
Abstract
Purpose
Some patients have worse actual observed postoperative (apo) respiratory function values than predicted postoperative (ppo) values. The present study therefore clarified the predictive factors that hinder the recovery of the postoperative respiratory function.
Methods
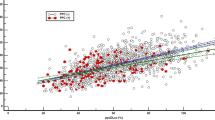
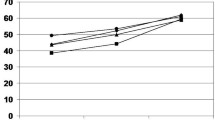
This study enrolled 255 patients who underwent anatomical pulmonary resection for lung cancer. A pulmonary function test (PFT) was carried out before surgery and at one, three, and six months after surgery. In each surgical procedures, the forced expiratory volume in 1 s (FEV1) ratio was calculated as the apo value divided by the ppo value. In addition, we investigated the predictive factors that inhibited postoperative respiratory function improvement in patients with an FEV1 ratio < 1.0 at 6 months after surgery.
Results
The FEV1 ratio gradually improved over time in all surgical procedures. However, 49 of 196 patients who underwent a PFT at 6 months after surgery had an FEV1 ratio < 1.0. In a multivariate analysis, right side, upper lobe, segmentectomy and pleurodesis for prolonged air leakage were independent significant predictors of a decreased FEV1 ratio (p = 0.003, 0.006, 0.001, and 0.009, respectively).
Conclusion
Pleurodesis was the only controllable factor that might help preserve the postoperative respiratory function. Thus, the intraoperative management of air leakage is important.



Similar content being viewed by others

Data availability
The data underlying this article cannot be shared publicly due to the privacy of individuals that participated in the study.
Abbreviations
- PFT:
-
Pulmonary function test
- FEV1:
-
Forced expiratory volume in 1 s
- VC:
-
Vital capacity
- DLCO:
-
Diffusing capacity of the lung for carbon monoxide
- ppo:
-
Predicted postoperative
- apo:
-
Actual observed postoperative
References
Sarna L, Evangelista L, Tashkin D, Padilla G, Holmes C, Brecht ML, et al. Impact of respiratory symptoms and pulmonary function on quality of life of long-term survivors of non-small cell lung cancer. Chest. 2004;125(2):439–45.
Pierce RJ, Copland JM, Sharpe K, Barter CE. Preoperative risk evaluation for lung cancer resection: predicted postoperative product as a predictor of surgical mortality. Am J Respir Crit Care Med. 1994;150:947–55.
Miyazaki T, Callister MEJ, Franks K, Dinesh P, Nagayasu T, Brunelli A. Minute ventilation-to-carbon dioxide slope is associated with postoperative survival after anatomical lung resection. Lung Cancer. 2018;125:218–22.
Kearney DJ, Lee TH, Reilly JJ, DeCamp MM, Sugarbaker DJ. Assessment of operative risk in patients undergoing lung resection. Importance of predicted pulmonary function. Chest. 1994;105:753–9.
Wang JS. Relationship of carbon monoxide pulmonary diffusing capacity to postoperative cardiopulmonary complications in patients undergoing pneumonectomy. Kaohsiung J Med Sci. 2003;19:437–46.
Brunelli A, Charloux A, Bolliger CT, Rocco G, Sculier JP, Varela G, et al. ERS/ESTS clinical guidelines on fitness for radical therapy in lung cancer patients (surgery and chemo-radiotherapy). Eur Respir J. 2009;34:17–41.
Korst RJ, Ginsberg RJ, Ailawadi M, Bains MS, Downey RJ Jr, Rusch VW, et al. Lobectomy improves ventilatory function in selected patients with severe COPD. Ann Thorac Surg. 1998;66:898–902.
Ueda K, Murakami J, Sano F, Hayashi M, Kobayashi T, Kunihiro Y, et al. Assessment of volume reduction effect after lung lobectomy for cancer. J Surg Res. 2015;197:176–82.
Brunelli A, Refai MA, Salati M, Sabbatini A, Morgan-Hughes NJ, Rocco G. Carbon monoxide lung diffusion capacity improves risk stratification in patients without airflow limitation: evidence for systematic measurement before lung resection. Eur J Cardiothorac Surg. 2006;29:567–70.
Ferguson MK, Vigneswaran WT. Diffusing capacity predicts morbidity after lung resection in patients without obstructive lung disease. Ann Thorac Surg. 2008;85:1158–64.
Yokoba M, Ichikawa T, Harada S, Naito M, Sato Y, Katagiri M. Postoperative pulmonary function changes according to the resected lobe: a 1-year follow-up study of lobectomized patients. J Thorac Dis. 2018;10(12):6891–902.
Takamochi K, Imashimizu K, Fukui M, Maeyashiki T, Suzuki M, Ueda T, et al. Utility of objective chest tube management after pulmonary resection using a digital drainage system. Ann Thorac Surg. 2017;104:275–83.
Fukui M, Takamochi K, Suzuki K, Ando K, Matsunaga T, Hattori A, et al. Advantages and disadvantages of corticosteroid use for acute exacerbation of interstitial pneumonia after pulmonary resection. Gen Thorac Cardiovasc Surg. 2021;69:472–7.
Brunelli A, Refai M, Salati M, Xiume F, Sabbatini A. Predicted versus observed FEV1 and DLCO after major lung resection: a prospective evaluation at different postoperative periods. Ann Thorac Surg. 2007;83:1134–9.
Nomori H, Shiraishi A, Cong Y, Sugimura H, Mishima S. Differences in postoperative changes in pulmonary functions following segmentectomy compared with lobectomy. Eur J Cardiothorac Surg. 2018;53:640–7.
Okada M, Koike T, Higashiyama M, Yamato Y, Kodama K, Tsubota N. Radical sublobar resection for small-sized non-small cell lung cancer: a multicenter study. J Thorac Cardiovasc Surg. 2006;132:769–75.
Ueda K, Tanaka T, Hayashi M, Li TS, Tanaka N, Hamano K. Computed tomography-defined functional lung volume after segmentectomy versus lobectomy. Eur J Cardiothorac Surg. 2010;37:1433–7.
Deng B, Cassivi SD, de Andrade M, Nichols FC, Trastek VF, Wang Y, et al. Clinical outcomes and changes in lung function after segmentectomy versus lobectomy for lung cancer cases. J Thorac Cardiovasc Surg. 2014;148:1186–92.
Yoshimoto K, Nomori H, Mori T, Ohba Y, Shiraishi K, Tashiro K, et al. Postoperative change in pulmonary function of the ipsilateral preserved lung after segmentectomy versus lobectomy. Eur J Cardiothorac Surg. 2010;37:36–9.
Yamagishi H, Chen-Yoshikawa TF, Oguma T, Hirai T, Date H. Morphological and functional reserves of the right middle lobe: radiological analysis of changes after right lower lobectomy in healthy individuals. J Thorac Cardiovasc Surg. 2021;162:1417–23.
Irani B, Miller JE, Linberg E, Attar S. Use of radiopaque markings on middle lobe (or lingula) following upper resectional surgery. Ann Thorac Surg. 1968;5:1–7.
Maeyashiki T, Takamochi K, Matsunaga T, Oh S, Suzuki K. Negative impact of chemical pleurodesis on postoperative pulmonary function for managing prolonged air leakage after segmentectomy. Gen Thorac Cardiovasc Surg. 2021;69:707–15.
Acknowledgements
We would like to thank Editage (www.editage.com) for English language editing.
Funding
This work was supported in part by a Grant-in-Aid for Cancer Research from the Ministry of Health, Labour, and Welfare of Japan, and the Smoking Research Foundation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ueno, H., Takamochi, K., Hirayama, S. et al. Predictive factors inhibiting recovery of the respiratory function after anatomical pulmonary resection. Surg Today 53, 1081–1088 (2023). https://doi.org/10.1007/s00595-023-02666-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-023-02666-0