
Abstract
Objectives
Mandibular reconstruction after segmental mandibulectomy can be challenging without virtual surgical planning and osteotomy guides. The purpose of this study was to analyze anatomic parameters to facilitate the evaluation of ideal fibula wedge osteotomies to reconstruct the neomandibula in a simple and cost-effective manner without the need for preoperative virtual planning.
Materials and methods
Computed tomography scans were acquired from randomly selected patients, and all images were obtained from routine clinical diagnostics, e.g., tumor staging, or preoperatively before reconstruction. Data was used to calculate stereolithographic models of the mandible for length and angle measurements. Statistical analysis was performed (p < 0.05).
Results
CT scans of 100 patients were analyzed: 39 were female and 61 were male patients, mean age was 59.08a. The mandibular arch angle proved to be constant with 241.07 ± 2.39°. The outside B-segment length was 80.05 ± 5.16 mm; the anterior S-segment length was 27.69 ± 3.16 mm. The angle of the mandibular arch showed differences in means (p = 0.004) between age groups, but effect was proved low. No relevant statistical significances were detected.
Conclusions
The development of a mandible reconstruction template tool would benefit the majority of head and neck patients, which is due to a constant mandibular arch angle and symphysis segment length throughout the general patient population, allowing the mimicking of a harmonic mandibular arch with up to three fibula segments.
Clinical relevance
The developed mandible reconstruction template tool can facilitate the fibula wedge osteotomies necessary for reconstruction of an ideal neomandibula providing a novel approach which is simple and cost-effective.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The bony reconstruction of the mandible by microvascular fibula free flaps after segmental mandibulectomy is an established standard procedure in reconstructive head and neck surgery. As first described in the maxillofacial region by Hidalgo et al. in 1989 [1], it was proved to be well suited for mandible reconstruction due to a long vascular pedicle, a wide vessel diameter, and the possibility to harvest a skin island and a muscle cuff. Further, a shortened operating time by a two-team approach for the vessel and transplant dissection is less physically demanding for the patient and the surgeon [2, 3]. Additionally, the fibula is the only bone transplant which allows reconstruction of the whole mandible with one single flap. Nevertheless, surgeons are challenged by reconstructions of complex defects with one or more osteotomies in order to achieve a harmonic and functional neomandibular arch [4]. At the same time, the mandible plays an essential role for facial harmony, speech, mastication, and airway maintenance [5]. To address these vital roles of the mandible and to mimic it in the most accurate way possible, the exact adaption, segmentation, and forming of the fibula are essential. Therefore, the simulation of the mandibular contour correspondingly assumes the exact angles of the osteotomy and the bent plates. A feasible solution is seen in virtual surgical planning (VSP). VSP is increasingly applied for complex defect reconstructions, especially in two or more segmented mandible reconstruction cases to facilitate osteotomy and enhance accuracy. As a drawback, VSP is associated with higher financial costs and more intense preoperative planning. Furthermore, VSP has the drawback of a limited intraoperative flexibility. This could lead to have some safety risk, e.g., the resection margins are much larger than planned before and whole VSP therefore fails. In less complex reconstructive cases, the question remains if full-scale VSP with high additional preoperative effort and costs improves patient outcome. Efforts were made to address small defects by using stereolithographic (STL) models, silicon templates, and handmade cutting guides [6]. However, few tools to support osteotomy placement and segment design are available for microvascular fibular transplant reconstruction in head and neck surgery. During clinical routine, the experienced reconstructive surgeon is frequently confronted with more segmental bone defects, where full-scale VSP might be considered too laborious, but non-guided fibula reconstruction is challenging due to the correct osteotomy arches and the risk of impairing the pedicle and/or the skin perforators during transplant fitting and osteosynthesis. Consequently, the need for alternative methods without time-consuming preoperative planning and thus reduced financial overheads is evident. The aim of the study was the development of a surgical resection and reconstruction guide in order to facilitate fibula free flap reconstruction of the mandible. This consists of a template with an arbitrary symphysis segment and length-adjustable corpus segments. For the development and planning of the resection and reconstruction guide, detailed anatomic knowledge on the possible variations of angles and distances of the B- and S-segments of the human mandible was needed to cover the extensive variety of defect configurations. We therefore implemented a study on analyzing anatomic parameters of the human mandible with special focus on the variations in length of the B- and S-segments, as well as on the angles of the mandibular arch. Sufficient data on the anatomic values necessary for constructing an effective mandibular reconstruction tool do not exist in the international literature. Hence, we evaluated existing CT scans for routine diagnostics of patients, generated corresponding digital 3D models, and performed exact measurements of clinically relevant values.
Materials and methods
Study design and data acquisition
To address the raised questions regarding the distribution of anatomic proportions of the human mandible for the development of a resection and reconstruction device for fibula free flaps, a retrospective cohort study was designed and implemented. The collection and analysis of the study’s data was approved by the ethics committee of the Technische Universität München (registration number 459/18S). The research was conducted in accordance with the Declaration of Helsinki.
Study sample
The study included digital radiological data of high-resolution computed tomography (CT) scans from 100 randomly selected patients. All patients under the age of 16 years and with traumatic or pretreated mandibular defects as well as bony reconstructions were excluded. Patients with deformities of the mandibular, e.g., due to syndromic diseases or patients with dysgnathia were also excluded from the patient collective. The Digital Imaging and Communications in Medicine (DICOM) data was used for the calculation of 3D models for corresponding anatomic measurements. All patients eligible for the study were treated at the Department of Oral and Maxillofacial Surgery of the Klinikum rechts der Isar, Technische Universität München, and evaluated retrospectively. Radiological data of relevant cases was archived after treatment for further anatomic evaluation and digital 3D model preparation. CT scans were obtained as DICOM data files, and slice thickness had to be smaller than 1 mm for sufficient STL model resolution.
3D model preparation
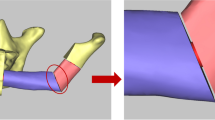
The acquired DICOM data of relevant CT scans was matched with corresponding clinical patient data (e.g., age, sex, dental status), and measurement values were collected. DICOM data was imported into the Mimics software (Mimics Innovation Suite 19.0, Materialise, Leuven, Belgium). Radiological images were evaluated, and 3D models were calculated by using the software. Virtual tissue dissection was performed on the data set until only the bony mandible components remained. The model was then exported as an STL file for further processing and analysis (Fig. 1).

Illustration of the novel resection and cutting guide for mandibular reconstruction by free fibula flaps. The construction design of the two templates (above) and their clinical use (below)
Anatomic measurement
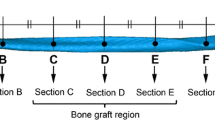
The calculated STL files were imported into the netfabb software (netfabb Basic, version 5.2.1, Autodesk Inc., San Rafael, USA). The STL models were marked with defined points for distance and angle measurements. Resulting values were collected and used for further statistical analysis. The angle of the whole mandibular arch was measured on the caudal border of the mandible and consists of the left and right angles between the B- and S-segments (see Fig. 2). The length of the S- and B-segments on the lateral, medial, and caudal surface of the mandible were measured from the canine to the jaw angle in a parallel line to the base of the mandible (see Fig. 3). Condylar distances were measured between the mid- and most cranial surface point of the condyle (Co) on each side. Additionally, the distance from the condyle’s surface to the gnathion (Gn), as the most caudal point of the mandible symphysis in the median-sagittal plane, was measured [7] (see Fig. 4).

The measurement of the mandibular arch angles

The measurement of the B- and S-segments

Additional anatomic measurements
Data analysis and statistical calculations
The obtained clinical patient data was correlated with measurement values from the 3D models. Statistical analysis on base data was performed for patient demographics and corresponding measurement value distribution. The SPSS 22.0.0 software (IBM SPSS, Inc., Chicago, IL, 2013) was used for statistical calculations. The Pearson correlations and t tests for independent samples were performed to evaluate associations between clinical variables (e.g., age, sex, dental status) and values of anatomic measurements. A p value < 0.05 was considered to be statistically significant.
Results
Altogether, the study reviewed and analyzed the radiological and clinical data of 100 patients with a normal state mandibula. All patients had recent CT scans, which were performed during routine diagnostics. DICOM data of relevant patients was acquired, and 3D models of the mandible were produced digitally. Out of the 100 included patients, 39 were female and 61 were male. The mean age of the patients was 59.08 years (median 60.5 years; SD 15.741; range 77 years; min–max 16–93 years). With regard to dental status, 20 patients (20%) were edentulous, 26 patients (26%) were partially edentulous (1–6 remaining teeth), and 54 patients (54%) were toothed (> 6 teeth) (see Table 1). The values of the various measurements of the mandible in detail are displayed in Table 2; the corresponding distances are illustrated in Fig. 4. The angle of the mandibular arch was proved highly constant in the measurement results. The overall value was 241.07° (SD ± 2.39°, range 16.68°, min 235.40°, max 252.08°); values for the left side were 120.39° ± 1.68° and for the right side 120.68° ± 1.44°. The outside length of the B-segment was measured to be 80.05 mm (SD ± 5.16 mm, range 27.40 mm, min 68.81 mm, max 96.21 mm) and the length of the anterior S-segment was 27.69 mm (SD ± 3.16 mm, range 16.33 mm, min 20.62 mm, max 36.95 mm). The distance from the surface of the condyle (Co) to the anterior chin (Gn) was 124.83 mm (SD ± 6.84 mm, range 40.90 mm), between the two condyles (Co–Co) the length was 104.95 mm (SD ± 5.20 mm, range 30.21 mm), and between the two jaw angles the length was 98.89 mm (SD ± 7.20 mm, range 33.88 mm). The distance between the canine teeth could be measured in 75 patients and was 26.21 mm (SD ± 2.07 mm, range 11.76).
The mandibular arch angle showed a positive correlation with age (p = 0.002) and a negative correlation with the parameters depicting the sagittal mandibular length, e.g., lateral B-segment (p = 0.009), caudal B-segment (p = 0.012), medial B-segment (p = 0.009), caudal S-segment (p = 0.003), jaw angle–Gn (p = 0.002), and Co–Gn (p = 0.008).
The angle of the mandibular arch showed differences in means (p = .004) between age groups (threshold 50 years), but the effect was proved low (Cohen r = .12). Other relevant statistical significances could not be detected. Referring to this data, we started the development of a surgical resection and reconstruction guide which consists of a template with an arbitrary symphysis segment and length-adjustable corpus segments.
The construction plan contained a cutting guide for the mandible as well as the fibula, both having a sliding bar for individual adjustment of the segment length for the corpus. Resection was performed after placement of the resection template on the lower jaw for one, two, or three segments, e.g., B, SB, or BSB, according to the classification by Urken [8]. The extension of the B-segments could be measured, and the adjusted length was transferred to the fibula template, where concordant osteotomies were performed. Afterward, the exact positioning of the segments and corresponding osteosynthesis was supported by the template (Fig. 1). The development was performed in collaboration with an industrial partner (KLS Martin, Tuttlingen, Germany).
Discussion
Microvascular fibula free flap is regarded as standard treatment for reconstruction of the mandible. The key to mimicking the human jaw in the most natural way possible is to perform the ideal fibula osteotomies and follow osteosynthesis of the segments in order to achieve a harmonic mandibular arch. VSP is increasingly applied especially in two or more segmented mandible reconstruction cases to facilitate osteotomies and thus enhance accuracy. Several authors describe advantages of this method regarding reduced operating time and increased precision of reconstruction with comparable complication rates [2, 4, 9,10,11,12,13,14,15,16,17]. Critical points are the additional costs and time for preoperative planning and that the strategy is superfluous in the case of positive margins or other reasons for intraoperative treatment concept modification [18,19,20]. While changing, the surgical strategy is getting easier with increasing experience in this technique; costs are a serious matter against the background of cost-effectiveness as well as clinical outcomes as a benchmark for hospitals and insurance carriers [21]. As an alternative to VSP-planned cutting guides, Pirgousis et al. reported the ideal fibula wedge osteotomy to recreate the mandibular angle by using an autoclavable metal wedge of about 56° [5]. Their team measured the angle of the mandibular angle in 60 patients and produced a wedge respecting the average angle of all measured patients. This simple but well-designed technique is very well suited for reconstructions of defects of the body and ascending ramus, e.g., BR according to the classification of Urken [8]. However, many mandible reconstructions, especially after tumor ablation due to oral squamous cell carcinoma infiltration in the anterior part of the mandible, require reconstruction of the body and symphysis region (BS or BSB). As no technique to facilitate the reconstruction of this angle has been described at present, the aim of this study was to analyze the angle of different patients to find a standard angle for the symphysis body region.
We therefore implemented a study based on radiological data from high-resolution CT scans, which were performed on patients during routine oral and maxillofacial diagnostics. DICOM data from the scans were then used for digital 3D-model generation, and anatomic measurements were performed. These examinations revealed harmonic statistic results (see Table 2). The angle of the mandibular arch is highly constant with 241.07° ± 2.39° and not mainly influenced by age and sex. Therefore, it is possible to achieve a harmonic and natural neomandibular arch with a three-segmented fibula and fixation angles between the two BS segments of 120° on each side. Furthermore, the S-segment also proved to be relatively constant and independent from other parameters with 27.69 mm ± 3.16 mm. The B-segment was however the parameter with more distributed values of 80.05 mm ± 5.16 mm (range 27.40 mm). Hence, it was possible to construct a single template device for all patients independent of gender or age. The length of the symphysis (S-segment) and the angles between corpus and symphysis (BS angle) could be standardized, due to their constant length. The length of the corpus (B-segment) however has to allow an individually adjustable length. With the length of the symphysis segment being fixed to about 27 mm and not designed to be adjustable, it was important that this length does not lead to malperfusion. The selected length for the anterior segment was estimated to be a safe segment length with regard to bone perfusion, as similar values have been used by the authors previously and throughout the literature without leading to complications [22,23,24]. Based on this data, the planned fibula free flap reconstruction templates could now be designed and constructed [25].
The developed fibula reconstruction tool can be both used on the patients’ left and right fibulas without difference. It is designed for the standard case of harvesting the right fibula with anastomosis on the left neck side and intraoral skin paddle position or harvesting the left fibula with anastomosis on the right neck side and intraoral skin paddle position. The template tool can also be used in non-standard cases. For these situations, the outer osteotomy guides have to be exchanged with each other. This adaption is used for harvesting the right fibula with anastomosis on the right neck side and extraoral/small skin paddle or harvesting the left fibula with anastomosis on the left neck side with extraoral/small skin paddle. The anatomic data generated in this study with special focus on the relevance for head and neck reconstructive surgery is unique in the international literature. Several studies have been published on the subject of anatomic mandible data, but most of these are unsuitable for questions on bony reconstruction. Watanabe et al., for example, measured height and width of human mandibles and the path of the canal of the inferior alveolar nerve with respect to implantological questions, without referring to mandibular angles and segment length [26]. Miller et al. also analyzed the mandible with regard to implantological issues, especially focusing on the symphysis region [27]. Deguchi et al. analyzed the volumes of the maxilla and the mandible as well as their respective ratio with regard to dysgnathia patients [28]. However, the study did not provide values useful for the development of a fibula reconstruction template tool. A study performed by Kano et al. on postmortem CT scans of Japanese subjects with the aim of facilitating gender determination by analyzing anatomic angles and landmarks of the mandible featured some of the values also represented in our data [29]. In this study, special focus was given to the mental region, as chin differences between genders are most distinct. Due to the different placement of the measurement points, a general comparison to our data evaluation is not possible even though some of the measured values are overlapping. At least for the distance between the jaw angles, the selected points of measurement are comparably equal and the related values are very similar (e.g., means in length from Kano et al. are 102.9 mm for male/95.8 mm for female patients, compared with 101.8 mm for male/94.4 mm for female subjects in this study). However, this data does not provide the relevant information to reconstruct a standardized neomandible. Consequently, to this day, there is no anatomic data published in the international literature displaying the necessary values for the development of a template tool for mandible reconstruction with fibula free flap, thus highlighting the importance of this study.
Conclusion
It can be concluded that the development of a standardized template tool for mandible reconstruction with fibula free flap is possible, due to a constant mandibular arch angle of about 240° and a symphysis segment length of 27.69 mm throughout the general patient population. The corpus length, by contrast, is the only part which needs to be adaptable to different mandibular extensions. The design and development of a standardized reconstruction device have already started, and the clinical testing and implementation process are ongoing. The expected release and thus common availability of the template system is scheduled for the second half of 2019.
References
Hidalgo DA (1989) Fibula free flap: a new method of mandible reconstruction. Plast Reconstr Surg 84(1):71–79
Roser SM, Ramachandra S, Blair H, Grist W, Carlson GW, Christensen AM, Weimer KA, Steed MB (2010) The accuracy of virtual surgical planning in free fibula mandibular reconstruction: comparison of planned and final results. J Oral Maxillofac Surg 68(11):2824–2832. https://doi.org/10.1016/j.joms.2010.06.177
Thankappan K, Trivedi NP, Subash P, Pullara SK, Peter S, Kuriakose MA, Iyer S (2008) Three-dimensional computed tomography-based contouring of a free fibula bone graft for mandibular reconstruction. J Oral Maxillofac Surg 66(10):2185–2192. https://doi.org/10.1016/j.joms.2008.01.035
Antony AK, Chen WF, Kolokythas A, Weimer KA, Cohen MN (2011) Use of virtual surgery and stereolithography-guided osteotomy for mandibular reconstruction with the free fibula. Plast Reconstr Surg 128(5):1080–1084. https://doi.org/10.1097/PRS.0b013e31822b6723
Pirgousis P, Brown D, Fernandes R (2013) Digital measurements of 120 mandibular angles to determine the ideal fibula wedge osteotomy to re-create the mandibular angle for microvascular reconstruction. J Oral Maxillofac Surg 71(12):2169–2175. https://doi.org/10.1016/j.joms.2013.05.005
Rommel N, Kesting MR, Rohleder NH, Bauer FMJ, Wolff KD, Weitz J (2017) Mandible reconstruction with free fibula flaps: outcome of a cost-effective individual planning concept compared with virtual surgical planning. J Craniomaxillofac Surg 45(8):1246–1250. https://doi.org/10.1016/j.jcms.2017.04.010
Segner D, Hasund A (1994) Individualisierte Kephalometrie, vol 2. Franklin Printing and Publishing House Ltd, Hamburg
Urken ML, Weinberg H, Vickery C, Buchbinder D, Lawson W, Biller HF (1991) Oromandibular reconstruction using microvascular composite free flaps. Report of 71 cases and a new classification scheme for bony, soft-tissue, and neurologic defects. Arch Otolaryngol Head Neck Surg 117(7):733–744
Gil RS, Roig AM, Obispo CA, Morla A, Pages CM, Perez JL (2015) Surgical planning and microvascular reconstruction of the mandible with a fibular flap using computer-aided design, rapid prototype modelling, and precontoured titanium reconstruction plates: a prospective study. Br J Oral Maxillofac Surg 53(1):49–53. https://doi.org/10.1016/j.bjoms.2014.09.015
Avraham T, Franco P, Brecht LE, Ceradini DJ, Saadeh PB, Hirsch DL, Levine JP (2014) Functional outcomes of virtually planned free fibula flap reconstruction of the mandible. Plast Reconstr Surg 134(4):628e–634e. https://doi.org/10.1097/PRS.0000000000000513
Foley BD, Thayer WP, Honeybrook A, McKenna S, Press S (2013) Mandibular reconstruction using computer-aided design and computer-aided manufacturing: an analysis of surgical results. J Oral Maxillofac Surg 71(2):e111–e119. https://doi.org/10.1016/j.joms.2012.08.022
Metzler P, Geiger EJ, Alcon A, Ma X, Steinbacher DM (2014) Three-dimensional virtual surgery accuracy for free fibula mandibular reconstruction: planned versus actual results. J Oral Maxillofac Surg 72(12):2601–2612. https://doi.org/10.1016/j.joms.2014.07.024
Sharaf B, Levine JP, Hirsch DL, Bastidas JA, Schiff BA, Garfein ES (2010) Importance of computer-aided design and manufacturing technology in the multidisciplinary approach to head and neck reconstruction. J Craniofac Surg 21(4):1277–1280. https://doi.org/10.1097/SCS.0b013e3181e1b5d8
Tepper O, Hirsch D, Levine J, Garfein E (2012) The new age of three-dimensional virtual surgical planning in reconstructive plastic surgery. Plast Reconstr Surg 130(1):192e–194e; author reply 194e-195e. https://doi.org/10.1097/PRS.0b013e318254fbf6
Zheng GS, Su YX, Liao GQ, Chen ZF, Wang L, Jiao PF, Liu HC, Zhong YQ, Zhang TH, Liang YJ (2012) Mandible reconstruction assisted by preoperative virtual surgical simulation. Oral Surg Oral Med Oral Pathol Oral Radiol 113(5):604–611. https://doi.org/10.1016/j.tripleo.2011.05.016
Stirling Craig E, Yuhasz M, Shah A, Blumberg J, Salomon J, Lowlicht R, Fusi S, Steinbacher DM (2015) Simulated surgery and cutting guides enhance spatial positioning in free fibular mandibular reconstruction. Microsurgery 35(1):29–33. https://doi.org/10.1002/micr.22229
Mazzoni S, Marchetti C, Sgarzani R, Cipriani R, Scotti R, Ciocca L (2013) Prosthetically guided maxillofacial surgery: evaluation of the accuracy of a surgical guide and custom-made bone plate in oncology patients after mandibular reconstruction. Plast Reconstr Surg 131(6):1376–1385. https://doi.org/10.1097/PRS.0b013e31828bd6b0
Moro A, Cannas R, Boniello R, Gasparini G, Pelo S (2009) Techniques on modeling the vascularized free fibula flap in mandibular reconstruction. J Craniofac Surg 20(5):1571–1573. https://doi.org/10.1097/SCS.0b013e3181b0db5c
Deek NF, Wei FC (2016) Computer-assisted surgery for segmental mandibular reconstruction with the osteoseptocutaneous fibula flap: can we instigate ideological and technological reforms? Plast Reconstr Surg 137(3):963–970. https://doi.org/10.1097/01.prs.0000479998.49928.71
Weitz J, Bauer FJ, Hapfelmeier A, Rohleder NH, Wolff KD, Kesting MR (2016) Accuracy of mandibular reconstruction by three-dimensional guided vascularised fibular free flap after segmental mandibulectomy. Br J Oral Maxillofac Surg 54(5):506–510. https://doi.org/10.1016/j.bjoms.2016.01.029
Toto JM, Chang EI, Agag R, Devarajan K, Patel SA, Topham NS (2014) Improved operative efficiency of free fibula flap mandible reconstruction with patient-specific, computer-guided preoperative planning. Head Neck. https://doi.org/10.1002/hed.23815
Fichter AM, Ritschl LM, Georg R, Kolk A, Kesting MR, Wolff KD, Mucke T (2019) Effect of segment length and number of osteotomy sites on cancellous bone perfusion in free fibula flaps. J Reconstr Microsurg 35(2):108–116. https://doi.org/10.1055/s-0038-1667364
Matros E, Santamaria E, Cordeiro PG (2013) Standardized templates for shaping the fibula free flap in mandible reconstruction. J Reconstr Microsurg 29(9):619–622. https://doi.org/10.1055/s-0033-1356645
Strackee SD, Kroon FH, Jaspers JE, Bos KE (2001) Modeling a fibula transplant in mandibular reconstructions: evaluation of the effects of a minimal number of osteotomies on the contour of the jaw. Plast Reconstr Surg 108(7):1915–1921; discussion 1922-1913. https://doi.org/10.1097/00006534-200112000-00010
Weitz J, Wolff KD, Kesting MR, Nobis CP (2018) Development of a novel resection and cutting guide for mandibular reconstruction using free fibula flap. J Craniomaxillofac Surg. https://doi.org/10.1016/j.jcms.2018.09.007
Watanabe H, Mohammad Abdul M, Kurabayashi T, Aoki H (2010) Mandible size and morphology determined with CT on a premise of dental implant operation. Surg Radiol Anat 32(4):343–349. https://doi.org/10.1007/s00276-009-0570-3
Miller RJ, Edwards WC, Boudet C, Cohen JH (2011) Maxillofacial anatomy: the mandibular symphysis. J Oral Implantol 37(6):745–753. https://doi.org/10.1563/AAID-JOI-D-10-00136
Deguchi T Sr, Katashiba S, Inami T, Foong KW, Huak CY (2010) Morphologic quantification of the maxilla and the mandible with cone-beam computed tomography. Am J Orthod Dentofac Orthop 137(2):218–222. https://doi.org/10.1016/j.ajodo.2008.02.029
Kano T, Oritani S, Michiue T, Ishikawa T, Hishmat AM, Sogawa N, Inamori-Kawamoto O, Maeda H (2015) Postmortem CT morphometry with a proposal of novel parameters for sex discrimination of the mandible using Japanese adult data. Legal Med 17(3):167–171. https://doi.org/10.1016/j.legalmed.2014.12.009
Acknowledgments
The present work was performed in (partial) fulfillment of the requirements for obtaining the degree “Dr. med. dent.”
Funding
Open Access funding provided by Projekt DEAL. Presented data acquisition, analyzation, and development of the fibula reconstruction templates were financially supported by Gebrüder Martin GmbH & Co. KG, KLS Martin Group, Tuttlingen, Germany. Funding was received by the Department of Oral and Maxillofacial Surgery, Klinikum Rechts der Isar, Technische Universität München (Head: Prof. Dr. Dr. K.-D. Wolff).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The fibula reconstruction templates were jointly developed with Gebrüder Martin GmbH & Co. KG, KLS Martin Group, Tuttlingen, Germany. The Department of Oral and Maxillofacial Surgery, Klinikum Rechts der Isar, Technische Universität München received financial funding for the development. The authors declare to have no further conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (Technische Universität München, registration number 459/18S) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain studies with animals performed by any of the authors.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nobis, CP., Kesting, M.R., Wolff, KD. et al. Development of a template tool for facilitating fibula osteotomy in reconstruction of mandibular defects by digital analysis of the human mandible. Clin Oral Invest 24, 3077–3083 (2020). https://doi.org/10.1007/s00784-019-03177-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-019-03177-4