
Abstract
Background
The radiolucent zones in the patella are sometimes observed in patients who have undergone total knee arthroplasty (TKA) without patellar resurfacing. On the basis of radiological findings from our clinical experience, we hypothesize that the pathogenesis of this lesion may be similar to that of the lesions of spontaneous osteonecrosis, and this lesion may be due to both osteoporosis and stress concentration. The present study aimed to determine the incidence of the radiolucent zone after TKA without patellar resurfacing. Moreover, the roles of osteoporosis and patellar morphology, which are related to the stress distribution in the patella, were also investigated.
Methods
We studied 48 knees of 38 patients who underwent primary TKA using the Genesis II prosthesis. Axial radiographs taken 1 year postoperatively were used to assess the incidence of the radiolucent zone. The World Health Organization fracture risk assessment tool (FRAX) score and the preoperative patellar facet angle were compared between patients with and without the radiolucent zones.
Results
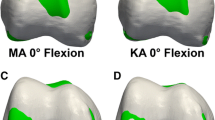
Five patellae (10.4 %) showed the radiolucent zones postoperatively (the radiolucent group), whereas no such lesions were found in the remaining 43 patellae (the normal group). The major osteoporotic fracture risk of the radiolucent group calculated using the FRAX was 24.8 % and significantly higher than that in the normal group (14.7 %; p = 0.01). The average patellar facet angle in the radiolucent group was 123.6°, which was significantly smaller than that in the normal group (133.6°; p = 0.003).
Discussion and conclusions
The results of the present study suggest that both underlying osteoporosis and a steep patellar facet angle may play an important role in the pathogenesis of the radiolucent zones in patellae after TKA without patellar resurfacing. Patellar resurfacing may be considered, particularly in osteoporotic patients who have a steep patellar facet angle, to avoid the appearance of the postoperative radiolucent zone in the patella.




Similar content being viewed by others


References
Hasegawa M, Ohashi T. Long-term clinical results and radiographic changes in the nonresurfaced patella after total knee arthroplasty: 78 knees followed for mean 12 years. Acta Orthop Scand. 2002;73:539–45.
Rodriguez-Merchan EC, Gomez-Cardero P. The outerbridge classification predicts the need for patellar resurfacing in TKA. Clin Orthop Relat Res. 2009;468:1254–7.
Shih HN, Shih LY, Wong YC, Hsu RW. Long-term changes of the nonresurfaced patella after total knee arthroplasty. J Bone Joint Surg Am. 2004;86-A:935–9.
Narvaez JA, Narváez J, De Lama E, Sánchez A. Spontaneous osteonecrosis of the knee associated with tibial plateau and femoral condyle insufficiency stress fracture. Eur Radiol. 2003;13:1843–8.
Robertson DD, Armfield DR, Towers JD, Irrgang JJ, Maloney WJ, Harner CD. Meniscal root injury and spontaneous osteonecrosis of the knee: an observation. J Bone Joint Surg Br. 2009;91:190–5.
Yamamoto T, Bullough PG. Spontaneous osteonecrosis of the knee: the result of subchondral insufficiency fracture. J Bone Joint Surg Am. 2000;82:858–66.
Fujiwara S, Nakamura T, Orimo H, Hosoi T, Gorai I, Oden A, Johansson H, Kanis JA. Development and application of a Japanese model of the WHO fracture risk assessment tool (FRAX). Osteoporos Int. 2008;19:429–35.
Watts NB, Lewiecki EM, Miller PD, Baim S. National Osteoporosis Foundation 2008 Clinician’s Guide to Prevention and Treatment of Osteoporosis and the World Health Organization Fracture Risk Assessment Tool (FRAX): what they mean to the bone densitometrist and bone technologist. J Clin Densitom. 2008;11:473–7.
Takahashi A, Sano H, Ohnuma M, Kashiwaba M, Chiba D, Kamimura M, Sugita T, Itoi E. Patellar morphology and femoral component geometry influence patellofemoral contact stress in total knee arthroplasty without patellar resurfacing. Knee Surg Sports Traumatol Arthrosc. 2012;20:1787–95.
Kanamiya T, Naito M, Hara M, Yoshimura I. The influences of biomechanical factors on cartilage regeneration after high tibial osteotomy for knees with medial compartment osteoarthritis: clinical and arthroscopic observations. Arthroscopy. 2002;18:725–9.
Wiberg G. Roentgenographs and anatomic studies on the femoropatellar joint: with special reference to chondromalacia patellae. Acta Orthop Scand. 1941;12:319–410.
Insall J, Salvati E. Patella position in the normal knee joint. Radiology. 1971;101:101–4.
Heesterbeek PJ, Beumers MP, Jacobs WC, Havinga ME, Wymenga AB. A comparison of reproducibility of measurement techniques for patella position on axial radiographs after total knee arthroplasty. Knee. 2007;14:411–6.
Waters TS, Bentley G. Patellar resurfacing in total knee arthroplasty. A prospective, randomized study. J Bone Joint Surg Am. 2003;85:212–7.
van Jonbergen HP, Scholtes VA, van Kampen A, Poolman RW. A randomised, controlled trial of circumpatellar electrocautery in total knee replacement without patellar resurfacing. J Bone Joint Surg Br. 2011;93:1054–9.
Noble J, Alexander K. Studies of tibial subchondral bone density and its significance. J Bone Joint Surg Am. 1985;67:295–302.
Durr HD, Martin H, Pellengahr C, Schlemmer M, Maier M, Jansson V. The cause of subchondral bone cysts in osteoarthrosis: a finite element analysis. Acta Orthop Scand. 2004;75:554–8.
Conflict of interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subjects of this study.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Takahashi, A., Kamimura, M., Sano, H. et al. Radiolucent zone of the patella following total knee arthroplasty without patellar resurfacing. J Orthop Sci 19, 558–563 (2014). https://doi.org/10.1007/s00776-014-0570-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00776-014-0570-y