
Summary
Background
The aim of our study was to investigate the role of visual load levels in intraocular pressure (IOP) elevation in patients taking prostaglandin analogs and to try to optimize the conditions for their effects on the uveoscleral outflow.
Material and methods
A total of 33 patients (40 eyes) with first diagnosed primary open-angle glaucoma (POAG) and resistance to latanoprost 0.005 % IOP were included in this study. These patients were pre-examined with the definition of visual and reading acuity, refraction, and true, tolerant, and target IOP with perimetry and ophthalmoscopy. Subjects were divided into two groups of comparable age, sex, and refraction. In each group, the thickness of the ciliary body by ultrasound biomicroscopy was investigated, and the level of near visual load and tolerated correction for near were defined.
Results
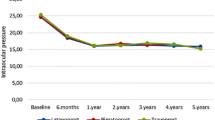
It was found that in both groups, 85 % of the eyes with POAG had moderately high (3–6 h per day) and high (> 6 h per day) near visual load. Maximal ciliary body thickness in both groups was significantly higher than the results received by other authors: 0.881 ± 0.039 mm in group 1 and 0.889 ± 0.049 mm in group 2. Also, a direct dependence of the ciliary body thickness on the true value of IOP (r = 0.52) was observed. Hypercorrection of presbyopia was made in group 1 gradually, in steps of 0.25 D. The value of additional correction averaged 0.5 ± 0.13 D. The magnitude of additional correction was inversely related to age (r = 0.79). To assess the effectiveness of presbyopia overcorrection in reducing IOP 1 year later, tonometry, visual acuity check, perimetry (MD/year method), ophthalmoscopy, and measurement of the thickness of the ciliary body were performed. In group 1, the reduction of IOP (17.3 ± 0.84 mmHg) was statistically significant (p < 0.01), and its value was close to the average tolerant IOP (17.0 ± 0.67 mmHg), but was higher than the target (14.3 ± 0.67 mmHg). Also, in this group, statistically significant (p < 0.01) decrease in the thickness of the ciliary body was observed, more marked in patients with high near visual load (r = 0.47). Progression of glaucoma according to perimetry was significantly less (p < 0.01) in the group with hypercorrection of presbyopia as compared with the group with ordinary correction.
Conclusions
Overcorrection of presbyopia, in addition to antihypertensive therapy, may be a way to regulate IOP for patients with high near visual load and POAG.
Zusammenfassung
Einleitung
Das Ziel unserer Forschung war das Studium der Rolle des Sehbelastungsniveaus in der Augeninnendrucksteigerung der Patienten, die die Analoga des Prostaglandins benutzen, und der Versuch, die Bedingungen für ihre Wirkung auf den Uveosklerabfluss zu optimieren.
Materialien und Methoden
In die Studie wurden 33 Patienten (40 Augen) mit der zum ersten Mal gestellten Diagnose des primären Offenwinkelglaukoms und mit dem zum Latanoprostum 0,005 % resistenten Augeninnendruck eingeschlossen. Diese Patienten wurden vorher untersucht, indem man die Sehkraft in die Ferne und in der Nähe, Refraktion, echten, toleranten und zweckgebundenen Augeninnendruck mit der Perimetrie und Ophthalmoskopie bestimmte. Die Probanden wurden in zwei Gruppen mit dem vergleichbaren Alter, Geschlecht und Refraktion geteilt. In jeder Gruppe wurden die Dicke des Strahlenkörpers mithilfe der Ultraschallbiomikroskopie, das Niveau der Nahsehbelastung und die verträgliche Nahkorrektion bestimmt.
Ergebnisse
Es wurde festgestellt, dass es in den beiden Gruppen in 85 % von Augen mit dem primären Offenwinkelglaukom eine mäßig hohe (3–6 h pro Tag) und hohe (mehr als 6 h pro Tag) Nahsehbelastung gab. Die maximale Dicke des Strahlenkörpers in den beiden Gruppen war wesentlich höher, als die von anderen Autoren festgestellten Angaben: 0,881 ± 0,039 mm in der 1. Gruppe und 0,889 ± 0,049 mm in der 2. Gruppe. Auch ließ sich eine gerade Abhängigkeit der Strahlenkörperdicke von dem echten Augeninnerdruck (r = 0,52) beobachten. Die Hyperkorrektion der Presbyopie wurde in der 1. Gruppe allmählich, mit dem Schritt 0,25 D verschrieben. Der Wert der zusätzlichen Korrektion betrug im Durchschnitt 0,5 ± 0,13 D. Die Größe der zusätzlichen Korrektion war dem Alter indirekt proportional (r = 0,79). Zur Bewertung der Hyperkorrektionseffizienz der Presbyopie in der Reduktion des Augeninnendnucks wurden Tonometrie, Sehschärfekontrolle, Perimetrie (Methode MD/Jahr), Ophthalmoskopie, Messung der Strahlenkörperdicke durchgeführt. In der 1. Gruppe war die Reduktion des Augeninnendrucks (17,3 ± 0,84 mmHg) statistisch bedeutsam (p < 0,01), ihr Wert war dem durchschnittlichen toleranten Augeninnendrucks (17,0 ± 0,67 mmHg) nah, aber höher, als zweckgebundener (14,3 ± 0,67 mmHg). Auch war in dieser Gruppe eine statistisch bedeutsame Reduktion der Dicke des Strahlenkörpers (p < 0,01), die mehr bei den Patienten mit der hohen Nahsehbelastung (r = 0,47) ausgeprägt war, zu beobachten. Die Glaukomprogredienz war laut der Perimetrie in der Gruppe mit der Hyperkorrektion der Presbyopie im Vergleich zu einfacher Korrektion viel geringer (p < 0,01).
Schlussfolgerungen
Die Hyperkorrektion der Presbyopie als Mittel der Regulation des Augeninnendrucks könnte eine Ergänzung zu der Antihypertensivtherapie für die Patienten mit der hohen Nahsehbelastung und dem primären Offenwinkelglaukom sein.

Similar content being viewed by others


References
Ge J, Zhao JL, Cui H. Ophthalmology. Beijing: People’s Medical Publishing House; 2005. pp. 246–73.
Adatia FA, Damji KF. Chronic open-angle glaucoma. Review for primary care physicians. Can Fam Physician. 2005;51:1229–37.
Heijl A, Leske MC, Bengtsson B, Hyman L, Bengtsson B, Hussein M. Early manifest glaucoma trial group. Reduction of intraocular pressure and glaucoma progression: results from the early manifest glaucoma trial. Arch Ophthalmol. 2002;120(10):1268–79.
Van Buskirk EM, Cioffi GA. Glaucomatous optic neuropathy. Am J Ophthalmol. 1992;113(4):447–52.
Quigley HA. Number of people with glaucoma worldwide. Br J Ophthalmol. 1996;80(5):389–93.
Lichter PR, Musch DC, Gillespie BW, Guire KE, Janz NK, Wren PA. Interim clinical outcomes in the Collaborative Initial Glaucoma Treatment Study comparing initial treatment randomized to medications or surgery. Ophthalmology. 2001;108:1943–53.
Gordon MO, Beiser JA, Brandt JD, Heuer DK, Higginbotham EJ, Johnson CA, et al. The Ocular Hypertension Treatment Study: baseline factors that predict the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120:714–20.
Jampel HD. Target pressure in glaucoma therapy. J Glaucoma. 1997;6(2):133–8. Review.
Iomdina EN, Ignat’eva NIu, Danilov NA, Arutiunian LL, Kiseleva OA, Nazarenko LA. Biochemical, structural and biomechanical features of human scleral matrix in primary open-angle glaucoma. Vestn Oftalmol. 2011;127(6):10–4.
Koshits IN, Svetlova OV, Zaseeva MV, Shukhaev SV, Makarov FN, Kotliar KE, Smolnikov BA. Physiological principles of hypotensive therapy of openangle glaucoma during presbyopia period. Part I. Initial theoretical presuppositions, hypotheses and facts. Glaukoma. 2006;3:35–70.
Koshits IN, Svetlova OV, Zaseeva MV, Shukhaev SV, Makarov FN, Kotliar KE, Smolnikov BA. Physiological principles of hypotensive therapy of open-angle glaucoma during presbyopia period. Part II. Perspective algorithms of practical sparing effects. Glaukoma. 2006;4:51–70.
Balalin SV, Fokin VP. On tolerated and target-oriented intraocular pressure in primary open-angle glaucoma. Rus Med J. 2008;9:117–9.
Chauhan BC, Garway-Heath DF, Goñi FJ, et al. Practical recommendations for measuring rates of visual field change in glaucoma. Br J Ophthalmol. 2008; 92(4):569–73.
European Glaucoma Society. Terminology and guidelines for glaucoma. Savona: Editrice DOGMA; 2008. pp. 82–8.
Lossing LA, Sinnott LT, Kao CY, Richdale K, Bailey MD. Measuring changes in ciliary muscle thickness with accommodation in young adults. Optom Vis Sci. 2012;89(5):719–26.
Egorova EV, Bessarabov AN, Uzunyan DG, Sarukhanyan AA. Anatomy-topographic features of the eyes in various types of refraction and their changes in glaucoma according to the results of ultrasonic biomicroscopy. Glaukoma. 2006;2:17–23.
Bezdetko P, Abdoola, AMD, Shchadnykh M. Anterior segment morphometric parameters of presbyopic eyes with and without POAG and varying refraction. Kharkiv Surg Sch. 2012;4:84–7.
Ethical standards
All patients gave informed consent to take part in the study. The research was performed according to the principles of the Helsinki Declaration and was approved by the ethical committees.
Conflict of interests
The authors declare that there is no conflict of interests regarding the publication of this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Shchadnykh, M., Bezditko, P. Optimization of the uveoscleral outflow in the patients with primary open-angle glaucoma and resistant to latanoprost intraocular pressure. Spektrum Augenheilkd. 28, 148–152 (2014). https://doi.org/10.1007/s00717-014-0222-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00717-014-0222-9
Keywords
- Primary open-angle glaucoma
- Resistant intraocular pressure
- Near visual load levels
- Presbyopia correction
- Maximal ciliary body thickness