. This was particularly the case for self-care, for which there were no explicit definitions, and self-management, for which there was only one. For self-help, there were five explicit definitions in five included articles. These varied widely, with self-help being operationalized in terms of evidence-based treatments delivered through technology, actions taken by the individual, group meetings, treatments which could be used without professional consultation, and the delivery of computerized CBT. While there are some commonalities across these definitions (e.g., not involving a professional, digital or technology-based delivery), the variation across included articles and the lack of consensus around a particular definition suggests that self-help may encompass a spectrum of strategies or interventions across the literature concerning adolescents with emotional problems.
Discussion
This scoping review aimed to answer the following two research questions: (1) “How are the concepts of self-management, self-care, and self-help described in the context of adolescents with emotional problems?”, and (2) “What strategies or techniques have been proposed to facilitate self-management, self-care, and self-help in adolescents with emotional problems?” A search of the literature yielded 62 empirical articles that met inclusion criteria for this scoping review. Text excerpts from included articles were analyzed using reflexive thematic analysis [55, 56]. This resulted in 12 distinct themes which were presented as a typology to address the first research question (see Table 2). Areas of conceptual overlap in these themes were displayed visually as a Venn diagram (see Fig. 2). In addition, the definitions of self-management, self-help, and self-care (where present in the included literature) were presented (see Table 4). These are explored in terms of their points of convergence and divergence and in relation to relevant literature below. To answer the second research question, strategies or techniques which were associated with self-management, self-help, or self-care were described in Table 3. The themes which overlapped between multiple concepts are discussed in the context of relevant literature below.
Definitions of concepts and themes
There was considerable overlap between the definitions of self-help. For instance, three definitions specifically referenced technological or digitally available interventions, such as computerized cognitive behavioral therapy [105], the provision of treatment through technology [106], and the use of the internet in self-help [74]. However, two definitions did not mention technology or digital availability at all and instead focused on the individual aspects of self-help, such as the actions an individual can take to prevent or manage a condition [66] or treatments that can be used by an individual without consulting a healthcare professional [107]. The sole definition provided for self-management appeared similar to one of the definitions given for self-help, with both emphasizing the role of the individual in the daily steps or actions taken to manage the impact of a health condition [64, 66].
This lack of explicit definitions is not surprising given the confusion and overlap around these concepts in the literature more generally. It is possible that the lack of definitions for “self-care” indicates the usage of this term is more colloquial rather than theory- or evidence-based. This aligns with the findings in this review that self-management and self-help were “Associated with clinical treatments or interventions” (Theme 3, while self-care was not. A recent study supports this assertion, suggesting that self-care research lacks a strong evidence base partly due to the absence of a clear definition of the concept [25].
Additionally, many studies were excluded from this scoping review that focused on self-care for adolescents with diabetes (e.g., [108]). While not within the scope of the review, it is possible that self-care is more clearly defined in the context of diabetes, whilst it requires further investigation and elucidation within the context of adolescents with emotional problems. This clearer definition in diabetes research could be due to self-care historically forming an important part of the transition of disease management tasks (such as glucose monitoring and insulin administration) from parents or carers to adolescents [109]. Other research suggests that there are seven self-care behaviors that have been linked with better outcomes for people with diabetes: “healthy eating, being active, monitoring, taking medication, problem solving, healthy coping, and reducing risks” [110 p. 446].
One theme, “Digitally available”, was related to self-management, self-help, and self-care. Indeed, the digital availability of interventions was a common feature across these concepts and may be indicative of the interests of adolescents in terms of help-seeking. There is evidence that adolescents use the Internet to seek help for mental health difficulties, with adolescents reporting multiple benefits of online help-seeking, including anonymity, ease of access, ability to connect with others, inclusivity, immediacy, and privacy [111]. Another implicitly common thread (based on the methodology of this scoping review) was that self-management, self-help, and self-care did not require professional involvement. While related strategies or techniques could involve professionals, included articles explained that they could be done without professional involvement. Wolpert et al. highlight that due to the high and increasing numbers of young people with mental health problems, simply hiring more professionals to provide treatment is not a realistic solution [13]. Therefore, these authors argue it is important to consider alternative strategies (like self-management, self-help, and self-care) that can reach more people, and potentially help those for whom specialist support is not the only or best course of action [13].
Self-help and self-care overlapped on one theme: “Monitoring, managing, and preventing symptoms.” This aligns with the literature around both self-help and self-care in young people. For example, recent research during the Covid-19 pandemic suggested that a self-help intervention was successful in reducing the symptoms of anxiety in university students by helping them to monitor their emotions and manage stress [112]. Likewise, in a recent study of a program aiming to prevent serious mental health difficulties amongst adolescents in England, self-care strategies such as deep breathing techniques and stress balls were described by adolescents as helpful in managing difficult emotions, such as anger or stress [19]. The only specific digital strategy associated with self-care in this scoping review, Rainbow SPARX [58, 93], was also associated with self-help (see Table 3). Rainbow SPARX is a computerized cognitive behavioral therapy program designed for sexual minority youth which resulted in a significant decrease in depressive symptoms for LGBTQ+ adolescents [58].
Self-help and self-management overlapped across the following two themes: “Associated with clinical treatments or interventions” and “Can involve social elements.” Self-help peer support programs have been described as an essential source of support for young people with mental health problems [113], and research suggests that peers, family, and social groups influence adolescents’ capacity to self-manage and seek treatment for their depression, e.g., in a recent study of Latina adolescents [61]. This was highlighted in associated strategies in included articles for self-management, specifically in “Peer relationships or involving others in management” (e.g., friends, parents, or mainstream authorities) [61, 64, 104]. This was also the case for self-help, specifically in “Ask a trusted friend or relative to help you get out and about or do activities” [60], “Be with friends” [103], “Let family and friends know how you are feeling so that they are aware of what you are going through” [60], “Spending time with friends and family” [66], and “Talk problems or feelings over with someone who is supportive and caring” [60]. In general, the evidence base appears to be larger for self-help and self-management than it is for self-care as applied to adolescents with emotional problems, which may explain in part why self-help and self-management were predominately associated with clinical treatments or interventions. This is evidenced by the existence of systematic reviews which have been conducted regarding self-help (e.g., [73]) and self-management (e.g., [114]) for mental health conditions amongst adolescents, while no such systematic reviews exist for self-care (to the authors’ knowledge).
Finally, self-care and self-management overlapped across one theme: “Daily activities to improve health”. Previous research has equated self-care with daily life [19] or referred to daily self-care [115] amongst adolescents with a health condition. However, Stapley et al. [19] focused on how self-care strategies are used to cope with the stressors of daily life, rather than how self-care is used specifically to manage emotional problems. The findings from the current review add to this, as they suggest that a variety of self-care strategies can be employed to improve symptoms of emotional problems on a regular basis. Though primarily discussed in the context of chronic illness, daily activities to improve health are also mentioned in the literature around self-management in terms of daily disease self-management regimens [18] and daily medication adherence [116]. The current review supports these findings, as self-management was described in one included article as the “daily steps that individuals take to minimize the impact of a health condition on their health status [47]” [64, p. 18], and other included articles described daily self-management strategies such as mood tracking [70] and daily videos or text messages with CBT-related key messages delivered automatically via mobile phone [75].
Strategies and techniques
Many of the interventions or strategies identified for self-help, self-management, and self-care in this review (see Table 3) overlapped with the “self or community approaches” for children and young people identified by Wolpert et al. [13]. Some examples of overlap or similarity are: “Goal setting” [13] overlaps with “Reward yourself for reaching a small goal” [60], “Apps delivering self-help strategies” [13] overlaps with “Self-help ICBT programs” [57], “Sleep” [13] is identical to “Sleep” [60, 103], and “Playing a therapeutic online or computer-based game” [13] overlaps with “Rainbow SPARX” [69]. Notably, there was overlap across self-management, self-help, and self-care, suggesting that strategies associated with these terms might be more meaningfully grouped under a label such as “self or community approaches”, and do not necessarily need to be separated by concept [13].
It is clear from the findings of this scoping review that self-help is the most frequently discussed concept (when compared with self-management and self-care) in the literature addressing adolescents with emotional problems. There are several potential reasons for this. First of all, self-help has the largest evidence base of the three concepts. This could be owing to the proliferation of e-health resources over the past two decades, which has increased steadily alongside the dramatic growth of the Internet and smartphone usage [23]. Recently, the growing importance of digital self-help and other online support resources has been illuminated during the Covid-19 pandemic, which led to reported increases in adolescents’ use of digital interventions for mental health support [117, 118]. Secondly, self-help may be a preferred term due to a historic precedent set by the profitable “self-help” industry; since the coining of the term “self-help” by Samuel Smiles in 1859 [119], the self-help industry now grosses a yearly estimated 10 billion dollars in the US [28]. Therefore, familiarity with the term may drive its colloquial usage, and this is supported by the self-help MeSH term being added in 1979, whilst self-care and self-management were added in 1981 and 2018, respectively [32]. Finally, self-help may lend itself better to therapeutic intervention development, as the focus may be on actively “helping” or improving an individual’s illness-related behavior (rather than “managing” or “caring” in relation to behavior) through the implementation of behavior change techniques [120].
Limitations and strengths
A strength of this scoping review is its consideration of all forms of empirical studies, as well as unpublished or grey literature. It is therefore likely that this review represents a comprehensive map of the ways in which self-help, self-care, and self-management are discussed in the current literature around adolescents with emotional problems. An additional strength was the reliability of the analysis performed in this review, as it was checked by two additional members of the research team. The screening for this review was also strengthened by the high interrater reliability between the first reviewer (RT) and the second reviewer (AM).
There are some limitations to this research. Firstly, it is important to consider these findings as a preliminary framework for understanding overlap between the concepts of self-help, self-care, and self-management. This framework does not aim to fully operationalize the concepts themselves, but instead highlights how they are currently being discussed in the existing literature around adolescents with emotional problems. There is far more literature for self-help than self-management or self-care, which appear underrepresented in the literature around adolescents with emotional problems. Therefore, a large gap still exists in our understanding of self-management and self-care for adolescents with emotional problems. Additionally, attempts to separate or elucidate these concepts in this scoping review could have been hampered by the jingle-jangle fallacy, e.g., by implying through differing terminology that the terms are conceptually distinct when they may all be describing the same idea [34]. This fallacy suggests that two or more concepts in psychology with the same or similar-sounding names might mean different things, or vice versa [34]. There are also cultural differences that may impact on both the role and definitions of all three concepts which should be explored in future research. For example, research shows that understanding of mental health varies across cultures, impacting factors such as help-seeking, use of resources, and perceived stigma [121]. Finally, caution should be taken when referring to research around self-care specifically, as there appears to be very little literature discussing self-care amongst adolescents with emotional problems.
Conclusions
Self-management, self-help, and self-care are all concepts which have been discussed in the literature around adolescents with emotional problems. There is considerable overlap in both the ways in which these concepts are discussed in the literature and the strategies or approaches which are proposed in relation to them. Previous research has suggested that these strategies should be grouped under an inclusive umbrella, such as “self or community approaches” [13]. This assertion is supported by the findings of this scoping review, as there is enough similarity in the literature to merit these strategies or approaches being grouped together. Whilst self-management, self-help, and self-care may describe conceptually different ideas, the strategies or approaches to facilitate them appear to be similar across multiple domains.
As no research has been conducted previously to draw together this literature, this scoping review has important implications for policy and intervention development for adolescents’ self-management, self-help, and self-care of emotional problems, as it provides clarity on the similarities and differences between how these concepts are discussed, and the strategies associated with each of these concepts in the relevant literature. Despite this, more research is needed specifically for self-management, self-help, and self-care amongst marginalized groups, such as LGBTQ + young people, as these groups may have the highest unmet need for mental health support and could benefit from online or digital approaches [122, 123].
Implications for research
As there is evidence that increased discrimination experienced during the Covid-19 pandemic has had particularly negative effects on the mental health of marginalized groups like LGBTQ + young people [124], future research should investigate how self-help (as well as self-management and self-care) strategies and interventions can help these young people. Promising evidence for the development of interventions targeting depression amongst LGBTQ + young people were discussed in this scoping review [58, 69]. However, as these were only two studies that took place in New Zealand and the UK, far more research is needed on a global scale in this area.
The results of this review reveal the lack of research regarding self-management, self-help, and self-care amongst young people from marginalized groups who face emotional problems. From the included articles, there is evidence that the needs and preferences of these groups may be influenced by intersectional factors relating to ethnicity, sexual orientation, gender identity, and class (e.g., [67, 69]).
Data availability
All data for this review is held by the first author (RT).
References
Vizard T, Sadler K, Ford T, Newlove-Delgado T, McManus S, Marcheselli F, Davis J, Williams T, Leach C, Mandalia D, Cartwright C (2020) Mental health of children and young people in England, 2020. NHS Digital. https://files.digital.nhs.uk/CB/C41981/mhcyp_2020_rep.pdf. Accessed 13 Nov 2022
NHS Digital (2018) Mental health of children and young people in England, 2017 - summary of key findings. https://files.digital.nhs.uk/A6/EA7D58/MHCYP%202017%20Summary.pdf. Accessed 13 Nov 2022
NHS Digital (2020) Mental health of children and young people in England, 2020 - wave 1 follow up to the 2017 survey. https://digital.nhs.uk/data-and-information/publications/statistical/mental-health-of-children-and-young-people-in-england/2020-wave-1-follow-up. Accessed 13 Nov 2022
NHS Digital (2021) Mental health of children and young people in England 2021 - wave 2 follow up to the 2017 survey. https://digital.nhs.uk/data-and-information/publications/statistical/mental-health-of-children-and-young-people-in-england/2021-follow-up-to-the-2017-survey#chapter-index. Accessed 13 Nov 2022
Dekker MC, Ferdinand RF, Van Lang NDJ, Bongers IL, Van Der Ende J, Verhulst FC (2007) Developmental trajectories of depressive symptoms from early childhood to late adolescence: gender differences and adult outcome. J Child Psychol Psychiatry 48(7):657–666. https://doi.org/10.1111/j.1469-7610.2007.01742.x
Ogundele MO (2018) Behavioural and emotional disorders in childhood: a brief overview for paediatricians. World J Clin Pediatr 7(1):9–26. https://doi.org/10.5409/wjcp.v7.i1.9
Children’s Commissioner (2022) Children’s mental health services 2020/21. https://www.childrenscommissioner.gov.uk/report/briefing-on-childrens-mental-health-services-2020-2021/. Accessed 10 May 2022
Moore A, Gammie J (2018) Revealed: hundreds of children wait more than a year for specialist help. Health Serv J. https://www.hsj.co.uk/quality-and-performance/revealed-hundreds-of-children-wait-more-than-a-year-for-specialist-help/7023232.article. Accessed 13 Nov 2022
Edbrooke-Childs J, Deighton J (2020) Problem severity and waiting times for young people accessing mental health services. BJPsych Open 6(6):e118. https://doi.org/10.1192/bjo.2020.103
Crenna-Jennings W, Hutchinson J (2020) Access to child and adolescent mental health services in 2019. Education Policy Institute. https://epi.org.uk/publications-and-research/access-to-child-and-adolescent-mental-health-services-in-2019/. Accessed 9 May 2022
Wolpert M, Vostanis P, Young S, Clark B, Davies R, Fleming I, Howey L, Howley P, Macdougall A, Martin P, Martin T, Payne C, Ritchie B, Senior R, York A, Whale A (2015) Child and adolescent mental health services payment system project: Final Report. CAMHS Press. https://www.ucl.ac.uk/evidence-based-practice-unit/sites/evidence-based-practice-unit/files/migrated-files/CAMHS_Payment_System_Project_-_Final_Report.pdf. Accessed 18 Dec 2022
Wolpert M, Harris R, Hodges S, Fuggle P, James R, Wiener A, McKenna C, Law D, York A, Jones M, Fonagy P, Fleming I, Munk S (2017) THRIVE elaborated. CAMHS Press. https://www.annafreud.org/media/4817/thrive-elaborated-2nd-edition.pdf. Accessed 13 May 2022
Wolpert M, Dalzell K, Ullman R, Garland L, Cortina M, Hayes D, Patalay P, Law D (2019) Strategies not accompanied by a mental health professional to address anxiety and depression in children and young people: a scoping review of range and a systematic review of effectiveness. The Lancet Psychiatry 6(1):46–60. https://doi.org/10.1016/S2215-0366(18)30465-6
National Institute for Health and Care Excellence (2019) Depression in children and young people: identification and management (NICE quality standard no. 134). https://www.nice.org.uk/guidance/ng134. Accessed 13 Nov 2022
Department of Health (2000) The NHS plan: a plan for investment, a plan for reform. https://webarchive.nationalarchives.gov.uk/20121102184216/http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4002960. Accessed 13 Nov 2022
de Silva D (2011) Helping people help themselves: a review of the evidence considering whether it is worthwhile to support self-management. The Health Foundation. https://www.health.org.uk/sites/default/files/HelpingPeopleHelpThemselves.pdf. Accessed 11 May 2020
Bennett SD, Cuijpers P, Ebert DD, McKenzie Smith M, Coughtrey AE, Heyman I, Manzotti G, Shafran R (2019) Practitioner Review: Unguided and guided self-help interventions for common mental health disorders in children and adolescents: a systematic review and meta-analysis. J Child Psychol Psychiatry 60(8):828–847. https://doi.org/10.1111/jcpp.13010
Lerch MF, Thrane SE (2019) Adolescents with chronic illness and the transition to self-management: a systematic review. J Adolesc 72:152–161. https://doi.org/10.1016/j.adolescence.2019.02.010
Stapley E, Demkowicz O, Eisenstadt M, Wolpert M, Deighton J (2019) Coping with the stresses of daily life in England: a qualitative study of self-care strategies and social and professional support in early adolescence. The Journal of Early Adolescence 40(5):605–632. https://doi.org/10.1177/0272431619858420
Kooth plc (2021) Kooth Pulse 2021: Identifying issues and collaborating to enable positive mental health for all. https://explore.kooth.com/wp-content/uploads/2021/05/Kooth-Pulse-2021-Report.pdf. Accessed 8 February 2022
Headspace (2022) About Headspace. https://www.headspace.com/about-us. Accessed 13 May 2022
Calm Harm (2022) About Calm Harm. https://calmharm.co.uk/. Accessed 13 May 2022
Eysenbach G (2001) What is e-health? J Med Internet Res 3 (2):e20. doi:https://doi.org/10.2196/jmir.3.2.e20
Fergie G, Hunt K, Hilton S (2013) What young people want from health-related online resources: a focus group study. J Youth Stud 16(5):579–596. https://doi.org/10.1080/13676261.2012.744811
Jaarsma T, Strömberg A, Dunbar SB, Fitzsimons D, Lee C, Middleton S, Vellone E, Freedland KE, Riegel B (2020) Self-care research: how to grow the evidence base? Int J Nursing Stud. https://doi.org/10.1016/j.ijnurstu.2020.103555
Brijnath B-A (1982) Josefine (2016) “I’m running my depression:” self-management of depression in neoliberal Australia. Soc Sci Med 152:1–8. https://doi.org/10.1016/j.socscimed.2016.01.022
Bergsma A (2008) Do self-help books help? J Happiness Stud 9(3):341–360. https://doi.org/10.1007/s10902-006-9041-2
Harwood TM, L’Abate L (2010) Self-help in mental health: a critical review. Springer Science + Business Media, New York, NY, US. https://doi.org/10.1007/978-1-4419-1099-8
Wolpert M, Harris R, Hodges S, Fuggle P, James R, Wiener A, McKenna C, Law D, York A, Jones M, Fonagy P, Fleming I, Munk S (2019) THRIVE framework for system change. http://implementingthrive.org/wp-content/uploads/2019/03/THRIVE-Framework-for-system-change-2019.pdf. Accessed 30 July 2020
Fonagy P, Cottrell D, Phillips J, Bevington D, Glaser D, Allison E (2015) What works for whom?: a critical review of treatments for children and adolescents, 2nd edn. The Guilford Press, New York, New York
Hayes D, Edbrooke-Childs J, Town R, Wolpert M, Midgley N (2020) Barriers and facilitators to shared decision-making in child and youth mental health: exploring young person and parent perspectives using the theoretical domains framework. Couns Psychother Res 20(1):57–67. https://doi.org/10.1002/capr.12257
National center for biotechnology information (2020) MeSH. https://www.ncbi.nlm.nih.gov/mesh/
Abrines-Jaume N, Midgley N, Hopkins K, Hoffman J, Martin K, Law D, Wolpert M (2016) A qualitative analysis of implementing shared decision making in child and adolescent mental health services in the United Kingdom: stages and facilitators. Clin Child Psychol Psychiatry 21(1):19–31. https://doi.org/10.1177/1359104514547596
Block J (1995) A contrarian view of the five-factor approach to personality description. Psychol Bull 117(2):187–215. https://doi.org/10.1037/0033-2909.117.2.187
Marsh HW, Pekrun R, Parker PD, Murayama K, Guo J, Dicke T, Arens AK (2019) The murky distinction between self-concept and self-efficacy: beware of lurking jingle-jangle fallacies. J Educ Psychol 111(2):331–353. https://doi.org/10.1037/edu0000281
Mandara J (2003) The typological approach in child and family psychology: a review of theory, methods, and research. Clin Child Fam Psychol Rev 6(2):129–146. https://doi.org/10.1023/A:1023734627624
Peters MDJ, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB (2015) Guidance for conducting systematic scoping reviews. Int J Evidence-Based Healthcare 13(3):12. https://doi.org/10.1097/XEB.0000000000000050
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, Moher D, Peters MDJ, Horsley T, Weeks L, Hempel S, Akl EA, Chang C, McGowan J, Stewart L, Hartling L, Aldcroft A, Wilson MG, Garritty C, Lewin S, Godfrey CM, Macdonald MT, Langlois EV, Soares-Weiser K, Moriarty J, Clifford T, Tunçalp Ö, Straus SE (2018) PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 169(7):467–473. https://doi.org/10.7326/M18-0850
Town R, Hayes D, Fonagy P, Stapley E (2021) Self-management, self-care, and self-help in adolescents with emotional problems: a scoping review protocol. JBI Evid Synth 19(9):2373–2381. https://doi.org/10.11124/jbies-20-00224
Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E (2018) Systematic review or scoping review? guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol 18(1):143. https://doi.org/10.1186/s12874-018-0611-x
Armstrong R, Hall BJ, Doyle J, Waters E (2011) ‘Scoping the scope’ of a cochrane review. J Public Health 33(1):147–150. https://doi.org/10.1093/pubmed/fdr015
World Health Organization (2017) Depression and other common mental disorders: global health estimates. https://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf. Accessed 8 Dec 2022
Rehm J, Shield KD (2019) Global burden of disease and the impact of mental and addictive disorders. Curr Psychiatry Rep 21(2):10. https://doi.org/10.1007/s11920-019-0997-0
Age limits and adolescents (2003) Paediatr Child Health 8 (9) 577–578 https://doi.org/10.1093/pch/8.9.577
Goodman R (2001) Psychometric properties of the strengths and difficulties questionnaire. J Am Acad Child Adolesc Psychiatry 40(11):1337–1345. https://doi.org/10.1097/00004583-200111000-00015
Barlow J, Wright C, Sheasby J, Turner A (2002) Self-management approaches for people with chronic conditions: a review. Patient Educ Couns 48(2):177–187. https://doi.org/10.1016/S0738-3991(02)00032-0
Clark NM, Becker MH, Janz NK, Lorig K, Rakowski W, Anderson L (1991) Self-management of chronic disease by older adults: a review and questions for research. J Aging Health 3(1):3–27. https://doi.org/10.1177/089826439100300101
Wright B, Tindall L, Littlewood E, Allgar V, Abeles P, Trépel D, Ali S (2017) Computerised cognitive–behavioural therapy for depression in adolescents: feasibility results and 4-month outcomes of a UK randomised controlled trial. BMJ Open 7(1):e012834. https://doi.org/10.1136/bmjopen-2016-012834
Van Driel ML, De Sutter A, De Maeseneer J, Christiaens T (2009) Searching for unpublished trials in Cochrane reviews may not be worth the effort. J Clin Epidemiol 62(8):838–844. https://doi.org/10.1016/j.jclinepi.2008.09.010
Hopewell S, Clarke M, Askie L (2006) Reporting of trials presented in conference abstracts needs to be improved. J Clin Epidemiol 59(7):681–684. https://doi.org/10.1016/j.jclinepi.2005.09.016
Hartling L, Featherstone R, Nuspl M, Shave K, Dryden DM, Vandermeer B (2017) Grey literature in systematic reviews: a cross-sectional study of the contribution of non-English reports, unpublished studies and dissertations to the results of meta-analyses in child-relevant reviews. BMC Med Res Methodol 17(1):1–11. https://doi.org/10.1186/s12874-017-0347-z
McHugh ML (2012) Interrater reliability: the kappa statistic. Biochem Med (Zagreb) 22(3):276–282. https://pubmed.ncbi.nlm.nih.gov/23092060
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. https://doi.org/10.1136/bmj.n71
Peters M, Godfrey C, McInerney P, Munn Z, Tricco A, Khalil H (2020) JBI manual for evidence synthesis. JBI. https://doi.org/10.46658/JBIMES-20-12
Braun V, Clarke V (2006) Using thematic analysis in psychology. Qual Res Psychol 3(2):77–101. https://doi.org/10.1191/1478088706qp063oa
Braun V, Clarke V (2019) Reflecting on reflexive thematic analysis. Qualitative Res Sport, Exercise Health 11(4):589–597. https://doi.org/10.1080/2159676X.2019.1628806
Spence SH, March S, Donovan CL (2019) Social support as a predictor of treatment adherence and response in an open-access, self-help, internet-delivered cognitive behavior therapy program for child and adolescent anxiety. Internet Interventions. https://doi.org/10.1016/j.invent.2019.100268
Lucassen MFG, Merry SN, Hatcher S, Frampton CMA (2015) Rainbow SPARX: a novel approach to addressing depression in sexual minority youth. Cogn Behav Pract 22(2):203–216. https://doi.org/10.1016/j.cbpra.2013.12.008
O’Connor K, Bagnell A, McGrath P, Wozney L, Radomski A, Rosychuk RJ, Curtis S, Jabbour M, Fitzpatrick E, Johnson DW, Ohinmaa A, Joyce A, Newton A (2020) An internet-based cognitive behavioral program for adolescents with anxiety: pilot randomized controlled trial. JMIR Ment Health 7(7):e13356. https://doi.org/10.2196/13356
Morgan AJ, Ross AM, Yap MBH, Reavley NJ, Parker A, Simmons MB, Scanlan F, Jorm AF (2020) What works for mental health problems in youth? survey of real-world experiences of treatments and side effects. Early Interv Psychiatry 15(6):1502–1512. https://doi.org/10.1111/eip.13087
Stafford AM, Aalsma MC, Bigatti SM, Oruche UM, Draucker CB (2019) Getting a grip on my depression: a grounded theory explaining how Latina adolescents experience, self-manage, and seek treatment for depressive symptoms. Journal of Adolescent Health 64 (2, Supplement) S2-S3 https://doi.org/10.1016/j.jadohealth.2018.10.018
Kim S-I, Jo E, Ryu M, Cha I, Kim Y-H, Yoo H, Hong H (2019) Toward becoming a better self: understanding self-tracking experiences of adolescents with Autism spectrum disorder using custom trackers. Paper presented at the proceedings of the 13th EAI International Conference on Pervasive Computing Technologies for Healthcare, Trento, Italy. https://doi.org/10.1145/3329189.3329209
Poppelaars M, Tak YR, Lichtwarck-Aschoff A, Engels RCME, Lobel A, Merry SN, Lucassen MFG, Granic I (2016) A randomized controlled trial comparing two cognitive-behavioral programs for adolescent girls with subclinical depression: a school-based program (Op Volle Kracht) and a computerized program (SPARX). Behav Res Ther 80:33–42. https://doi.org/10.1016/j.brat.2016.03.005
Stafford AM (2019) The unfolding of depressive symptoms, disease self-management, and treatment utilization for Latina adolescents. Dissertation, Indiana University
Williamson H, Griffiths C, Harcourt D (2015) Developing young person’s Face IT: Online psychosocial support for adolescents struggling with conditions or injuries affecting their appearance. Health Psychology Open 2(2):2055102915619092. https://doi.org/10.1177/2055102915619092
Recto P, Dimmitt Champion J (2018) Mexican-American adolescents’ perceptions about causes of perinatal depression, self-help strategies, and how to obtain mental health information. J Child Adolesc Psychiatr Nurs 31(2–3):61–69. https://doi.org/10.1111/jcap.12210
Cheek C, Bridgman H, Fleming T, Cummings E, Ellis L, Lucassen MF, Shepherd M, Skinner T (2014) Views of young people in rural Australia on SPARX, a fantasy world developed for New Zealand youth with depression. JMIR serious games 2(1):e3–e3. https://doi.org/10.2196/games.3183
Logsdon C, Myers J, Rushton J, Gregg JL, Josephson AM, Davis DW, Brothers K, Baisch K, Carabello A, Vogt K, Jones K, Angermeier J (2018) Efficacy of an internet-based depression intervention to improve rates of treatment in adolescent mothers. Arch Womens Ment Health 21(3):273–285. https://doi.org/10.1007/s00737-017-0804-z
Lucassen M, Samra R, Iacovides I, Fleming T, Shepherd M, Stasiak K, Wallace L (2018) How LGBT+ young people use the internet in relation to their mental health and envisage the use of e-therapy: exploratory study. JMIR Serious Games 6(4):e11249. https://doi.org/10.2196/11249
Bevan Jones R, Thapar A, Rice F, Mars B, Agha SS, Smith D, Merry S, Stallard P, Thapar AK, Jones I, Simpson SA (2020) A digital intervention for adolescent depression (moodhwb): mixed methods feasibility evaluation. JMIR Ment Health 7(7):e14536. https://doi.org/10.2196/14536
Domhardt M, Steubl L, Baumeister H (2020) Internet- and mobile-based interventions for mental and somatic conditions in children and adolescents. Z Kinder Jugendpsychiatr Psychother 48(1):33–46. https://doi.org/10.1024/1422-4917/a000625
Radomski AD, Bagnell A, Curtis S, Hartling L, Newton AS (2020) Examining the usage, user experience, and perceived impact of an internet-based cognitive behavioral therapy program for adolescents with anxiety: randomized controlled trial. JMIR Ment Health 7(2):e15795. https://doi.org/10.2196/15795
Rickwood D, Bradford S (2012) The role of self-help in the treatment of mild anxiety disorders in young people: an evidence-based review. Psychol Res Behav Manag 5:25–36. https://doi.org/10.2147/PRBM.S23357
Rummel-Kluge C, Dietrich S, Koburger N (2015) Behavioural and cognitive-behavioural therapy based self-help versus treatment as usual for depression in adults and adolescents. Cochrane Database Systematic Reviews. https://doi.org/10.1002/14651858.CD011744
Whittaker R, Stasiak K, McDowell H, Doherty I, Shepherd M, Chua S, Dorey E, Parag V, Ameratunga S, Rodgers A, Merry S (2017) MEMO: an mHealth intervention to prevent the onset of depression in adolescents: a double-blind, randomised, placebo-controlled trial. J Child Psychol Psychiatry 58(9):1014–1022. https://doi.org/10.1111/jcpp.12753
Yuan S, Zhou X, Zhang Y, Zhang H, Pu J, Yang L, Liu L, Jiang X, Xie P (2018) Comparative efficacy and acceptability of bibliotherapy for depression and anxiety disorders in children and adolescents: a meta-analysis of randomized clinical trials. Neuropsychiatr Dis Treat 14:353–365. https://doi.org/10.2147/ndt.S152747
McLellan LF, Fitzpatrick S, Schniering CA, Rapee RM (2019) Self-help treatment of childhood anxiety disorders: innovations in CBT for childhood anxiety, OCD, and PTSD: improving access and outcomes. Cambridge University Press, New York, NY, US. https://doi.org/10.1017/9781108235655.004
Clarke J, Vatiliotis V, Verge CF, Holmes-Walker J, Campbell LV, Wilhelm K, Proudfoot J (2015) A mobile phone and web-based intervention for improving mental well-being in young people with type 1 diabetes: design of a randomized controlled trial. JMIR Res Protoc 4(2):e50. https://doi.org/10.2196/resprot.4032
Wolters LH, Op de Beek V, Weidle B, Skokauskas N (2017) How can technology enhance cognitive behavioral therapy: the case of pediatric obsessive compulsive disorder. BMC Psychiatry 17(1):226–226. https://doi.org/10.1186/s12888-017-1377-0
Garrido S, Millington C, Cheers D, Boydell K, Schubert E, Meade T, Nguyen QV (2019) What works and what doesn’t work? a systematic review of digital mental health interventions for depression and anxiety in young people. Front Psych 10:759–759. https://doi.org/10.3389/fpsyt.2019.00759
Bradley KL, Robinson LM, Brannen CL (2012) Adolescent help-seeking for psychological distress, depression, and anxiety using an internet program. Int J Ment Health Promot 14(1):23–34. https://doi.org/10.1080/14623730.2012.665337
Christensen H, Reynolds J, Griffiths KM (2011) The use of e-health applications for anxiety and depression in young people: challenges and solutions. Early Interv Psychiatry 5(Suppl 1):58–62. https://doi.org/10.1111/j.1751-7893.2010.00242.x
Cunningham M, Rapee R, Lyneham H (2006) Feedback to a prototype self-help computer program for anxiety disorders in adolescents. Australian e-Journal for the Advancement of Mental Health 5(3):216–224. https://doi.org/10.5172/jamh.5.3.216
Davidson TM, Yuen EK, Felton JW, McCauley J, Gros KS, Ruggiero KJ (2014) Feasibility assessment of a brief, web-based behavioral activation intervention for adolescents with depressed mood. Inter J Psy Med 48(1):69–82. https://doi.org/10.2190/PM.48.1.f
Ebert DD, Zarski AC, Christensen H, Stikkelbroek Y, Cuijpers P, Berking M, Riper H (2015) Internet and computer-based cognitive behavioral therapy for anxiety and depression in youth: a meta-analysis of randomized controlled outcome trials. PLoS One 10(3):e0119895. https://doi.org/10.1371/journal.pone.0119895
Makarushka MM (2011) Efficacy of an internet-based intervention targeted to adolescents with subthreshold depression. Dissertation, University of Oregon
Rasing SPA, Stikkelbroek YAJ, Bodden DHM (2019) Is Digital Treatment the holy grail? literature review on computerized and blended treatment for depressive disorders in youth. Int J Environ Res Public Health 17(1):153. https://doi.org/10.3390/ijerph17010153
Stasiak K, Fleming T, Lucassen MF, Shepherd MJ, Whittaker R, Merry SN (2016) Computer-based and online therapy for depression and anxiety in children and adolescents. J Child Adolesc Psychopharmacol 26(3):235–245. https://doi.org/10.1089/cap.2015.0029
Toscos T, Coupe A, Flanagan M, Drouin M, Carpenter M, Reining L, Roebuck A, Mirro MJ (2019) Teens using screens for help: impact of suicidal ideation, anxiety, and depression levels on youth preferences for telemental health resources. JMIR Ment Health 6(6):e13230. https://doi.org/10.2196/13230
Oh E, Jorm AF, Wright A (2008) Perceived helpfulness of websites for mental health information. Soc Psychiatry Psychiatr Epidemiol 44(4):293. https://doi.org/10.1007/s00127-008-0443-9
Cunningham M (2008) Overview of design approaches in the Cool Teens CD and other computer programs for adolescent anxiety. E-J Appl Psycho 4(2):6–11. https://doi.org/10.7790/ejap.v4i2.116
Whiteside SP (2016) Mobile device-based applications for childhood anxiety disorders. J Child Adolesc Psychopharmacol 26(3):246–251. https://doi.org/10.1089/cap.2015.0010
Lucassen MF, Stasiak K, Fleming T, Frampton C, Perry Y, Shepherd M, Merry SN (2020) Computerized cognitive behavioural therapy for gender minority adolescents: analysis of the real-world implementation of SPARX in New Zealand. Aust N Z J Psychiatry. https://doi.org/10.1177/0004867420976846
Merry SN, Stasiak K, Shepherd M, Frampton C, Fleming T, Lucassen MFG (2012) The effectiveness of SPARX, a computerised self help intervention for adolescents seeking help for depression: randomised controlled non-inferiority trial. BMJ : British Med J. https://doi.org/10.1136/bmj.e2598
Richardson T, Stallard P, Velleman S (2010) Computerised cognitive behavioural therapy for the prevention and treatment of depression and anxiety in children and adolescents: a systematic review. Clin Child Fam Psychol Rev 13(3):275–290. https://doi.org/10.1007/s10567-010-0069-9
Stice E, Rohde P, Gau JM, Wade E (2010) Efficacy trial of a brief cognitive-behavioral depression prevention program for high-risk adolescents: effects at 1- and 2-year follow-up. J Consult Clin Psychol 78(6):856–867. https://doi.org/10.1037/a0020544
Stice E, Rohde P, Seeley JR, Gau JM (2008) Brief cognitive-behavioral depression prevention program for high-risk adolescents outperforms two alternative interventions: a randomized efficacy trial. J Consult Clin Psychol 76(4):595–606. https://doi.org/10.1037/a0012645
Grist R, Porter J, Stallard P (2017) Mental health mobile apps for preadolescents and adolescents: a systematic review. J Med Internet Res 19(5):e176. https://doi.org/10.2196/jmir.7332
Meichenbaum D (2018) Ways to bolster resilience in lesbian, gay, bisexual, transgender, and questioning (LGBTQ) youth. Feminist transnational perspectives, Handbook of sex trafficking. https://doi.org/10.1007/978-3-319-73621-1_25
Stasiak K, Hatcher S, Frampton C, Merry SN (2012) A pilot double blind randomized placebo controlled trial of a prototype computer-based cognitive behavioural therapy program for adolescents with symptoms of depression. Behav Cogn Psychother 42(4):385–401. https://doi.org/10.1017/s1352465812001087
Calear AL, Christensen H, Mackinnon A, Griffiths KM (2013) Adherence to the MoodGYM program: outcomes and predictors for an adolescent school-based population. J Affect Disord 147(1):338–344. https://doi.org/10.1016/j.jad.2012.11.036
Barnes S, Prescott J (2018) Empirical evidence for the outcomes of therapeutic video games for adolescents with anxiety disorders: systematic review. JMIR Serious Games 6(1):e3. https://doi.org/10.2196/games.9530
Wisdom JP, Barker EC (2006) Getting out of depression: teens’ self-help interventions to relieve depressive symptoms. Child Fam Behav Ther 28(4):1–11. https://doi.org/10.1300/J019v28n04_01
Stafford AM, Nagy G, Gonzalez-Guarda R, Draucker CB (2020) The Influence of peer relationships on Latina adolescents’ experiences with depressive symptoms. J Pediatric Nursing: Nursing Care Children Families 55:250–257. https://doi.org/10.1016/j.pedn.2020.07.004
Gega L, Gilbody S (2015) Software-based psychotherapy: the example of computerized cognitive-behavioral therapy. Mental health in the digital age: Grave dangers, great promise. Oxford University Press, New York, NY, US. https://doi.org/10.1093/med/9780199380183.003.0011
Ahmead M, Bower P (2008) The effectiveness of self help technologies for emotional problems in adolescents: a systematic review. Child Adolesc Psychiatry Ment Health 2(1):20. https://doi.org/10.1186/1753-2000-2-20
Jorm AF, Allen NB, O’Donnell CP, Parslow RA, Purcell R, Morgan AJ (2006) Effectiveness of complementary and self-help treatments for depression in children and adolescents. Med J Aust 185(7):368–372. https://doi.org/10.5694/j.1326-5377.2006.tb00612.x
Helgeson VS, Novak SA (2007) Illness centrality and well-being among male and female early adolescents with diabetes. J Pediatr Psychol 32(3):260–272. https://doi.org/10.1093/jpepsy/jsl018
Dashiff CJ, McCaleb A, Cull V (2006) Self-care of young adolescents with type 1 diabetes. J Pediatr Nurs 21(3):222–232. https://doi.org/10.1016/j.pedn.2005.07.013
Tomky D, Tomky D, Cypress M, Dang D, Maryniuk M, Peyrot M, Mensing C (2008) Aade position statement. Diabetes Educ 34(3):445–449. https://doi.org/10.1177/0145721708316625
Pretorius C, Chambers D, Coyle D (2019) Young people’s online help-seeking and mental health difficulties: systematic narrative review. J Med Internet Res 21(11):e13873–e13873. https://doi.org/10.2196/13873
Charbonnier E, Trémolière B, Baussard L, Goncalves A, Lespiau F, Philippe AG, Le Vigouroux S (2022) Effects of an online self-help intervention on university students’ mental health during COVID-19: a non-randomized controlled pilot study. Computers Human Behavior Reports 5:100175. https://doi.org/10.1016/j.chbr.2022.100175
Shalaby RAH, Agyapong VIO (2020) Peer support in mental health: literature review. JMIR Ment Health 7(6):e15572. https://doi.org/10.2196/15572
Stinson J, Wilson R, Gill N, Yamada J, Holt J (2009) A systematic review of internet-based self-management interventions for youth with health conditions. J Pediatr Psychol 34(5):495–510. https://doi.org/10.1093/jpepsy/jsn115
Lindsay S, McDougall C, Sanford R (2013) Disclosure, accommodations and self-care at work among adolescents with disabilities. Disabil Rehabil 35(26):2227–2236. https://doi.org/10.3109/09638288.2013.775356
Muir-Cochrane E, Fereday J, Jureidini J, Drummond A, Darbyshire P (2006) Self-management of medication for mental health problems by homeless young people. Int J Ment Health Nurs 15(3):163–170. https://doi.org/10.1111/j.1447-0349.2006.00420.x
Kaess M, Moessner M, Koenig J, Lustig S, Bonnet S, Becker K, Eschenbeck H, Rummel-Kluge C, Thomasius R, Bauer S, Pro HC (2021) Editorial Perspective: a plea for the sustained implementation of digital interventions for young people with mental health problems in the light of the COVID-19 pandemic. J Child Psychol Psychiatry 62(7):916–918. https://doi.org/10.1111/jcpp.13317
Kooth (2020) Week 14: how Covid-19 is affecting the mental health of children and young people
Smiles S, Briggs A (1958) Self-help: with illustrations of conduct and perserverance / with an introduction by Asa Briggs. John Murray, London
Michie S, van Stralen MM, West R (2011) The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement Sci 6(1):42. https://doi.org/10.1186/1748-5908-6-42
Aloud N, Rathur A (2009) Factors affecting attitudes toward seeking and using formal mental health and psychological services among arab muslim populations. J Muslim Mental Health 4(2):79–103. https://doi.org/10.1080/15564900802487675
Marshall A (2016) Suicide prevention interventions for sexual and gender Minority Youth: an unmet need. Yale J Biol Med 89(2):205–213. http://www.ncbi.nlm.nih.gov/pmc/articles/pmc4918883/
Steele LS, Daley A, Curling D, Gibson MF, Green DC, Williams CC, Ross LE (2016) LGBT Identity, untreated depression, and unmet need for mental health services by sexual minority women and trans-identified people. J Womens Health 26(2):116–127. https://doi.org/10.1089/jwh.2015.5677
Kneale D, Becares L (2020) The mental health and experiences of discrimination of LGBTQ+ people during the COVID-19 pandemic: Initial findings from the Queerantine Study. medRxiv:2020.2008.2003.20167403. https://doi.org/10.1101/2020.08.03.20167403
Bry LJ, Chou T, Miguel E, Comer JS (2018) Consumer smartphone apps marketed for child and adolescent anxiety: a systematic review and content analysis. Behav Ther 49(2):249–261. https://doi.org/10.1016/j.beth.2017.07.008
Haeffel GJ (2010) When self-help is no help: traditional cognitive skills training does not prevent depressive symptoms in people who ruminate. Behav Res Ther 48(2):152–157. https://doi.org/10.1016/j.brat.2009.09.016
Krebs G, Turner C (2019) Self-help treatments for childhood obsessive-compulsive disorder including bibliotherapy. innovations in CBT for childhood anxiety, OCD, and PTSD: improving access and outcomes:332
Lerman BI, Lewis SP, Lumley M, Grogan GJ, Hudson CC, Johnson E (2017) Teen depression groups on facebook: a content analysis. J Adolesc Res 32(6):719–741. https://doi.org/10.1177/0743558416673717
Newbold A, Warren FC, Taylor RS, Hulme C, Burnett S, Aas B, Botella C, Burkhardt F, Ehring T, Fontaine JRJ, Frost M, Garcia-Palacios A, Greimel E, Hoessle C, Hovasapian A, Huyghe VEI, Lochner J, Molinari G, Pekrun R, Platt B, Rosenkranz T, Scherer KR, Schlegel K, Schulte-Korne G, Suso C, Voigt V, Watkins ER (2020) Promotion of mental health in young adults via mobile phone app: study protocol of the ECoWeB (emotional competence for well-being in young adults) cohort multiple randomised trials. BMC Psychiatry 20(1):458. https://doi.org/10.1186/s12888-020-02857-w
Ollendick TH, Öst L-G, Farrell LJ (2018) Innovations in the psychosocial treatment of youth with anxiety disorders: implications for a stepped care approach. Evid Based Ment Health 21(3):112–115. https://doi.org/10.1136/eb-2018-102892
Parslow R, Morgan AJ, Allen NB, Jorm AF, O’Donnell CP, Purcell R (2008) Effectiveness of complementary and self-help treatments for anxiety in children and adolescents. Med J Aust 188(6):355–359. https://doi.org/10.5694/j.1326-5377.2008.tb01654.x
Pennant ME, Loucas CE, Whittington C, Creswell C, Fonagy P, Fuggle P, Kelvin R, Naqvi S, Stockton S, Kendall T (2015) Computerised therapies for anxiety and depression in children and young people: a systematic review and meta-analysis. Behav Res Ther 67:1–18. https://doi.org/10.1016/j.brat.2015.01.009
Rees CS, Anderson RA, Kane RT, Finlay-Jones AL (2016) Online obsessive-compulsive disorder treatment: preliminary results of the “OCD? Not Me!” self-guided internet-based cognitive behavioral therapy program for young people. JMIR mental health 3(3):e5363. https://doi.org/10.2196/mental.5363
Acknowledgements
Sophie Pattison, Acting Subject Liaison Librarian for Biosciences and Psychology, UCL Library Services, London, UK, for assistance in developing a search strategy for this review. Professor Jessica Deighton, Director of the Evidence Based Practice Unit, Anna Freud Centre and University College London, London, UK, for assistance with planning this scoping review and reviewing early drafts of this manuscript. Dr. David Robinson, Technical Writer, Amazon, Seattle, WA, United States, for assistance in reviewing and editing a draft of this manuscript. This scoping review will fulfil part of the requirements of a PhD in psychology at University College London for RT.
Funding
This report is independent research funded by the National Institute for Health and Care Research ARC North Thames. The views expressed in this publication are those of the author(s) and not necessarily those of the National Institute for Health Research and Care or the Department of Health and Social Care.
Author information
Authors and Affiliations
Contributions
RT: Collecting the data, performing the analysis, writing the manuscript, editing the manuscript. Dr. DH: Providing supervisory support, designing the analysis, contributing to the analysis, editing the manuscript. AM: Conducting the second reviewer title and abstract screening, conducting the second reviewer full-text screening, contributing to reviewing the data extraction instrument, editing the manuscript. Professor PF: Providing supervisory support, designing the analysis, editing the manuscript. Dr. ES: Providing supervisory support, designing the analysis, contributing to the analysis, editing the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Appendices
Appendix 1: Search strategy
Final searches conducted: 15th, 17th, and 22nd February 2021.
PsycINFO (Ovid).
Search conducted 15th February 2021.
Search | Query | Records retrieved |
|---|---|---|
#1 | self car*.mp | |
#2 | self help*.mp | |
#3 | self manag*.mp | |
#4 | adolescen*.mp | |
#5 | child*.mp | |
#6 | kid?.mp | |
#7 | emerging adult*.mp | |
#8 | juvenile?.mp | |
#9 | minor?.mp | |
#10 | p?ediatric?.mp | |
#11 | teen*.mp | |
#12 | young adult*.mp | |
#13 | young people.mp | |
#14 | young person.mp | |
#15 | youth?.mp | |
#16 | acute stress.mp | |
#17 | anxiet*.mp | |
#18 | anxious*.mp | |
#19 | avoid*.mp | |
#20 | depress*.mp | |
#21 | emotional difficult*.mp | |
#22 | emotional disorder*.mp | |
#23 | emotional* health*.mp | |
#24 | emotional illness*.mp | |
#25 | emotional issue?.mp | |
#26 | GAD.mp | |
#27 | internali?ing.mp | |
#28 | low mood?.mp | |
#29 | major depress*.mp | |
#30 | mood disorder.mp | |
#31 | obsessive compulsive.mp | |
#32 | OCD.mp | |
#33 | panic*.mp | |
#34 | post traumatic stress.mp | |
#35 | posttraumatic stress.mp | |
#36 | PTSD.mp | |
#37 | social* phobi*.mp | |
#38 | stressor?.mp | |
#39 | trauma*.mp | |
#40 | worrie*.mp | |
#41 | worry.mp | |
#42 | specific phobia?.mp | |
#43 | Self-care/ | |
#44 | Self-help techniques/ | |
#45 | Adolescent development/ or early adolescence/ | |
#46 | Self-management/ | |
#47 | 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 | |
#48 | 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 45 | |
#49 | 1 or 2 or 3 or 43 or 44 or 46 | |
#50 | 47 and 48 and 49 | |
Limited to English language, published from 1st January 2000 to present | 2089 | |
Embase (Ovid)
Search conducted 15th February 2021.
Search | Query | Records retrieved |
|---|---|---|
#1 | self car*.mp | |
#2 | self help*.mp | |
#3 | self manag*.mp | |
#4 | adolescen*.mp | |
#5 | child*.mp | |
#6 | kid?.mp | |
#7 | emerging adult*.mp | |
#8 | juvenile?.mp | |
#9 | minor?.mp | |
#10 | p?ediatric?.mp | |
#11 | teen*.mp | |
#12 | young adult*.mp | |
#13 | young people.mp | |
#14 | young person.mp | |
#15 | youth?.mp | |
#16 | acute stress.mp | |
#17 | anxiet*.mp | |
#18 | anxious*.mp | |
#19 | avoid*.mp | |
#20 | depress*.mp | |
#21 | emotional difficult*.mp | |
#22 | emotional disorder*.mp | |
#23 | emotional* health*.mp | |
#24 | emotional illness*.mp | |
#25 | emotional issue?.mp | |
#26 | GAD.mp | |
#27 | internali?ing.mp | |
#28 | low mood?.mp | |
#29 | major depress*.mp | |
#30 | mood disorder.mp | |
#31 | obsessive compulsive.mp | |
#32 | OCD.mp | |
#33 | panic*.mp | |
#34 | post traumatic stress.mp | |
#35 | posttraumatic stress.mp | |
#36 | PTSD.mp | |
#37 | social* phobi*.mp | |
#38 | stressor?.mp | |
#39 | trauma*.mp | |
#40 | worrie*.mp | |
#41 | worry.mp | |
#42 | specific phobia?.mp | |
#43 | self care/ | |
#44 | self help/ | |
#45 | adolescent/ | |
#46 | 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 | |
#47 | 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 45 | |
#48 | 1 or 2 or 3 or 43 or 44 | |
#49 | 46 and 47 and 48 | |
Limited to English language, published from 1st January 2000 to present | 3263 | |
Medline (Ovid)
Search conducted 15th February 2021.
Search | Query | Records retrieved |
|---|---|---|
#1 | self car*.mp | |
#2 | self help*.mp | |
#3 | self manag*.mp | |
#4 | adolescen*.mp | |
#5 | child*.mp | |
#6 | kid?.mp | |
#7 | emerging adult*.mp | |
#8 | juvenile?.mp | |
#9 | minor?.mp | |
#10 | p?ediatric?.mp | |
#11 | teen*.mp | |
#12 | young adult*.mp | |
#13 | young people.mp | |
#14 | young person.mp | |
#15 | youth?.mp | |
#16 | acute stress.mp | |
#17 | anxiet*.mp | |
#18 | anxious*.mp | |
#19 | avoid*.mp | |
#20 | depress*.mp | |
#21 | emotional difficult*.mp | |
#22 | emotional disorder*.mp | |
#23 | emotional* health*.mp | |
#24 | emotional illness*.mp | |
#25 | emotional issue?.mp | |
#26 | GAD.mp | |
#27 | internali?ing.mp | |
#28 | low mood?.mp | |
#29 | major depress*.mp | |
#30 | mood disorder.mp | |
#31 | obsessive compulsive.mp | |
#32 | OCD.mp | |
#33 | panic*.mp | |
#34 | post traumatic stress.mp | |
#35 | posttraumatic stress.mp | |
#36 | PTSD.mp | |
#37 | social* phobi*.mp | |
#38 | stressor?.mp | |
#39 | trauma*.mp | |
#40 | worrie*.mp | |
#41 | worry.mp | |
#42 | specific phobia?.mp | |
#43 | Self-management/ or self care/ | |
#44 | Self-help groups/ | |
#45 | Adolescent/ | |
#46 | 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 | |
#47 | 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 45 | |
#48 | 1 or 2 or 3 or 43 or 44 | |
#49 | 46 and 47 and 48 | |
Limited to English language, published from 1st January 000 to present | 2288 | |
Cinahl plus (EBSCO)
Search conducted 15th February 2021.
Search | Query | Records retrieved |
|---|---|---|
S1 | (MH “Adolescence”) | |
S2 | (MH “Self-Management”) | |
S3 | (MH “Self Care”) | |
S4 | “specific phobia#” | |
S5 | worry | |
S6 | worrie* | |
S7 | trauma* | |
S8 | stressor# | |
S9 | “social* phobi*” | |
S10 | PTSD | |
S11 | “posttraumatic stress” | |
S12 | “post traumatic stress” | |
S13 | panic* | |
S14 | OCD | |
S15 | “obsessive compulsive” | |
S16 | “mood disorder” | |
S17 | “major depress*” | |
S18 | “low mood#” | |
S19 | internalizing | |
S20 | GAD | |
S21 | “emotional issue#” | |
S22 | “emotional illness*” | |
S23 | “emotional* health*” | |
S24 | “emotional disorder*” | |
S25 | “emotional difficult*” | |
S26 | depress* | |
S27 | avoid* | |
S28 | anxious* | |
S29 | anxiet* | |
S30 | “acute stress” | |
S31 | youth# | |
S32 | “young person” | |
S33 | “young people” | |
S34 | “young adult*” | |
S35 | teen* | |
S36 | p#ediatric# | |
S37 | minor# | |
S38 | juvenile# | |
S39 | “emerging adult*” | |
S40 | kid# | |
S41 | child* | |
S42 | adolescen* | |
S43 | “self manag*” | |
S44 | “self help*” | |
S45 | “self car*” | |
S46 | S2 OR S3 OR S43 OR S44 OR S45 | |
S47 | S1 OR S31 OR S32 OR S33 OR S34 OR S35 OR S36 OR S37 OR S38 OR S39 OR S40 OR S41 OR S42 | |
S48 | S4 OR S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 | |
S49 | S46 AND S47 AND S48 | |
Limited to English language, published from1st January 2000 to present | 1657 | |
Web of science
Search conducted 17th February 2021.
Search | Query | Records retrieved |
|---|---|---|
#1 | “self car*” | |
#2 | “self help*” | |
#3 | “self manag*” | |
#4 | adolescen* | |
#5 | child* | |
#6 | kid$ | |
#7 | “emerging adult*” | |
#8 | juvenile$ | |
#9 | minor$ | |
#10 | p$ediatric | |
#11 | teen* | |
#12 | “young adult*” | |
#13 | “young people” | |
#14 | “young person” | |
#15 | youth$ | |
#16 | “acute stress” | |
#17 | anxiet* | |
#18 | anxious* | |
#19 | avoid* | |
#20 | depress* | |
#21 | “emotional difficult*” | |
#22 | “emotional disorder*” | |
#23 | “emotional* health*” | |
#24 | “emotional illness*” | |
#25 | “emotional issue$” | |
#26 | GAD | |
#27 | internali$ing | |
#28 | “low mood$” | |
#29 | “major depress*” | |
#30 | “mood disorder” | |
#31 | “obsessive compulsive” | |
#32 | OCD | |
#33 | panic* | |
#34 | “post traumatic stress” | |
#35 | “posttraumatic stress” | |
#36 | PTSD | |
#37 | “social* phobi*” | |
#38 | stressor$ | |
#39 | trauma* | |
#40 | worrie* | |
#41 | worry | |
#42 | “specific phobia$” | |
#43 | #42 OR #41 OR #40 OR #39 OR #38 OR #37 OR #36 OR #35 OR #34 OR #33 OR #32 OR #31 OR #30 OR #29 OR #28 OR #27 OR #26 OR #25 OR #24 OR #23 OR #22 OR #21 OR #20 OR #19 OR #18 OR #17 OR #16 | |
#44 | #15 OR #14 OR #13 OR #12 OR #11 OR #10 OR #9 OR #8 OR #7 OR #6 OR #5 OR #4 | |
#45 | #3 OR #2 OR #1 | |
#46 | #45 AND #44 AND #43 | |
Limited to English language, published from 1st January 2000 to present | 1766 | |
Mednar
Search conducted 22nd February 2021.
Search | Query | Records retrieved |
|---|---|---|
#1 | (self care OR self help OR self manage) AND (adolescent OR young person) AND (acute stress OR anxiety OR avoid OR depress OR emotional disorder OR GAD OR internalizing OR low mood OR mood disorder OR obsessive compulsive OR panic OR post traumatic stress OR social phobia OR stressor OR trauma OR worry OR specific phobia) | |
Limited to English language, published from 1st January 2000 to present | 168 | |
Appendix 2: Data extraction instrument
Background information | |
Reference number | |
Reviewer (1st or 2nd) | |
Date of data extraction | |
Author(s) | |
Year | |
Title | |
Journal (if applicable) | |
Study description | |
Study design (e.g., RCT, experimental, systematic or scoping review, qualitative, quantitative) | |
Data collection method (e.g., surveys, telephone interviews, questionnaires), including measures | |
Data analysis method (e.g., thematic analysis, grounded theory, SPSS tests run) | |
Construct 1: Self-management, self-help, self-care, or other (please specify)? | |
Emotional problem(s) being targeted by Construct 1 | |
Study setting (e.g., school, hospital) | |
Country (or countries) where study was conducted (e.g., England) | |
Rural/urban (if stated)? | |
N of participants | |
Participant age range | |
Participant mean age (SD) | |
Participant gender identity or biological sex | |
Any specialist characteristics of participants? (e.g., homeless, LGBTQ + , Latina) | |
Participant ethnicity | |
Results or details extracted | |
Self-care definition or introduction in paper (if applicable) | |
Self-care related strategies or techniques (if applicable) | |
Self-management definition or introduction in paper (if applicable) | |
Self-management related strategies or techniques (if applicable) | |
Self-help definition or introduction in paper (if applicable) | |
Self-help related strategies or techniques (if applicable) | |
Summary of evaluation or empirical findings (if applicable) | |
Limitations (as stated by authors) | |
Reviewer comments | |
Appendix 3: Characteristics of included studies
Source | Country | Type of literature | Study population/sample size | Construct being studied |
|---|---|---|---|---|
[106] | USA and Australia | Systematic review | N/A | self-help |
[102] | Global | Systematic review | N/A | self-management |
[17] | Global | Systematic review and meta-analysis | N/A | self-help |
[70] | Wales | Mixed methods feasibility evaluation | 19 adolescents | self-management, self-help |
[81] | Canada | Qualitative interview study | 13 adolescents | self-help |
[125] | Global | Systematic review | N/A | self-management |
[67] | Tasmania | Qualitative | 16 rural Australian adolescents | self-help |
[82] | N/A | Qualitative review of research literature | N/A | self-help |
[78] | Australia | Protocol for an RCT | 280 adolescents (prospective) | self-help |
[83] | Australia | Feedback to a prototype | 22 adolescents | self-help |
[91] | Global | Review paper | N/A | self-help |
[84] | United States | Feasibility study (also looking at rates of access to an online intervention) | 24 adolescents | self-help |
[71] | Global | Systematic review of meta-analyses | N/A | self-help |
[85] | Global | Meta-analysis of randomized controlled outcome trials | N/A | self-help |
[80] | Global | Systematic review | N/A | self-help |
[105] | N/A | Book chapter | N/A | self-help |
[98] | Global | Systematic review | N/A | self-help |
[126] | USA | A randomized trial | 72 adolescents | self-help |
[107] | Global | Systematic literature search | N/A | self-help |
[62] | South Korea | Qualitative and questionnaire | 5 adolescents with ASD | self-management, self-care |
[127] | N/A | Book chapter | N/A | self-help |
[128] | Not collected | Qualitative content analysis | 508 Facebook posts by adolescents | self-help |
[68] | United States | Quantitative pretest–posttest design | 154 adolescent mothers in the intervention group | self-management |
[58] | New Zealand | Open pilot trial | 21 sexual minority adolescents | self-help |
[69] | England | Qualitative | 21 LGBT + adolescents | self-care |
[93] | New Zealand | Quantitative analysis of usage data | 9079 adolescents | self-help |
[86] | United States | Dissertation | 76 adolescents in the treatment group | self-help |
[77] | Global | Book chapter | N/A | self-help |
[99] | N/A | Book chapter/fact sheet | N/A | self-care |
[94] | New Zealand | Randomized controlled non-inferiority trial | 94 adolescents | self-help |
[60] | English speaking, high-income countries—Australia (40.9%), United Kingdom (22.1%), New Zealand (12.8%), United States (10.8%), Canada (7.5%), Ireland (4.7%), other (1.3%) | Survey study | 557 adolescents | self-help |
[129] | United Kingdom, Germany, Spain, Belgium | Protocol for a cohort multiple randomized control trial | 2142 adolescents (prospective) | self-help |
[59] | Canada | Pilot randomized control trial | 70 adolescents | self-management |
[90] | Australia | Telephone survey study | 3746 adolescents | self-help |
[130] | Global | Review paper | N/A | self-help |
[131] | Global | Systematic literature review | N/A | self-help |
[132] | Global | Systematic review and meta-analysis | N/A | self-help |
[63] | The Netherlands | Randomized controlled trial | 51 adolescents | self-help |
[72] | Canada | Randomized controlled trial | 536 adolescents | self-help, self-management |
[87] | Global | Systematic literature review | N/A | self-help |
[66] | United States | Qualitative descriptive study | 20 Mexican American adolescents | self-help |
[133] | Australia | Preliminary results from an open trial | 132 adolescents | self-help |
[95] | Global | Systematic review | N/A | self-help |
[73] | Global | Systematic literature review | N/A | self-help |
[74] | N/A | Systematic review protocol | N/A | self-help, self-management |
[57] | Australia | Predictive study involving an evaluation | 3684 adolescents | self-help |
United States | Qualitative study | 25 Latina adolescents | self-management | |
[104] | United States | Qualitative interview study | 25 Latina adolescents | self-management |
N/A | PhD thesis | N/A | self-management | |
[100] | New Zealand | Pilot double blind randomized controlled trial | 17 adolescents in the intervention group | self-help |
[88] | Global | Review | N/A | self-help |
[97] | United States | Randomized efficacy trial | 80 adolescents in the bibliotherapy control intervention | self-help |
[96] | United States | Effects of an efficacy trial at 1- and 2-year follow-up | 80 adolescents in the bibliotherapy control intervention) | self-help |
[89] | United States | Survey/questionnaire study | 2789 adolescents | self-help |
[92] | United States | Literature review and an evaluation | 169 adolescents | self-help |
[75] | New Zealand | Double-blind randomized placebo-controlled trial | 426 adolescents in the intervention group | self-help |
[65] | United Kingdom | Evaluation of the acceptability of an intervention | 28 adolescents with visible physical differences | self-management |
[103] | United States | Qualitative interview study | 14 adolescents | self-help |
Global | Scoping review and systematic review | N/A | self-help, self-care | |
[79] | Global | Debate paper referencing systematic reviews | N/A | self-help |
[48] | United Kingdom | Single center RCT feasibility study | 91 adolescents | self-help |
[76] | Global | Meta-analysis of randomized clinical trials | N/A | self-help, self-management |
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Town, R., Hayes, D., March, A. et al. Self-management, self-care, and self-help in adolescents with emotional problems: a scoping review. Eur Child Adolesc Psychiatry (2023). https://doi.org/10.1007/s00787-022-02134-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00787-022-02134-z