
Abstract
Objectives
To compare blood flow (BF) changes of teeth subjected to orthodontic forces during curve of Spee (COS) leveling using different archwires (AW).
Material and methods
Thirty subjects with COS > 5 mm were randomly assigned (1:1:1) into three groups based on the AW used: group 1: 0.017 × 0.025-inch stainless-steel (SS)AW, group 2: 0.019 × 0.025-inch SSAW, and group 3: 0.021 × 0.025-inch β-titanium (TMA)AW. In the 3 groups, a 5 mm-depth reverse COS was placed in the AWs. A laser Doppler flowmeter was used to measure BF at different time intervals (T0–T4).
Results
In the 3 AWs group, BF of all measured teeth was reduced 20 min after force application. Afterwards, the BF values started to increase until the baseline values were almost restored within 1 week. Differences in BF changes between the extrusion and intrusion subgroups were observed within groups 1 and 3 during the first 20 min of force application (P < 0.05). Similar BF changes were recorded using the 3 different AWs. BF changes were associated with tooth type and the amount of COS depth change.
Conclusions
During CoS leveling, similar BF changes were recorded using the 3 different AWs. Tooth type and the amount of COS depth change were associated with BF changes within the first 20 min of force application. Greater BF reduction was found in premolars compared to incisors during the first 20 min of AW placement.
Clinical relevance
It is important to select a type of applied forces that minimally affect the BF. Intrusive forces appeared to have lower negative effects on the BF of teeth during COS leveling.
Trial registration
ClinicalTrial.gov (# NCT04549948).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The curve of Spee (COS) refers to the upward progression of the teeth curvature from the incisors through the premolars and molars. A deep COS is usually associated with an increased anterior overbite. During orthodontic treatment, COS is leveled by bringing the incisal edges of the anterior teeth and the buccal cusps of the posterior teeth into a horizontal plane level [1].
The COS correction is usually achieved by posterior teeth extrusion and lower incisor intrusion [2,3,4]. A randomized clinical trial conducted by Nasrawi et al. [5] to measure the vertical movement for the lower incisors and lower molars associated with leveling excessive COS using 3 different archwire (AW) sizes concluded that leveling the COS was achieved in all groups by incisor intrusion, molar extrusion, and incisor proclination on different levels.
The application of orthodontic forces to teeth has been reported to induce molecular changes in the cells of the periodontal ligament, alveolar bone, and the pulp–dentine complex [6, 7].
The application of a contentious force to the teeth not only results in an inflammatory reaction within the periodontium but also has a significant effect on pulpal neural responsiveness, possibly for the entire duration of the orthodontic treatment [8]. Several methods have been suggested to investigate the pulpal response to an applied force. Histological observation [6, 7], fluorescent microsphere injection, and measurement of pulp tissue respiration rate may only be applied following tooth extraction. Laser Doppler flowmetry (LDF) is a noninvasive method that can be used to obtain repeated measurements of blood flow (BF) without causing tissue damage [9]. The blood flow signals from intact teeth measured by the LDF contain information of alteration in the BF. Therefore, the technique has been used to evaluate alterations in the BF during orthodontic movements in humans [10].
Most alterations in the BF that result from orthodontic treatment are reversible unless the pulp has been previously irritated by caries, restorations, or trauma [11]. Rarely, pulpal side effects may occur, including altered pulpal respiration rate, internal root resorption, pulp obliteration, and pulpal necrosis [12]. The characteristics of the applied orthodontic forces, such as the type, magnitude, force duration, and distribution, could contribute to blood flow disturbance [6, 12,13,14] and make the alteration reversible or irreversible. It is unanimously accepted that dental pulp changes are directly proportional to the applied forces; therefore, in adults it has to be between 50 and 100 cN [15]. High forces increase the risk of radicular resorption by raising the hyalinization of the periodontal tissue and inducing very sharp peaks of rises and falls in the cytokine levels which lead to undesirable effects on the tissues including the pulp [16], whereas light and continuous forces maintain high cytokine levels, which are necessary for continuous periodontal remodeling, for a longer time [17].
Intrusion applied to the teeth during orthodontic treatment is thought to have the greatest impact on the apical region. Therefore, a significant reduction in the BF during the application of a continuous intrusive force is expected. This is substantiated by results from trauma studies where intrusion injuries cause the highest percentage of pulp necrosis particularly in teeth with closed apices, compared to other luxation injuries [18]. Brodin et al. [10] measured the effect of tooth intrusion and extrusion on BF of human incisors (6 subjects). They reported that extrusion of the teeth gave no significant changes in BF during loading or unloading, while intrusion of the teeth reduced the BF by 20% during the first minute after force application. Subsequently the BF gradually increased and returned to the pre-stimulus level 3 min after unloading.
On the other hand, Sabuncuoglu and Ersahan [19] showed that BF decreased in the incisor teeth when subjected to 3 days of either light (40 g) or heavy (120 g) orthodontic intrusion, and the BF values returned to their baseline levels after 3 weeks of either light (40 g) or heavy (120 g) intrusion. Similarly, they demonstrated a short-term regressive change in BF during continuous molar intrusion with mini-implants, which tended to return to baseline values by the end of the observation period (6 months) [15]. Furthermore, Wu et al. [20] reported that the use of larger dimension AW increased the pressure stresses on the periodontal ligament and the alveolar bone, which might add to the risk of root resorption and irreversible pulp changes.
In the current orthodontic practice, 0.17 × 0.025-inch stainless steel (SS), 0.019 × 0.025-inch (SS), and 0.021 × 0.025-inch β-titanium (TMA) AWs are used for COS leveling during orthodontic treatment [5]. The smaller AW/bracket-slot play when 0.021 × 0.025-inch TMA AW is used has the advantage of more torque control and a less low incisor proclination during leveling. However, the effect of using larger AW dimensions with high frictional forces on pulp tissues during orthodontic treatment is not known yet. Therefore, it was assumed that the type and size of the AW might have a different impact on the BF during COS leveling with intrusive and extrusive forces. The previously reported studies regarding BF changes during extrusion and intrusion orthodontic forces were performed on individual teeth (incisors or upper molars), and to date, there are no published studies evaluating BF during lower arch leveling with lower molar extrusion and lower incisor intrusion using different sized orthodontic AW. Therefore, to determine whether alterations in the BF of anterior and posterior teeth during arch leveling using continuous AW with reverse COS could affect the long-term vitality of teeth, this study was conducted with the following objectives:
-
1-
To investigate BF changes of incisors subjected to orthodontic intrusive force during COS leveling using 0.017 × 0.025-inch stainless steel (SS) AW, 0.019 × 0.025-inch SS AW, and 0.021 × 0.025-inch β-titanium Titanium (TMA) AW at different time points (20 min, 48 h, 1 week, 1 month)
-
2-
To investigate BF changes of molars and premolars subjected to orthodontic extrusive force during COS leveling using 0.017 × 0.025-inch SS AW, 0.019 × 0.025-inch SS AW, and 0.021 × 0.025-inch TMA AW at the above 4 time points
-
3-
To compare BF changes based on tooth type and type of force (intrusive and extrusive forces) within the same AW size group
-
4-
To compare BF changes between teeth in the three different AW size groups as per tooth type and type of force
-
5-
To investigate the association between BF changes, type of force, AW type, tooth type, and the amount of change in COS
Null hypothesis
There is no significant difference in BF changes between intrusive and extrusive forces during COS leveling regardless of the AW used: 0.017 × 0.025-inch SS AW, 0.019 × 0.025-inch SS AW, and 0.021 × 0.025-inch TMA AW.
Material and methods
Study design
This study was a randomized clinical trial with a 1:1:1 allocation ratio. The methods were not changed after trial initiation. The study was approved by the Institutional Review Board at the Jordan University of Science and Technology (approval number 78/117/2018). This trial was registered with ClinicalTrial.gov with identifier number NCT04549948.
The sample size was calculated using the G*power 3.1.9 program. Univariate analysis revealed significant variability between subjects (F = 4.45, P = 0.017, Partial Eta Squared = 0.15). Assuming a medium effect size difference (0.4) between groups, power analysis yielded a total sample size estimate of 14 subjects (7 patients per group) at a conventional alpha level (0.05) and desired power (1 – β) of 0.95. To build up for an attrition rate of 10%, initial recruitment targeted a total of 8 patients/group.
The participants for this study were recruited from patients attending postgraduate orthodontic clinics. All subjects who agreed to participate in the study signed a consent form for participation after clarifying the purpose of the intervention. Subjects were selected based on the inclusion criteria: age ≥ 16 years and ≤ 25 years, normally inclined or retroclined lower incisors, presence of deep bite, depth of COS ≥ 5 mm, non-extraction treatment plan, averaged or reduced lower vertical height, good oral hygiene, and healthy periodontium, and all permanent teeth are present except for the third molars.
Exclusion criteria were history of previous orthodontic treatment, teeth with root resorption, endodontically treated teeth, history of previous trauma, restoration on measured teeth, presence of a medical condition or being under medication that could affect the treatment, and smoking.
After recruiting patients who met the inclusion criteria and just before the insertion of the leveling AWs, the intervention was randomly allocated using the permuted random block size of 3 with a 1:1:1 allocation ratio by one research assistant (S.D.). The allocation sequence was concealed from the researcher (Y.N.) by sequentially numbered, opaque, sealed, and stapled envelopes before the intervention. Patients were then asked to pick a sealed envelope to assign the method of intervention. The methods were not changed after trial initiation. The patient was blinded to the intervention used, but it was not possible to blind the clinician during treatment. However, the measurements of the BF were performed by one research assistant (H.D.) who was blinded to the type of intervention used.
Intervention
Thirty patients aged from 18 to 25 years who required fixed appliance orthodontic treatment were selected to participate in the study. All subjects were treated by the same orthodontic resident (Y.N.) using a pre-adjusted edgewise fixed appliance on upper and lower arches without extraction (American Orthodontics, 0.022 × 0.028-inch Roth prescription brackets). All AWs were ovoid in shape from 3 M Unetik company (Monrovia, California). A standardized bonding technique was applied according to the manufacturer’s instructions, and vertical bracket positioning was done using bracket gauge (4 mm from incisal tip for incisors, 4.5 mm from occlusal tip for canines and premolars).
Teeth alignment started with round 0.016-inch Nickel Titanium (NiTi) AW which included the upper and lower second molars, and then a sequence of 0.018-inch-NiTi and 0.016 × 0.022-inch-NiTi was inserted before 0.017 × 0.025-inch-NiTi AWs were reached. Appointment visits were the same for all patients during the intervention (every 4 weeks). After alignment and before the insertion of the reverse COS leveling Aws, an alginate impression for lower arch was taken for all patients at this time point (T0: before leveling).
Afterward, and based on their allocation group, 3 different leveling continuous AWs were inserted as follows:
-
Group 1: Leveling of COS using 0.017 × 0.025-inch SS AW
-
Group 2: Leveling of COS using 0.019 × 0.025-inch SS AW
-
Group 3: Leveling of COS using 0.021 × 0.025-inch TMA AW
In the 3 studied groups, a 5 mm depth reversed COS was placed in the interventional AWs using tweed plier distal to lower canines. Measurement of the applied reverse COS in the AWs was done using digital caliper and inserted without a cinch-back. The anterior labial crown torque was removed from all AWs by holding the AWs mesial to the first premolars with a pair of tweed pliers and “twisting’’ the AWs to achieve a zero torque “flat” surface anteriorly. This was further checked by holding the tweed pliers at the anterior and posterior segments of the AWs and observing the lack of torque anteriorly. All teeth were included in the fixed orthodontic appliance including lower second molars. Patients were instructed to contact the clinic within 24 h if any bracket debonded. After 1 month, an alginate impression was taken for the lower arch, and the COS change was recorded. Utility wax was used to cover the lower arch brackets so as not to distort the impression upon removal from the mouth.
Outcomes
Primary outcome: blood flow (BF) (Fig. 1)

BF measurement using LDF (courtesy of Alhaija et al. 2021) [36]
Measurements of the BF were taken by the use of LDF (Moor lab, Moor instruments, UK) with a wavelength of 780 nm and a dental probe MP 13 (Moor instruments, UK; 2 fibers, 0.25 mm diameter, centers 0.5 mm spaced a part). The flowmeter was calibrated according to the manufacturer’s instructions. Room temperature was maintained from 20 to 25 °C. Volunteers were provided with 15 min’ rest before each session.
Before starting the measurements, a silicone splint was fabricated to stabilize the dental probe during the measurements. The retentive areas of the brackets were covered with a layer of utility wax. Holes were made below the imprints of the brackets in the mold with a stainless-steel drill of 1.5 mm diameter to allow the probe to pass through the mold to touch the teeth to allow measurement of teeth on the same position at different times. The silicone splints were fabricated to extend over the attached gingiva. The retentive areas of the brackets and the labial gingiva were covered with utility wax. In addition, 4 cotton rolls were applied in the gingival sulcus to keep the lower lip and cheeks away. This helped in isolating the teeth during measurements to minimize contamination of the blood flow signals from adjacent tissues [21].
BF was recorded at 5 points:
-
1-
Before placement of interventional AWs in both groups. These values were considered the basal blood flow (T0).
-
2-
Twenty minutes after placement of the interventional AW (T1).
-
3-
Forty-eight hours after placement of the interventional AW (T2).
-
4-
One week after placement of the interventional AW (T3).
-
5-
One month after placement of the interventional AW (T4).
Secondary outcome: depth of COS
The depth of COS was measured manually just before the placement of interventional AW and at the end of the intervention (1 month) using a digital caliper as the perpendicular distance between the deepest cusp tip and a flat plane that was laid on top of the mandibular dental cast, touching the incisal edges of the central incisors and the distal cusp tips of the second molars. It was measured on the right and left sides of the mandibular arch, and the average value was included in the analysis. All dental casts were trimmed and mounted equally on a dental surveyor to ensure accurate results.
Method error
Measurement error using Dahlberg formula and Houston’s coefficient of reliability was calculated. Dahlberg error was 0.6 PU for BF and 0.1 mm for COS, and the coefficients of reliability were above 88% indicating substantial agreement.
Statistical analysis
Data analysis was carried out using SPSS (28.0, SPSS Inc., NY, USA). Descriptive statistics for BF and COS depth at different time intervals were calculated. The Shapiro–Wilk test was applied to assess the normality of numeric data, and the result indicated that data were not normally distributed. The Wilcoxon signed-rank test was applied to detect differences between the right and left sides. The non-parametric Friedman test with a pairwise comparison of related samples and Bonferroni correction for multiple tests was applied to examine within-group differences in BF at the different time points. Kruskal–Wallis H test was used to detect differences between groups (AW groups and type of force subgroups). Linear regression analysis was applied to determine any association between BF changes within the first 20 min and the first 48 h of force application and AW size, type of force, tooth type, and the COS depth change. The P-value was set at 0.05 level.
Results
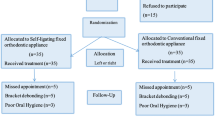
Thirty subjects (20 females and 10 males) received the planned intervention. Complete records for all subjects were available during the analysis stage. The age averaged 21.60 (3.62) years, 23.50 (4.66) years, and 20.20 (2.51) years in groups 1, 2, and 3, respectively. Before the intervention, the lower incisors’ inclination was 94.8 (3.7), 92.5 (4.0), and 93.4 (3.6) degrees, and the maxillary/mandibular plane angle was 24.1 (4.3), 24.6 (4.8), and 23.9 (2.9) degrees in groups 1, 2, and 3, respectively (P > 0.05). The participants’ flowchart is presented in Fig. 2. At T0, there were 30 subjects. None of the subjects were excluded from the analysis, and at the final analysis stage (T4), there was full data for 30 patients (10/group). Negative outcomes were not reported by any patients during the trial.

CONSORT flow chart showing patients’ flow during the trial
Teeth on both sides were assessed. The Wilcoxon signed-rank test revealed no significant differences in BF changes between the right and left sides within each group. Therefore, the right and left sides were averaged, and the mean BF values were used in the final analysis. The results are presented according to tooth type and type of applied force. The incisors were analyzed in the intrusion group (total of 60 teeth/20 teeth in each AW group), while the extrusion group was subdivided into 2 subgroups: premolars only (total of 60 teeth/20 teeth in each AW group) and first molars only as the second subgroup (total of 30 teeth/10 teeth in each AW group).
Primary outcome
Based on tooth type
The medians and the interquartile range (IQR) for the BF measurements per tooth type are shown in Table 1. At T0, the BF values ranged from 2.15 mm/s in central incisors to 3.09 mm/s in the first molars. At T1, it dropped and ranged from 1.74 mm/s in central incisors to 2.41 mm/s in the first molars. At T4, it ranged from 2.21 mm/s in central incisors to 3.48 mm/s in the lateral incisor tooth.
Comparisons of BF changes within and between the different AW groups according to type of tooth are presented in Table 2. In the 3 AWs group, BF of all measured teeth was reduced 20 min after force application. However, a statistically significant reduction was reached in the first molars and canines in group 1, in all teeth except the lateral incisors in group 2, and in all teeth except canines and lateral incisors in group 3. Afterwards, the BF values started to increase until the baseline values were almost restored within 1 week. Later, BF values increased more than their baseline values but did not reach any statistically significant level (P > 0.05).
Similar BF changes were observed after the application of orthodontic force using different AW sizes and materials except for the lower canines, where it showed more reduction (− 3.11 mm/s and − 2.48 mm/s in groups 1 and 2, respectively) and more recovery (1.13 mm/s and 1.69 mm/s) in SS groups compared to the TMA group (− 2.76 mm/s and 0.35 mm/s) (P < 0.05).
Based on force type
The medians and the IQR for the BF measurements per type of force applied are shown in Table 3. At T0, the BF values ranged from 2.23 mm/s in the intrusion group to 3.01 in the extrusion group. At T1, the BF values dropped and ranged from 1.80 mm/s in the intrusion group to 2.41 mm/s in the extrusion group. At T4, it increased and ranged from 2.35 mm/s in the intrusion group to 3.18 mm/s in the extrusion group.
Comparisons of BF changes within and between the different AW groups according to type of applied force are presented in Table 4.
Within the same AW group at the different time intervals, similar BF changes were found within the first 20 min of intrusion and extrusion force application. In group 1, BF values were restored within 1 week, whereas it continued to increase in the 0.019 × 0.025-inch SS group (premolar extrusion subgroup), and in the TMA group (premolar extrusion and the incisor intrusion subgroups).
Within the same AW groups, when the extrusion and intrusion subgroups were compared, significant differences in BF changes were observed in groups 1 and 3 during the first 20 min of force application (P < 0.05), while in group 2, no statistically significant differences were detected at any time point (Table 4).
Similar BF changes were recorded in teeth subjected to extrusion and intrusion forces using the 3 different AWs. However, in the premolars’ extrusion group, significant BF increase toward baseline values was observed within the first 48 h of force application in the SS AW groups (P = 0.016).
Regression analysis results (Table 5) indicated that BF changes within the first 20 min of force application were significantly associated with tooth type (P = 0.001) and the amount of COS depth change (P < 0.001). However, none of these factors showed any association with BF changes at subsequent time points (P > 0.05).
Secondary outcome
Reduction of COS
Within the 1-month trial, COS was reduced in all groups. The baseline depth of the COS before the intervention averaged 5.30±0.46 mm, 5.60 ± 0.92 mm, and 5.40±0.49 mm in groups 1, 2, and 3, respectively. After 1 month, COS was on average 4.40±0.49 mm, 4.70±0.91, and 4.70±0.46 in groups 1, 2, and 3, respectively (P > 0.05). The reduction of COS was significant in all AW sizes’ groups (P < 0.001).
Discussion
Although BF changes during extrusion and intrusion orthodontic forces have been previously reported [10, 15, 19, 22,23,24,25], these studies were done on individual teeth (incisors or upper molars) with forces applied in a different way to that during conventional fixed orthodontic treatment. Since it has been shown that during orthodontic treatment, COS is leveled by molars and premolars extrusion, and lower incisors intrusion [2,3,4,5], the current study was conducted to investigate and compare BF in the lower teeth during lower arch COS leveling using different AWs. The null hypothesis of this study was partly rejected as there were significant differences in the BF changes between the intrusion and extrusion forces using different AW size and material.
In the current orthodontic practice, 0.017 × 0.025-inch SS, 0.019 × 0.025-inch SS, and 0.21 × 0.025 TMA AWs are used for COS leveling during orthodontic treatment. The reported stiffness values for 0.019 × 0.025-inch SS AW are higher than 0.021 × 0.025-inch-TMA AW which means the amount of the delivered force when using 0.19 × 0.025-inch SS is higher [26]. On the other hand, while TMA AW generates gentle forces and delivers approximately half the force of SS AW [27], 0.021 × 0.025-inch TMA AW has less AW/bracket-slot play (due to increased AW dimension) and has higher frictional resistance compared to SS AWs [28]. The smaller AW/bracket-slot play when 0.021 × 0.025-inch TMA AW is used has the advantage of more torque control and a less lower incisor proclination during leveling. However, the effect of using larger AW dimension with high frictional forces on pulp tissues during orthodontic treatment is not known yet. Furthermore, Wu et al. [20] reported that the use of larger dimension AWs increased the pressure stresses on the PDL and alveolar bone which might add the risk of root resorption and irreversible pulp changes. Therefore, it was assumed that the type and size of the AW might have different impact on the BF during COS leveling with intrusive and extrusive forces.
In the current study, only subjects with good oral hygiene and healthy periodontium were included. The oral health status during the study was maintained by giving the patients oral hygiene instructions both verbally and using social media [29]. Plaque accumulation is a major concern during orthodontic treatment, where brackets, AWs, and elastics hinder access to good oral hygiene measures causing worsening of the oral health status [30]. However, no evidence of any significant difference in oral hygiene levels among the different orthodontic appliances was reported [31].
It has been demonstrated that tooth morphology affects the distribution, the amount of orthodontic force, and the developed strain within the PDL [32]. Therefore, the extrusion force was studied in the first molars and premolars separately.
Different types of tooth movement were reported during leveling the COS in subjects with different vertical proportions. Rozzi et al. [33] demonstrated that in low-angle subjects, leveling of the COS occurs through buccal movement and intrusion of the mandibular incisors; in high-angle subjects, it occurs through extrusion and uprighting of the posterior teeth. In the current study, all included subjects had average or reduced vertical proportions to ensure that arch leveling will be similarly produced among subjects. In the present study, there was a decrease in BF 20 min after the placement of the interventional AWs irrespective of their size, tooth type, or type of force application. The reduction in BF is attributed to the force applied to the vessels that enter and exit the apical foramen, which get constricted. The resulting vascular compression thus creates a reduction in the BF [34]. Extrusion forces cause stretching of the pulpal vasculature, and if severe may result in its rupture, while intrusive forces cause compression and may collapse depending on the magnitude of force. The BF began to recover after 48 h of force application and returned to its baseline levels after 1 week, which indicates that the decaying of the forces had begun, and the inflammatory process of the initial phase was in the reverse.
Within the first 20 min of force application, BF showed more reduction in the extrusion subgroup as compared to the intrusion subgroup. Although intrusion is associated with more crushing of cells and vessels in the apical tissues than luxation injuries, and more detrimental effect on the vasculature of the pulp [18], this effect might have been superseded by higher trauma to the apical vasculature by virtue of larger vertical movements during extrusion. Nasrawi et al. [5] assessed the amount of lower intrusion and molar extrusion during COS leveling using 3 different AWs. They reported that COS was leveled by 0.41 mm, 0.06 mm, and 0.16 mm of lower molar extrusion and by 0.04 mm, 0.24 mm, and 0.58 mm of lower incisor intrusion when 0.017 × 0.025 SS AW, 0.019 × 0.025 SS AW, and 0.021 × 0.025 TMA AW were used, respectively [18].
In the current study, significant BF recovery occurred within 48 h of force application (intrusion and extrusion) in group 1, while it continued to increase in the premolar extrusion subgroups in 0.019 × 0.25-inch SS and 0.21 × 0.025-inch TMA AWs and in the intrusion subgroup in the TMA AW group. The continued BF increase after 1 week of extrusive force application in groups 2 and 3 could be explained by the higher force applied to the teeth using the larger dimension AWs in groups 2 and 3. Also, the less AW/bracket play in group 3 may have produced more frictional forces.
These results agree with previous studies [22, 23, 35] and in partial agreement with Brodin et al. [10], who reported that extrusion of the teeth gave no significant changes in BF, while intrusion reduced the BF by 20% during the first minute after force application, and BF returned to the pre-stimulus level 3 min after unloading. Variation in results may be attributed to the type of tooth being investigated and to the amount of vertical movement induced during either intrusion or extrusion. Contrary to the finding of the current study, Barwick and Ramsay [24] reported that despite the application of heavy intrusive forces for a short time, there was no alteration in the BF in human maxillary central incisors. The small sample size, type of teeth tested, and the size of their apical foramen, force application methods, duration of force application, and the different methodology used to assess BF may explain the variation in results.
These results were also inconsistent with studies that used NiTi AWs; McDonald and Pitt Ford [25] reported an increase in BF at 24 h and 48 h using a removable appliance, while other studies [22, 33, 35, 36] reported a maximum BF reduction 72 h after orthodontic force application and restored BF to original values after 1 month. NiTi AWs are more flexible as they have a lower modulus of elasticity compared to stainless steel wires, with better mechanical properties that allow them to deliver lower continuous force over longer periods. The use of different time points in the current study, different AW sizes and materials, and different force levels in the previous studies explains the difference in the reported findings.
When comparing BF changes between the 3 AWs, only the canines showed significant differences. The canines showed more BF changes (more BF reduction during the first 20 min and more recovery during the first 48 h) when the SS AWs were used. This may be due to higher forces applied to the canines when using the stiffer SS AWs. Also, the position of the canines in the middle of the lower arch connecting the intrusion and extrusion parts of the reverse COS AWS may have subjected the canines to more complex types of orthodontic forces.
When the type of force was compared between the 3 AWs, premolars subgroup showed more BF return toward their baseline value in group 2 (0.019 × 0.025-inch SS AW) as compared to group 3 (TMA AW) within the first 48 h of force application. As the premolars are in the deepest point of the accentuated COS, they are subjected to more extrusive forces when COS is placed in the AW. This indicates that the premolars in SS group may have been subjected to more insults due to higher forces that necessitated an increase in BF changes to help in recovery.
In the current study, 1 month after force application, BF increased beyond its original value. This was contrary to the previous studies [15, 22, 33, 35, 36]. Abu Alhaija et al. [22, 23, 35, 36] reported no difference in the BF 1 month after orthodontic force application and the baseline values using NiTi AW for orthodontic alignment. Also, Sabuncuoglu and Ersahan [15] demonstrated that BF values tend to return to their baseline levels after 3 weeks in both light (40 g) and heavy (120 g) intrusive force groups. However, in their study [15], the intrusive force was applied on upper incisors using NiTi coil spring from 0.016 × 0.022-inch AW to a mini-implant, whereas in the current study, heavier and larger dimensions AWs were used for the COS leveling. The continued increase in BF in the current study even at 1 month may be explained by the fact that forces were higher and more damage has occurred to the pulp; therefore, in an attempt of the pulp to heal itself, hyperemia continued. This is a natural tendency of the pulp tissue to adapt to the aggression caused by force application. The inflammatory process will bring in the inflammatory cells and vasodilation, thus promoting tissue repair and generating new blood vessels [37]. Longer follow-up from 3 or 6 months may have shown more details on the recovery potential of the dental pulp in both types of forces (intrusion, extrusion).
Regression analysis revealed an association between BF changes with the type of tooth and the amount of COS depth changes. The change of the COS reflects the outcome of orthodontic force application. Therefore, it is expected to detect changes in the pulp as a result of this force. Based on the above results, it seems prudent to evaluate the amount of change in COS required and to select the type of AW that may produce the least amount of force to avoid detrimental pulpal effects during extrusion.
Limitations of the current study include the following: BF measurements were carried out during active orthodontic treatment, and teeth were not in a fixed position, the extrusive and intrusive forces were applied to teeth with different morphology, and the presence of the orthodontic appliance limits the measurement area and hinders the placement of a black rubber dam sheet during BF measurements to reduce signals from the gingival blood vessels [38, 39].
Conclusions
-
During CoS leveling, BF was reduced after 20 min and then started to increase at 48 h. It returned to its baseline values 1 week after AW insertion in all AW size groups and type of force subgroups.
-
Similar BF changes were recorded in all teeth using different AWs sizes and materials.
-
In groups 1 and 3, more BF reduction were found in the extruded premolars compared to that of the intruded incisors during the first 20 min of AW placement.
-
After 1 week of reverse CoS AW placement, BF continued to increase in the extruded premolars in groups 2 and 3 and in the intruded incisors in group 3.
-
In the premolars “extrusion subgroup,” BF showed more increase toward baseline values within the first 48 h of force application in the SS AW groups (groups 1 and 2).
-
Tooth type and the amount of COS depth change were associated with BF changes within the first 20 min of force application.
Generalizability
This is a single center study; therefore, generalizability of the results cannot be made.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Carcara S, Preston CB, Jureyda O (2001) The relationship between the curve of Spee, relapse, and the Alexander discipline. In Semin Orthod 7(2):90–99. https://doi.org/10.1053/sodo.2001.23550
Burstone CR (1977) Deep overbite correction by intrusion. Am J Orthod 72(1):1–22. https://doi.org/10.1016/0002-9416(77)90121-x
Parker CD, Nanda RS, Currier GF (1995) Skeletal and dental changes associated with the treatment of deep bite malocclusion. Am J Orthod Dentofacial Orthop 107(4):382–393. https://doi.org/10.1016/s0889-5406(95)70091-9
Bernstein RL, Preston CB, Lampasso J (2007) Leveling the curve of Spee with a continuous archwire technique: a long-term cephalometric study. Am J Orthod Dentofacial Orthop 131(3):363–371. https://doi.org/10.1016/j.ajodo.2005.05.056
Nasrawi YH, Alhaija ESA, Al Maaitah EF (2022) Efficacy of lower arch leveling, lower incisors’ root resorption, and pain associated with the correction of curve of Spee using different orthodontic archwires: a randomized clinical trial. Clin Oral Investig. https://doi.org/10.1007/s00784-022-04672-x
Han G, Hu M, Zhang Y, Jiang H (2013) Pulp vitality and histologic changes in human dental pulp after the application of moderate and severe intrusive orthodontic forces. Am J Orthod Dentofacial Orthop 144:518–522. https://doi.org/10.1016/j.ajodo.2013.05.005
Ramazanzadeh BA, Sahhafian AA, Mohtasham N, Hassanzadeh N, Jahanbin A, Shakeri MT (2009) Histological changes in human dental pulp following application of intrusive and extrusive orthodontic forces. J Oral Sci 51:109–115. https://doi.org/10.2334/josnusd.51.109
Alomari F, Al-Habahbeh R, Alsakarna B (2011) Responses of pulp sensibility tests during orthodontic treatment and retention. Int Endod J 44(7):635–643. https://doi.org/10.1111/j.1365-2591.2011.01865.x
Vongsavan N, Matthews B (1993) Some aspects of the use of laser Doppler flow meters for recording tissue blood flow. Exp Physiol 78:1–14. https://doi.org/10.1113/expphysiol.1993.sp003664
Brodin P, Linge L, Aars H (1996) Instant assessment of blood flow after orthodontic force application. J Orofac Orthop 57:306–309. https://doi.org/10.1007/BF02197551
Hamilton RS, Gutmann JL (1999) Endodontic-orthodontic relationships: a review of integrated treatment planning challenges. Int Endod J 32(5):343–360. https://doi.org/10.1046/j.1365-2591.1999.00252.x
Javed F, Al-Kheraif A, Romanos EA, Romanos GE (2015) Influence of orthodontic forces on human dental pulp: a systematic review. Arch Oral Boil 60:347–356. https://doi.org/10.1016/j.archoralbio.2014.11.011
Polat-Ozsoy O. Pain and discomfort after orthodontic appointments (2007).Semin Orthod 13, 292–300https://doi.org/10.1053/j.sodo.2007.08.010
Subay RK, Kaya H, Tarim B, Subay A, Cox CF (2001) Response of human pulpal tissue to orthodontic extrusive applications. J Endod 27:508–511. https://doi.org/10.1097/00004770-200108000-00003
Sabuncuoglu FA, Ersahan S (2014) Changes in maxillary molar pulp blood flow during orthodontic intrusion. Aust Orthod J 30:152–160
Maltha JC, Van Leeuwen EJ, Dijkman GE, Kuijpers-Jagtman AM (2004) Incidence and severity of root resorption in orthodontically moved premolars in dogs. Orthod Craniofac Res 7:115–121. https://doi.org/10.1111/j.1601-6343.2004.00283.x
Lee KJ, Park YC, Yu HS, Choi SH, Yoo YJ (2004) Effects of continuous and interrupted orthodontic force on interleukin-1beta and prostaglandin E2 production in gingival crevicular fluid. Am J Ortho Dentofacial Orthoped 125:168–177. https://doi.org/10.1016/j.ajodo.2003.03.006
Andreasen J O, Bakland L K, Andreasen F M. (2006) Traumatic intrusion of permanent teeth. Part 2. A clinical study of the effect of preinjury and injury factors, such as sex, age, stage of root development, tooth location, and extent of injury including number of intruded teeth on 140 intruded permanent teeth. Dent Traumatol 22(2):90–8. https://doi.org/10.1111/j.1600-9657.2006.00422.x.
Sabuncuoglu FA, Ersahan S (2015) Comparative evaluation of blood flow during incisor intrusion. Aust Orthod J 31(2):171–177
Wu J, Wang X, Jiang Y, Wu Z, Shen Q, Chen Y, Meng Q, Ye N (2022) Effect of archwire plane and archwire size on anterior teeth movement in sliding mechanics in customized labial orthodontics: a 3D finite element study. BMC Oral Health 22:33. https://doi.org/10.1186/s12903-022-02066-9
Setzer FC, Challagulla P, Kataoka SH, Trope M (2012) Effect of tooth isolation on laser Doppler readings. Int Endo J 45:1–6. https://doi.org/10.1111/iej.12019
Abu Alhaija ES, Taha NA (2021) A comparative study of initial changes in blood flow between conventional and self-ligating fixed orthodontic brackets during leveling and alignment stage. Clin Oral Investig 25(3):971–981. https://doi.org/10.1007/s00784-020-03386-2
Salles AWR, Salles AMC, Nogueira GEC (2013) Laser Doppler blood-flow signals from human teeth during an alignment and leveling movement using a superelastic archwire. ISRN Dent 19;2013:102816. https://doi.org/10.1155/2013/102816. eCollection 2013.
Barwick PJ, Ramsay DS (1996) Effect of brief intrusive force on human blood flow. Am J Orthod Dentofacial Orthop 110(3):273–279. https://doi.org/10.1016/s0889-5406(96)80011-4
Mcdonald F, Pitt Ford TR (1994) Blood flow changes in permanent maxillary canines during retraction. Euro J Orthod 16:1–93. https://doi.org/10.1093/ejo/16.1.1
Sheibaninia A, Salehi A, Asatourian A (2017) Comparison of spring characteristics of titanium-molybdenum alloy and stainless steel. J Clin Exp Dent 9(1):e84. https://doi.org/10.4317/jced.532741
Fischer-Brandies H, Orthuber W, Es-Souni M, Meyer S (2000) Torque transmission between square wire and bracket as a function of measurement, form and hardness parameters. J Orofacial Orthop/Fortschritte der Kieferorthopädie 61(4):258–265. https://doi.org/10.1007/s000560050011
Kusy RP (1997) A review of contemporary archwires: their properties and characteristics. Angle Orthod 67(3):197–207. https://doi.org/10.1043/0003-3219(1997)067<0197:AROCAT>2.3.CO;2
Scribante A, Gallo S, Bertino K, Meles S, Gandini P (2021) Sfondrini MF (2021) The effect of chairside verbal instructions matched with Instagram social media on oral hygiene of young orthodontic patients: a randomized clinical trial. Appl Sci 11(2):706. https://doi.org/10.3390/app11020706
Al-Jewair TS, Suri S, Tompson BD (2011) Predictors of adolescent compliance with oral hygiene instructions during two arch multibracket fixed orthodontic treatment. Angle Orthod 81:525–531
Chhibber A, Agarwal S, Yadav S, Kuo CL, Upadhyay M (2018) Which orthodontic appliance is best for oral hygiene? A randomized clinical trial. Am J Orthod Dentofacial Orthop 153(2):175–183. https://doi.org/10.1016/j.ajodo.2017.10.009
Papageorgiou SN, Sifakakis I, Keilig L, Patcas R, Affolter S, Eliades T, Bourauel C (2016) Torque differences according to tooth morphology and bracket placement: a finite element study. Eur J Orthod 39(4):411–418. https://doi.org/10.1093/ejo/cjw074
Rozzi M, Mucedero M, Pezzuto C, Cozza P (2017) Leveling the curve of Spee with continuous archwire appliances in different vertical skeletal patterns: a retrospective study. Am J Ortho Dentofacial Orthop 151:758–766. https://doi.org/10.1016/j.ajodo.2016.09.023
Heyeraas KJ, Kvinnsland I (1992) Tissue pressure and blood flow in pulpal inflammation. Proc Finn Dent Soc 88:393–401
Abu Alhaija ESJ, Al-Abdallah SY, Taha NA (2019) A comparative study of initial changes in blood flow between clear aligners and fixed orthodontic appliances. Am J Orthod Dentofacial Orthop 156(5):603–610. https://doi.org/10.1016/j.ajodo.2018.11.013
Alhaija ESA, Shahin AY, Badran SA, Daher SO, Daher HO (2021) Blood flow changes and pain scores related to using superelastic 0.018-inch nickel titanium as the first orthodontic alignment archwire: a prospective clinical trial. J Appl Oral Sci 4;29:e20210089. https://doi.org/10.1590/1678-7757-2021-0089. .
Vandevska-Radunovic V, Kristiansen AB, Heyeraas KJ, Kvinnsland S (1994) Changes in blood circulation in teeth and supporting tissues incident to experimental tooth movement. Eur J Orthod 16:361–369. https://doi.org/10.1093/ejo/16.5.361
Hartmann A, Azérad J, Boucher Y (1996) Environmental effects on laser Doppler pulpal blood-flow measurements in man. Arch Oral Biol 41:333–339. https://doi.org/10.1016/0003-9969(95)00133-6
Soo-ampon S, Vongsavan N, Soo-ampon M, Chuckpaiwong S, Matthews B (2003) The sources of laser Doppler blood-flow signals recorded from human teeth. Arch Oral Biol 48(5):353–360. https://doi.org/10.1016/s0003-9969(03)00011-6
Funding
Open Access funding provided by the Qatar National Library. The study was supported by the Deanship of Research at the Jordan University of Science and Technology, research grant number (436/2018).
Author information
Authors and Affiliations
Contributions
Conceptualization: Elham S. Abu Alhaija. Methodology: Elham S. Abu Alhaija, Nessrin Taha, Hasan Daher, Saba Daher, Yousef H. Nasrawi. Data acquisition: All authors. Formal analysis and investigation: Raidan Ba-Hattab. Interpretation: Raidan Ba-Hattab. Writing—original draft preparation: Elham S. Abu Alhaija, Nessrin Taha, Raidan Ba-Hattab. Writing—review and editing: All authors. Funding acquisition: Elham S. Abu Alhaija. Correspondence: Raidan Ba-Hattab.
Corresponding author
Ethics declarations
Ethics approval
The study was approved by the institutional ethics and research committee at the Jordan University of Science and Technology, and it is registered with clinicaltrials.gov registration number NCT04549948.
Informed consent
A written informed consent was obtained from all participants before the treatment.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ba-Hattab, R., Abu Alhaija, E.S., Nasrawi, Y.H. et al. Leveling the curve of Spee using different sized archwires: a randomized clinical trial of blood flow changes. Clin Oral Invest 27, 2943–2955 (2023). https://doi.org/10.1007/s00784-023-04894-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-023-04894-7