
Abstract
Background
Vertebral artery aneurysms account for less than 5% of all cerebral aneurysms. They have a high risk of rupture and are associated with threatening clinical outcomes compared with anterior circulation aneurysms.
Method
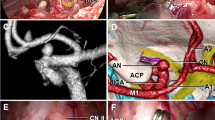
The endoscopic endonasal transclival approach (EETA) was used. During the temporary clipping, the neck of the aneurysm was dissected, and a permanent clip was applied. The repair of the skull base defect was carried out with the nasoseptal mucoperiosteal flap on the vascular pedicle.
Conclusion
The EETA is a feasible alternative for the clipping of the medially located ruptured vertebral artery aneurysm. EETA can be recommended for centers with a large volume of cerebrovascular and endoscopic neurosurgical procedures.





Similar content being viewed by others


Data Availability
All data generated or analyzed during this study are included in this published article and its supplementary information files.
References
Ali AMS, Hannan CJ, Islim AI, Mascitelli JR, Javadpour M (2022) Surgical and endovascular treatment of saccular posterior inferior cerebellar artery aneurysms: systematic review and meta-analysis. World Neurosurg 162:e168–e177
Doan V, Lemos-Rodriguez AM, Sreenath SB, Unnithan A, Recinos PF, Zanation AM, Sasaki-Adams DM (2016) Using the endoscopic endonasal transclival approach to access aneurysms arising from AICA, PICA, and vertebral artery: an anatomical study. J Neurol Surg B Skull Base 77(3):207–211
Gardner PA, Vaz-Guimaraes F, Jankowitz B, Koutourousiou M, Fernandez-Miranda JC, Wang EW, Snyderman CH (2015) Endoscopic endonasal clipping of intracranial aneurysms: surgical technique and results. World Neurosurg 84(5):1380–1393
Guan J, Li G, Kong X, He C, Long J, Qin H, Zhang H, Wang R (2017) Endovascular treatment for ruptured and unruptured vertebral artery dissecting aneurysms: a meta-analysis. J Neurointerv Surg 9(6):558–563
Harvey RJ, Parmar P, Sacks R, Zanation AM (2012) Endoscopic skull base reconstruction of large dural defects: a systematic review of published evidence. Laryngoscope 122(2):452–459
Morera VA, Fernandez-Miranda JC, Prevedello DM, Madhok R, Barges-Coll J, Gardner P, Carrau R, Snyderman CH, Rhoton AL, Kassam AB (2010) “Far-medial” expanded endonasal approach to the inferior third of the clivus: the transcondylar and transjugular tubercle approaches. Neurosurgery 66(6 Suppl Operative):ons211–ons220
Morita A, Kirino T, Hashi K et al (2012) The natural course of unruptured cerebral aneurysms in a Japanese cohort. N Engl J Med 366(26):2474–2482
Sanai N, Tarapore P, Lee AC, Lawton MT (2008) The current role of microsurgery for posterior circulation aneurysms: a selective approach in the endovascular era. Neurosurgery 62(6):1236–1249
Spetzler RF, McDougall CG, Zabramski JM, Albuquerque FC, Hills NK, Russin JJ, Partovi S, Nakaji P, Wallace RC (2015) The barrow ruptured aneurysm trial: 6-year results. J Neurosurg 123(3):609–617
Wiebers DO (2003) Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet 362(9378):103–110
You W, Meng J, Yang X, et al (2022) Microsurgical management of posterior circulation aneurysms: a retrospective study on epidemiology, outcomes, and surgical approaches. Brain Sciences 2022, 12, 1066 12(8):1066
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Informed consent
The patients have consented to the submission of this How I Do It for submission to the journal.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key points
1. Individual selection of patients with medially located VA aneurysms.
2. Individual approach planning using intraoperative neuronavigation.
3. Harvesting the NMF on the vascular pedicle, as well as a bone fragment of the nasal septum, for the subsequent repair of the skull base defect.
4. Performing an EETA.
5. Identification of VA, BA, PICA, and abducens nerves before clipping.
6. Achieving minimal prolapse of permanent clips into the skull base defect.
7. Performing multilayer repair of the skull base defect using an NMF on the vascular pedicle, a bone fragment of the nasal septum, and fibrin-thrombin glue.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary video (MP4 18242 KB)
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Dzhindzhikhadze, R., Kambiev, R., Polyakov, A. et al. How I do it: the endoscopic endonasal transclival approach for clipping of the ruptured vertebral artery aneurysm. Acta Neurochir 165, 2825–2830 (2023). https://doi.org/10.1007/s00701-023-05606-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-023-05606-6