
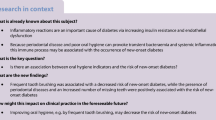
Abstract
Objectives
Periodontitis is a non-communicable disease (NCD) that may be linked to other NCDs through shared risk factors. Accordingly, we analyzed the relationship between periodontitis and behavioral and metabolic risks common to NCDs in Brazilian adults over three decades.
Methods
Indicators of periodontitis, behavioral risks (smoking, alcohol use, sugar-sweetened beverages (SSB), and physical activity), and metabolic risks (overweight/obesity, dyslipidemia, hyperglycemia, and hypertension) in Brazilian adults (25–49 y-old) between 1990 to 2019 were obtained from the Global Burden of Disease Study 2019. Data were adjusted for Gini index. Fixed-effects and Prais-Winsten regressions were performed (p < 0.05).
Results
The prevalence of periodontitis has increased among Brazilians since 2005. High-SSB diet, alcohol use, and metabolic risks increased between 1990–2019, whereas smoking decreased. In crude models, periodontitis prevalence increased with alcohol use (2545.1; 95%CI: 2307.9–2782.3), high-SSB diet (365.5; 95%CI: 322.5–408.4), low physical activity (1784.4; 95%CI: 763.7–2805.0), overweight/obesity (172.3; 95%CI: 156.3–188.4), dyslipidemia (734.5; 95%CI: 624.7–844.2), and hyperglycemia (1774.3; 95%CI: 1555.9–1992.7). After adjustment for the Gini index, periodontitis prevalence raised with a high-SBB diet (1416.0; 95%CI: 1120.2–1711.8), overweight/obesity (629.9; 95%CI: 573.1–686.8), dyslipidemia (2035.8; 95%CI: 1728.1–2343.5), and hyperglycemia (8918.1; 95%CI: 7979.8–9856.3).
Conclusions
Periodontitis has increased in Brazil since 2005, despite the smoking reduction. Sugar-sweetened beverage was the behavioral risk that mostly accompanied the periodontal trend.
Clinical relevance
Our results support upstream strategies targeting commercial, social, political, and structural determinants to tackle NCDs and reduce oral health inequities.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Noncommunicable diseases (NCDs), such as cardiovascular disease, cancers, respiratory diseases, and diabetes, are responsible for approximately 70% of deaths worldwide, comprising 85% of premature deaths in low- and middle-income countries [1]. Periodontitis is a chronic disease manifested as irreversible inflammatory destruction of teeth apparatus and is one of the most prevalent NCDs [2]. Although not directly linked to mortality, periodontitis can predict other fatal NCDs decades earlier, such as diabetes and cardiovascular diseases [3].
The American Academy of Periodontology and the European Federation of Periodontology point out that periodontitis results from the interaction between a dysbiotic microbiome and the host-dysregulated immune response. Furthermore, they recognize that smoking and diabetes are risk factors that affect the severity, extent, and treatment response of periodontitis. In contrast, obesity, physical activity, and nutrition were noted as emerging risk factors that need future confirmation as etiological factors for periodontitis [4].
Systematic reviews have shown that alcohol consumption [5], sugar intake [6], and metabolic risk factors, e.g., obesity and hyperglycemia [7], are associated with an increased risk for periodontitis. In contrast, physical activity has been associated with an opposite trend [8]. However, to the best of our knowledge, no nationally representative sample studies have investigated all of those major behavioral and metabolic risk factors for NCDs associated with the rate of periodontitis from a longitudinal perspective.
Brazil is a continental country with peculiarities that make it suitable for assessing trends in behavioral and metabolic risk factors associated with periodontal disease. Brazil's smoking rate has markedly declined over the past few years [9], resulting from an efficient tobacco control policy implemented at the end of the eighties [10]. Meanwhile, the prevalence of periodontitis in Brazil has grown above the global mean in the last three decades [11]. Besides that, other behavioral risk factors, such as added sugar and alcohol consumption, have escalated in the country [12]; so, have metabolic risk factors, i.e., overweight/obesity, hyperglycemia, hypertension, and dyslipidemia rates [9]. Sifting through the literature, studies investigating the prevalence of periodontitis and the risk factors for NCDs after all these transformations are not found. For instance, even though tobacco smoking is an acknowledged cause of periodontitis [4] and its reduction is expected to decrease the burden of periodontitis in the population, it remains uncertain whether other behavioral and metabolic risk factors can nullify the effect of a decrease in exposure to tobacco.
Thus, we hypothesize that the prevalence of periodontitis has been increasing in Brazil over the last three decades, accompanied by added sugar and alcohol consumption and, consequently, overweight/obesity, hyperglycemia, hypertension, and dyslipidemia rates, despite the smoking reduction. Accordingly, we analyzed the prevalence of periodontitis over the last three decades (1990 to 2019) in Brazilian adults and estimated the association between the burden of behavioral and metabolic risk factors with periodontitis rate.
Methods
Study design
The present study uses panel data from 26 Brazilian states from adults (25 to 49 years) over three decades (1990 to 2019). The data were obtained from the Global Burden of Disease Study 2019 (GBD) [13] and the Brazilian Institute of Geography and Statistics (IBGE). The GBD systematically quantifies global disease and risk factor burdens across 204 countries and territories, enabling comparisons over time, among populations, and across health issues. The primary source of GBD data is national or state representative surveys, and it imputes missing data [14, 15]. Supplementary Table S1 contains descriptive information about the data herein used and its source.
Outcome
The periodontal disease provided by the GBD was the prevalence rate of periodontitis (per 100,000 inhabitants), defined in the study as a Community Periodontal Treatment Needs Index (CPITN) code IV, clinical attachment loss (CAL) > 6 mm, or probing pocket depth (PPD) > 5 mm [16].
Behavioral and metabolic variables
The main behavioral and metabolic risk factors for NCDs were chosen following the World Health Organization (WHO) risk factors for NDCs [1]. Accordingly, the behavioral risk factors were smoking, alcohol use, a diet high in sugar-sweetened beverages (SSB), and low physical activity. The metabolic risk factors were high body mass index (BMI) as an overweight/obesity marker, high LDL cholesterol as an indicator of dyslipidemia, high fasting plasma glucose as a hyperglycemia surrogate, and high systolic blood pressure as a proxy of hypertension. Due to their high collinearity, each independent variable was used in separate regression models. All these variables were available as the summary exposure value (SEV). The SEV measures a population’s exposure to a risk factor that considers the intensity of exposure, whose value varies from 0% (non-exposure) to 100% (fully-exposed).
The Gini index from 2005 to 2019 (Fig. S1), which measures the distribution of the Gross Domestic Product (GDP) representing income inequality, ranging from 0 (perfect equality) to 1 (maximum inequality), was used to adjust the models.
Modeling approach
The models were fitted using fixed-effects modeling at a significance level of 0.05. State-level clustering was used to relax the autocorrelation and heteroskedasticity requirement [17]. Fixed-effect models are appropriate for assessing health outcomes because they can estimate unobservable location effects that remain fixed over time, i.e., geographic, and historical factors. Linear regressions were performed using R and RStudio.
The linear regression model consisted of a crude approach using the outcome explained by risk factors and the unobservable fixed-effect. A data matrix with 26 states × 30 years (t = 1990–2019) was used. The crude model was:
in which Periodontitis is the prevalence rate of periodontitis in a state i in year t. The RiskFactors are the SEV of the behavioral risk factors (i.e., smoking, alcohol use, a diet high in sugar-sweetened beverages, and low physical activity) and the metabolic risk factors (i.e., overweight/obesity, dyslipidemia, hyperglycemia, and hypertension). ui is the unobservable location effect, and εit is an error term.
Adjusted analysis was performed using the Gini index. As in Brazil the Gini index has not been present since 1990, and evidence suggests a disturbance in the prevalence of periodontitis estimation in Brazil around the 2000s (Fig. S2) [18], thus, regression analyses were conducted using a data matrix with 26 states × 15 years (t = 2005–2019). The Gini index was chosen because it is the longest series available for the Brazilian states in panel data format and has already been associated with health indicators in the country [19]. Hence, the adjusted regression model was:
As a sensitivity analysis, we performed models for the two main behavioral risk factors, smoking, and a diet high in SSB, in the two intervals, 1990–2005 and 2005–2019.
Prais-Winsten estimations were performed to explore trends in time series of the prevalence of periodontitis and the summarized SEV of behavioral and metabolic risk factors. The GBD gives prevalence and SEV in summary form for Brazil, thus, the data matrix analyzed were 1 country × 30 years (19902019) and 1 country × 15 years (2005–2019). Results were classified as stationary (p > 0.05), increased (β1 > 0), or decreased (β1 < 0), given a p < 0.05. Logarithmic transformation was used to reduce the variance heterogeneity of the residuals. The annual percent change (APC) was also performed using the formula: 100*(10β – 1), being β the coefficient of the Prais-Winsten regression [20].
Role of the funding source
This study was financed by the Coordination for the Improvement of Higher Education Personnel (CAPES). The funding agency did not influence the design, data collection, analysis, or publication decision. All authors had full access to the data and scientific independence to interpret them.
Results
The distribution of periodontitis in the Brazilian states among adults (25 to 49 years old) in 1990, 2005, and 2019 is depicted in Fig. 1. The prevalence of periodontitis significantly increased between 2005 to 2019 (APC: + 3.4%; 95%CI: 1.9–5.0) in Brazil. However, over the three decades, an uptrend but non-significant prevalence (APC: + 2.0%; 95%CI: -1.2–5.2) was observed. Rio de Janeiro and Rio Grande do Sul were the states that consistently showed the highest rates of periodontitis.

Prevalence rate of periodontitis in Brazilian states among adults (25 to 49 y-old), 1990, 2005, and 2019
Table 1 shows the time series for each behavioral and metabolic risk factor in Brazil. There was an increase in the SEV of diet high in SSB (APC: + 2.4%; 95%CI: 1.9–2.8) and alcohol use (APC: + 1.5%; 95%CI: 0.9–2.2), in addition to the SEV of overweight/obesity (APC: + 9.9%; 95%CI: 8.7–9.3), dyslipidemia (APC: + 1.1%; 95%CI: 1.0–1.1) and hyperglycemia (APC: + 3.1%; 95%CI: 2.2–4.1) over the three decades. The SEV of smoking decreased from 14.9% in 1990 to 6.3% (APC: -6.7%; 95%CI: -7.8–-5.5). From 2005 to 2019, among the SEV of behavioral factors, only a diet high in SSB (APC: + 1.3%; 95%CI: 1.1–1.5) increased, whereas smoking decreased (APC: -9.5%; 95%CI: -9.7– -9.2). In this period, all SEV of metabolic risk factors increased in the country, mainly overweight/obesity (APC: + 4.6%; 95%CI: 3.5–5.7). Figure 2 displays the time series of behavioral and metabolic risk factors by state. An upward trajectory of SSB consumption was observed across all states, in contrast to smoking trends. Notably, the states of São Paulo, Rio de Janeiro, and Rio Grande do Sul exhibited the highest rates of SSB consumption in Brazil.

Summary exposure value of behavioral and metabolic risk factors in Brazilian states among adults (25 to 49 years) between 1990 and 2019
In the crude regression models, the SEV of behavioral risk factors alcohol use (365.5; 95%CI: 2307.9–2782.3), diet high in SSB (365.5; 95%CI: 322.5–408.4), and low physical activity (1784.4; 95%CI: 763.7–2805.0), and the metabolic risk factors overweight/obesity (172.3; 95%CI: 156.3–188.4), dyslipidemia (734.5; 95%CI: 624.7–844.2), and hyperglycemia (1774.3; 95%CI: 1555.9–1992.7) were positively associated with an increase in the prevalence of periodontitis in Brazil. Conversely, the SEV of smoking was negatively associated with periodontitis prevalence (-398.3; 95%CI: -473.6 – -323.0) over the study period. The linear regression coefficients are given in Table 2.
Regarding the behavioral risk factors, when the models were adjusted for the Gini index (2005–2019), an increase in the prevalence rate of periodontitis was observed for each percentage increase in the SEV of a diet high in SBB (1416.0; 95%CI: 1120.2–1711.8). The SEV of smoking was negatively associated with the prevalence of periodontitis (-1103.9; 95%CI: -1433.2– -774.5). Concerning the metabolic risk factors, an increase in the prevalence rate of periodontitis accompanied the percentage increase in the SEV of overweight/obesity (629.9; 95%CI: 573.1–686.8), dyslipidemia (2035.8; 95%CI: 1728.1–2343.5), and hyperglycemia (8918.1; 95%CI: 7979.8–9856.3). The linear regression coefficients for behavioral and metabolic risk factors adjusted for the Gini index from 2005 to 2019 are described in Table 3. The sensitivity analysis for smoking and SSB consumption in the two intervals (1990–2005 and 2005–2019) yielded consistent results (Table S2).
Discussion
Periodontitis rates have increased significantly among Brazilians since 2005, similar to increased consumption of sugar-sweetened beverages, overweight/obesity, dyslipidemia, and hyperglycemia. Furthermore, the prevalence of periodontitis rose despite the reduction of smoking. These findings reinforce the hypothesis that reducing smoking alone is not enough to reduce periodontitis burden. This study has the advantage of using the GBD database, providing complete and standardized data, and making it possible to compare population parameters over time in panel analysis.
The prevalence of periodontitis has been linked to the consumption of SSBs in Brazil. This observation may be endorsed by the highest rates of periodontitis in the states of Rio de Janeiro and Rio Grande do Sul, which also have consistently exhibited elevated levels of SSB consumption. Trend analyses showed that sugar-sweetened beverages' consumption rates increased significantly in Brazil over the three decades analyzed. These beverages are the primary source of discretionary calories in the Western diet. Sugar-sweetened beverages have been associated with metabolic risks such as obesity, insulin resistance, and hypertension [21]. Sustained insulin resistance leads the liver into de novo lipogenesis and consequent low-grade inflammation [22]. Increasing evidence points to the role of reactive oxygen species in establishing an oxidative stress environment that underlies the pathogenesis of periodontitis [23]. Periodontitis is highly prevalent in patients with type 2 diabetes, smoking habits, and obesity. Moreover, sugar consumption has been associated with cardiovascular risk [24] and also periodontal disease in adolescents [25] and young adults [26]. Poor dietary habits can worsen clinical periodontal parameters, contributing to oral dysbiosis. Sugars function as local stressors for the oral biofilm, which can create a highly proteic feeding environment for gram-negative bacterial species [27]. Inflammation-induced loss of periodontal tissue further exacerbates this situation. Other causative factors such as genetic factors and smoking may also contribute to periodontal lesion chronification, leading to a positive feedback loop that can worsen the deterioration of the tooth apparatus [28].
Our results from the crude analysis showed that an increase in alcohol consumption was associated with an increase in periodontitis burden over the last three decades, previous corroborating findings, including among Brazilians [29]. Alcohol use may reduce the immune response, favoring periodontitis development probably through maladaptive immunity [30]. Additionally, liver inflammation via acetaldehyde production may be observed, inducing de novo lipogenesis, and promoting hepatic insulin resistance, dyslipidemia, and hepatic steatosis, similar to the effects caused by added fructose [22]. Thus, alcohol use may result in or hasten low-grade systemic inflammation with oral consequences [22]. However, the alcohol use loss association after the model adjustment for the Gini index. Some hypotheses could explain this finding. First, the stationarity rate of alcohol use in the analyzed period (Table 1) could mask the association. Second, improving the Gini index (Fig. S1) in Brazil could mitigate the effects of alcohol consumption on periodontitis in the population since the alcohol harm paradox emphasizes that disadvantaged groups would be more exposed to alcohol-related problems [31]. Third, it is known that there is a consistent relationship between alcohol and periodontitis among males [5], whereas this study used an indicator for both sexes combined.
Similarly, low physical activity was also significantly associated in crude analysis with periodontitis prevalence. Physical activity could reduce the prevalence of periodontitis by reducing systemic inflammatory levels [8]. A study with obese individuals showed that weight loss induced by physical activity and a healthy diet might increase the expression of adiponectin receptors in adipose tissue and skeletal muscles [32]; an essential hormone regulator of insulin sensitivity and a biomarker for the risk of NCDs. However, the low physical activity rate in the Brazilian population did not account for the increase in periodontitis after adjustment for the Gini index. We suppose that the stationary level of this indicator between 2005 and 2019 was responsible for the loss of association after adjustment (Fig. 2 and Table 1).
Increased overweight/obesity also explained a greater periodontitis burden with the highest magnitude of association (R2 within = 0.920) among all the explored metabolic risk factors. In this sense, studies hypothesize that the white adipose tissue secretes adipocytokines, which, combined with the hypoxia caused by the expanded adipose tissue [33], could alter the innate immune response, increasing the susceptibility to inflammation and bacterial infections in periodontitis [34]. Since metabolic alterations are usually associated, hyperglycemia and dyslipidemia also explained the increase in periodontitis from 2005 to 2019 (R2 within > 0.820). A previous study has shown their association with periodontal disease [35]. Data suggest that the odds of periodontitis increase with the number of components of the metabolic syndrome present in an individual [35]. In fact, the progress of a hyperglycemic state together with a dyslipidemic profile can result in periodontal inflammation caused by systemic oxidative stress and a cascade of cytokines resulting from this process [23].
Surprisingly, our results demonstrate an inverse relationship, with periodontitis burden increasing despite reduced smoking rates. This unexpected outcome is likely linked to a substantial reduction in smoking (-58.14%) driven by Brazil's anti-smoking policies initiated in the 1980s [10]. The data suggests that targeting smoking reduction alone may not effectively mitigate the burden of periodontitis within the population, as it continued to rise. Therefore, we emphasize the necessity of proposing population-level policies addressing other behavioral and metabolic risk factors. In addition to the variables examined in this study, it is essential to contextualize the observed increase in periodontitis in Brazil during the study period. Various factors may have contributed to this trend, including dietary changes, such as the rise in ultra-processed foods [36, 37], limited access to dental care services, especially in underserved areas [38], as well as socio-economic and cultural factors.
Our findings support upstream strategies targeting commercial, social, political, and structural determinants to tackle NCDs and also reduce oral health inequities. For example, regulatory market policies, labeling, and taxation of products rich in added sugars in connection with subsidies to encourage a healthy diet including more fruits and vegetables can be efficient measures to tackle and prevent NDCs, as learned from the smoking case, whose reduction was associated with a lower periodontitis burden.
As limitations, our findings may be affected by underreporting some indicators since we used secondary data. The primary data source for the GBD information is national or state surveys and missing data are estimated using a smoothing algorithm designed for the database. Additionally, the use of ecological data from Brazilian states for linear regression may not allow for individual-level interpretations due to potential ecological fallacy. Given the close relationship of the conditions under study (periodontitis, behavioral, and metabolic risk factors) to socioeconomic inequalities, our aggregate-level data provide average estimates for both poor and wealthy individuals, requiring cautious interpretation. Despite nearly 30 years of data, our approach may not fully capture the chronic nature of these conditions, particularly periodontitis. The influence of risk factors may require a time lag to manifest, necessitating longer analysis periods to assess cumulative effects fully. Lastly, causal inferences should not be drawn from our study, as despite using fixed effects and control variables, the presence of unobserved time-varying confounding factors cannot be entirely ruled out.
The rate of periodontitis has been increasing in Brazil since 2005, despite the smoking reduction. Sugar-sweetened beverage consumption was the behavioral risk factor that best explained this trend in Brazilians. This behavior is parallelly related to the increased accumulation of exposures to metabolic alterations, thus nullifying the beneficial effect of tobacco reduction. Therefore, interventions on upstream determinants of NDCs are of utmost importance to control metabolic and behavioral risk factors that influence periodontitis rates.
Data Availability
The data utilized in this study is publicly available and can be freely accessed for download from https://vizhub.healthdata.org/gbd-results/ and https://sidra.ibge.gov.br/tabela/5939.
References
World Health Organization (2021) Noncommunicable diseases. In: World Health Organization. https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases. Accessed 13 Jan 2022
Peres MA, Macpherson LMD, Weyant RJ et al (2019) Oral diseases: a global public health challenge. The Lancet 394:249–260. https://doi.org/10.1016/S0140-6736(19)31146-8
Bengtsson VW, Persson GR, Berglund JS, Renvert S (2021) Periodontitis related to cardiovascular events and mortality: a long-time longitudinal study. Clin Oral Investig 25:4085–4095
Tonetti MS, Greenwell H, Kornman KS (2018) Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J Periodontol 89:S159–S172. https://doi.org/10.1002/JPER.18-0006
Pulikkotil SJ, Nath S, Muthukumaraswamy et al (2020) Alcohol consumption is associated with periodontitis. A systematic review and meta-analysis of observational studies. Community Dent Health 37:12–21. https://doi.org/10.1922/CDH_4569Pulikkotil10
Gupta V, Dawar A, Bhadauria US et al (2022) Sugar-sweetened beverages and periodontal disease: A systematic review. Oral Dis. https://doi.org/10.1111/ODI.14368
Salamonowicz M, Zalewska A, Maciejczyk M (2019) Oral consequences of obesity and metabolic syndrome in children and adolescents. Dent Med Probl 56:97–104. https://doi.org/10.17219/dmp/102620
Railson de Ferreira O, Corrêa MG, Magno MB et al (2019) Physical activity reduces the prevalence of periodontal disease: Systematic review and meta-analysis. Front Physiol 10:234. https://doi.org/10.3389/fphys.2019.00234
Gaspar RS, Rezende LFM, Laurindo FRM (2022) Analysing the impact of modifiable risk factors on cardiovascular disease mortality in Brazil. PLoS ONE 17:e0269549. https://doi.org/10.1371/journal.pone.0269549
Portes LH, Machado CV, Turci SRB et al (2018) Tobacco Control Policies in Brazil: a 30-year assessment. Ciênc Saúde Colet 23:1837–1848. https://doi.org/10.1590/1413-81232018236.05202018
Chen MX, Zhong YJ, Dong QQ et al (2021) Global, regional, and national burden of severe periodontitis, 1990–2019: An analysis of the Global Burden of Disease Study 2019. J Clin Periodontol 48:1165–1188. https://doi.org/10.1111/jcpe.13506
Bryazka D, Reitsma MB, Griswold MG et al (2022) Population-level risks of alcohol consumption by amount, geography, age, sex, and year: a systematic analysis for the Global Burden of Disease Study 2020. The Lancet 400:185–235. https://doi.org/10.1016/S0140-6736(22)00847-9
Global Burden of Disease Collaborative Network (2020) Global Burden of Disease Study 2019 (GBD 2019) Results. https://vizhub.healthdata.org/gbd-results/. Accessed 22 Oct 2023
Vos T, Lim SS, Abbafati C et al (2020) Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet 396:1204–1222. https://doi.org/10.1016/S0140-6736(20)30925-9
Murray CJL, Aravkin AY, Zheng P et al (2020) Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet 396:1223–1249. https://doi.org/10.1016/S0140-6736(20)30752-2
Global Burden of Disease Collaborative Network (2020) Periodontal diseases — Level 4 cause. In: Institute for Health Metrics and Evaluation. https://www.healthdata.org/results/gbd_summaries/2019/periodontal-diseases-level-4-cause. Accessed 22 Oct 2023
Abadie A, Athey S, Imbens GW, Wooldridge JM (2022) When should you adjust standard errors for clustering? Q J Econ 138:1–35. https://doi.org/10.1093/qje/qjac038
Costa Junior S da, Araujo PG, Frichembruder K, Hugo FN (2021) Brazilian Oral Health Policy: metasynthesis of studies on the Oral Health Network. Rev Saúde Pública 55:105. https://doi.org/10.11606/s1518-8787.2021055003454
Gaspar RS, Rossi L, Hone T, Dornelles AZ (2021) Income inequality and non-communicable disease mortality and morbidity in Brazil States: a longitudinal analysis 2002–2017. Lancet Reg Health - Am 2:100042. https://doi.org/10.1016/j.lana.2021.100042
Antunes JLF, Cardoso MRA (2015) Using time series analysis in epidemiological studies. Epidemiol Serv Saúde 24:565–576. https://doi.org/10.5123/S1679-49742015000300024
Lana A, Rodríguez-Artalejo F, Lopez-Garcia E (2014) Consumption of sugar-sweetened beverages is positively related to insulin resistance and higher plasma leptin concentrations in men and nonoverweight women. J Nutr 144:1099–1105. https://doi.org/10.3945/JN.114.195230
Lustig RH (2010) Fructose: Metabolic, Hedonic, and Societal Parallels with Ethanol. J Am Diet Assoc 110:1307–1321. https://doi.org/10.1016/j.jada.2010.06.008
Sczepanik FSC, Grossi ML, Casati M et al (2020) Periodontitis is an inflammatory disease of oxidative stress: We should treat it that way. Periodontology 2000 84:45–68. https://doi.org/10.1111/prd.12342
Johnson RK, Appel LJ, Brands M et al (2009) Dietary Sugars Intake and Cardiovascular Health. Circulation 120:1011–1020. https://doi.org/10.1161/CIRCULATIONAHA.109.192627
Moreira ARO, Batista RFL, Ladeira LLC et al (2021) Higher sugar intake is associated with periodontal disease in adolescents. Clin Oral Investig 25:983–991. https://doi.org/10.1007/s00784-020-03387-1
Lula ECO, Ribeiro CCC, Hugo FN et al (2014) Added sugars and periodontal disease in young adults: an analysis of NHANES III data. Am J Clin Nutr 100:1182–1187. https://doi.org/10.3945/ajcn.114.089656
Hajishengallis G (2014) The inflammophilic character of the periodontitis-associated microbiota. Mol Oral Microbiol 29:248–257. https://doi.org/10.1111/omi.12065
Loos BG, Van Dyke TE (2020) The role of inflammation and genetics in periodontal disease. Periodontology 2000 83:26. https://doi.org/10.1111/PRD.12297
Susin C, Wagner MC, Haas AN et al (2015) The association between alcohol consumption and periodontitis in southern Brazilian adults. J Periodontal Res 50:622–628. https://doi.org/10.1111/jre.12242
Liangpunsakul S, Toh E, Ross RA et al (2017) Quantity of alcohol drinking positively correlates with serum levels of endotoxin and markers of monocyte activation. Sci Rep 7:4462. https://doi.org/10.1038/s41598-017-04669-7
Boyd J, Sexton O, Angus C et al (2022) Causal mechanisms proposed for the alcohol harm paradox—a systematic review. Addiction 117:33–56. https://doi.org/10.1111/add.15567
Christiansen T, Paulsen SK, Bruun JM et al (2010) Diet-induced weight loss and exercise alone and in combination enhance the expression of adiponectin receptors in adipose tissue and skeletal muscle, but only diet-induced weight loss enhanced circulating adiponectin. J Clin Endocrinol Metab 95:911–919. https://doi.org/10.1210/jc.2008-2505
Guerreiro VA, Carvalho D, Freitas P (2022) Obesity, adipose tissue, and inflammation answered in questions. J Obes 2022:1–11. https://doi.org/10.1155/2022/2252516
Iwashita M, Hayashi M, Nishimura Y, Yamashita A (2021) The link between periodontal inflammation and obesity. Curr Oral Health Rep 8:76–83. https://doi.org/10.1007/S40496-021-00296-4
Lamster IB, Pagan M (2017) Periodontal disease and the metabolic syndrome. Int Dent J 67:67–77. https://doi.org/10.1111/IDJ.12264
Cassiano LS, Peres MA, Motta JVS et al (2022) Periodontitis is associated with consumption of processed and ultra-processed foods: findings from a population-based study. Nutrients 14:3735. https://doi.org/10.3390/nu14183735
da Costa Louzada ML, Martins APB, Canella DS et al (2015) Ultra-processed foods and the nutritional dietary profile in Brazil. Rev Saude Publica 49:38. https://doi.org/10.1590/S0034-8910.2015049006132
Bastos TF, de Paula Barbosa Medina L, da Silva Sousa NF et al (2019) Income inequalities in oral health and access to dental services in the Brazilian population: National health survey, 2013. Rev Bras Epidemiol 22:E190015.SUPL.2. https://doi.org/10.1590/1980-549720190015.supl.2
Acknowledgements
This study received support from the Coordination for the Improvement of Higher Education Personnel (CAPES). SAC was funded by PROCAD-Amazônia 8881.200487/2018-01 and PDPG-Amazônia Legal 0810/2020/88881.510244/2020-01. LLCL was supported by CAPES Finance Code 001, and FLS received funding from PDPG-Amazônia Legal 0810/2020/88881.510244/2020-01.
Funding
Open access funding provided by Royal Danish Library, Aarhus University Library GBD was supported by the Bill and Melinda Gates Foundation. Scholarships were provided by the Coordination for the Improvement of Higher Education Personnel (CAPES): SAC received funding from PROCAD-Amazônia 8881.200487/2018-01 and PDPG-Amazônia Legal 0810/2020/88881.510244/2020-01, LLCL was funded by CAPES Finance Code 001, and FLS received funding from PDPG-Amazônia Legal 0810/2020/88881.510244/2020-01.
Author information
Authors and Affiliations
Contributions
SAC designed, performed statistical analyses, and wrote the manuscript; FRMLL designed, wrote the manuscript, and revised its final version; LLCL designed and wrote the manuscript; FLS designed and revised its final version; AMAP designed and revised its final version; BFS performed statistical analyses and revised its final version; GGN designed, performed statistical interpretation, and wrote the manuscript; CCCR coordinated the study, designed, performed statistical interpretation, wrote the manuscript. All authors contributed to the editing and approval of the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The University of Washington research ethics committee has approved the GBD study protocol. The GBD was performed in accordance with all relevant federal, state, and local laws, as well as University of Washington regulations and procedures. Participant consent does not apply to this study.
Conflict of interests
The authors declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Alves-Costa, S., Leite, F.R.M., Ladeira, L.L.C. et al. Behavioral and metabolic risk factors associated with periodontitis in Brazil, 1990–2019: a multidimensional analysis for the Global Burden of Disease Study 2019. Clin Oral Invest 27, 7909–7917 (2023). https://doi.org/10.1007/s00784-023-05384-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-023-05384-6