
Abstract
Background
In recent years, thanks to several technological innovations, stereotactic cerebral biopsies have evolved from frame-based to frameless neuronavigation-assisted techniques.
Methods
The authors provide herein a detailed step-by-step description of the technique, shedding light on surgical tips and how to avoid complications. The practical application of the technique is demonstrated with a high-quality video.
Conclusion
The neuronavigation-assisted brain biopsy with electromagnetic tracking is a “true frameless” procedure. It represents a simple, safe, and effective innovation for frameless biopsy of cerebral lesions. This technique is time efficient, offering a high degree of accuracy required for the establishment of a definitive diagnosis, enabling optimal further treatment, and thus improving patient outcome.



Similar content being viewed by others


Abbreviations
- EM:
-
Electromagnetic
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
- WI:
-
Weighted images
- DTI:
-
Diffusion tensor imaging
References
Æbelø AM, Noer VR, Schulz MK, Kristensen BW, Pedersen CB, Poulsen FR (2019) Frameless stereotactic neuronavigated biopsy: a retrospective study of morbidity, diagnostic yield, and the potential of fluorescence. Clin Neurol Neurosurg 181(March):28–32
Bertuccio A, Elia A, Robba C, Scaglione G, Longo GP, Sgubin D, Vitali M, Barbanera A (2020) Frameless stereotactic biopsy with DTI-based tractography integration: how to adjust the trajectory-a case series. World Neurosurg 143:346–352
Dhawan S, He Y, Bartek J, Alattar AA, Chen CC (2019) Comparison of frame-based versus frameless intracranial stereotactic biopsy: systematic review and meta-analysis. World Neurosurg 127:607-616.e4
Giamouriadis A, Perera D, Safdar A, Vergani F, Bhangoo R, Gullan R, Ashkan K (2019) Safety and accuracy of frameless electromagnetic-navigated (AXIEMTM)-guided brain lesion biopsies: a large single-unit study. Acta Neurochir (Wien) 161(12):2587–2593
McMillen JL, Vonau M, Wood MJ (2010) Pinless frameless electromagnetic image-guided neuroendoscopy in children. Child’s Nerv Syst 26(7):871–878
Mohyeldin A, Elder JB (2017) Stereotactic biopsy platforms with intraoperative imaging guidance. Neurosurg Clin N Am 28(4):465–475
Paleologos TS, Dorward NL, Wadley JP, Thomas DGT (2001) Clinical validation of true frameless stereotactic biopsy: analysis of the first 125 consecutive cases. Neurosurgery 49(4):830–837
Riche M, Amelot A, Peyre M, Capelle L, Carpentier A, Mathon B (2021) Complications after frame-based stereotactic brain biopsy: a systematic review. Neurosurg Rev 44(1):301–307
Sciortino T, Fernandes B, Conti Nibali M et al (2019) Frameless stereotactic biopsy for precision neurosurgery: diagnostic value, safety, and accuracy. Acta Neurochir (Wien) 161(5):967–974
Thien A, Rao JP, Ng WH, King NKK (2017) The fluoropen: a simple low-cost device to detect intraoperative fluorescein fluorescence in stereotactic needle biopsy of brain tumors. Acta Neurochir (Wien) 159(2):371–375
Author information
Authors and Affiliations
Contributions
Conceptualization: GA. Methodology: AD. Formal analysis and investigation: PV. Writing — original draft preparation: PV and GA. Writing — review and editing: AD and DL. Supervision: DL.
Corresponding author
Ethics declarations
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent to participate
Informed consent was obtained from all the patients included in this study.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key points
1. Brain biopsy aims to provide the diagnosis of cerebral lesions of unknown origin.
2. A recent meta-analysis did not show significant differences between the frame-based and frameless techniques regarding the diagnostic yield, morbidity, and mortality.
3. Frameless techniques avoid the usage of the Mayfield head holder, making the procedure easier, faster, and more comfortable to the patient.
4. Before surgery, it is crucial to obtain a complete neuroimaging assessment with both CT and MRI scans.
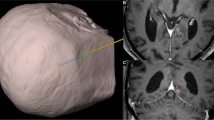
5. Once the images are uploaded to the workstation, the target and the trajectory are established, paying attention to respect eloquent neurovascular structures.
6. DTI tractography can be elaborated and added to the plan, to avoid crossing white matter pathways.
7. When the intraoperative registration with the EM system is performed, an error of < 1.5 mm is acceptable.
8. During the procedure, before harvesting the sample, the accuracy of the neuronavigation should be checked according to well-known anatomical landmarks. Hitting the target is crucial!
9. Intraoperative fluorescein and frozen sample analysis reduces dramatically the risk of non-diagnosis.
10. Patients should be always aware of the advantages, disadvantages, and alternative options.
This article is part of the Topical Collection on Neurosurgical Technique Evaluation.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (MP4 156284 KB)
Rights and permissions
About this article

Cite this article
Veiceschi, P., Locatelli, D., Dario, A. et al. Frameless neuronavigation-assisted brain biopsy with electromagnetic tracking: how I do it?. Acta Neurochir 164, 3317–3322 (2022). https://doi.org/10.1007/s00701-022-05252-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-022-05252-4