
Abstract
Purpose
To review the epidemiological characteristics of proximal femur fractures in the young population (< 60 years) of Qatar between 2017 and 2019.
Methods
All patient treated for proximal femur fractures at Hamad General Hospital (HGH), a level one trauma center, were retrospectively reviewed between Jan 2017 and Dec 2019. All adults (18–60 years) with proximal femur fracture (femur head, femur neck, intertrochanteric and subtrochanteric fractures) were included with no restriction to the AO/OTA classification or fractures subtypes. Excluded cases were pathological fractures, cases with insufficient documentation or no radiographs.
Results
A total of 203 patients with a mean age of 40.07 ± 11.76 years were included, of who 89.9% were males. The incidence of proximal femur fracture was 3.12/100,000/year. Fall from height (48.1%) followed by road traffic accidents (26.9%) were common cause of injury. The most common fracture type was intertrochanteric fracture (36.1%) followed by femur neck fractures (33.7%).
Conclusion
This study provides the initial insights into the proximal femur fractures in the young population of Qatar. This is the first study to investigate of the epidemiology of such fractures in this particular patient group. Contrary to the existing literature on older age groups, the majority of the injuries were observed in males. Falls from height followed by road traffic accidents were the primary mechanisms leading to these fractures. Improved understanding of the profile of these injuries can aid in their prevention by implementing more effective safety measures.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The incidence of hip fractures has been increasing significantly over the last decades [1]. It is estimated that the annual incidence of hip fractures will rise up to 6 million fractures worldwide by the year 2050, 70% of which occurring in Asia, Latin America, the Middle East and Africa [2, 3].
Increased life expectancy and activity levels in older age, in addition to increased survival rates among younger trauma patients, explain the exponential rise in hip fracture rates [4]. As a result of this dramatic rise, the burden on health systems is expected to increase exponentially [5]. Up to 20 billion dollars are spent annually on hip fractures, making this type of fractures one of the most expensive fractures to treat [5]. Moreover, mortality rates of hip fractures are estimated to exceed 20% within one year and this percentage rises dramatically over time as the functional status of hip fracture patients deteriorates [6].
Hip fractures can be classified into intracapsular, such as femoral neck fractures, and extracapsular such as intertrochanteric and subtrochanteric fractures. Age distribution, mechanism of injury, management and outcomes differ between the different types and subtypes [1].
Qatar has one of the fastest growing economies in the world. The country’s rapid development has a substantial impact on its demographics and health indicators. More than 70% of the population are young expatriate male workers and approximately 83% of who falls within the age range of 15–65 years [7, 8]. This in turn, affects the incidence as well as the characteristics of hip fractures and their management.
As hip fractures have a significant impact on quality of life and increase morbidity and mortality, it is paramount to conduct an epidemiological study to investigate the incidence, characteristics and patterns of hip fractures in Qatar. Therefore, the aim of this retrospective epidemiological study is to review the epidemiological aspects of hip fractures of the young population (< 60 years) managed at Hamad General Hospital, the only level 1 trauma center in Qatar, between Jan 2017 and Dec 2019. We hypothesized that there is a higher incidence rate of hip fractures in young patients in Qatar as compared to other regions of the world.
Methods
Study design
Approval was obtained from the institutional review board at HGH, the only level one-trauma center in Qatar. All cases that were treated for proximal femur fractures at HGH, were retrospectively reviewed between Jan 2017 and Dec 2019.
Eligibility criteria
The inclusion criteria were all adults (18–60 years) with proximal femur fracture (femur head, femur neck, intertrochanteric or subtrochanteric fractures) that were treated at HGH between Jan 2017 and Dec 2019. All fracture patterns were included with no restriction to the AO/OTA classification or fractures subtypes [9]. Excluded cases were pathological fractures, cases with insufficient documentation or no radiographs.
Data source and collection
Data retrieved from the patients’ electronic medical files was assessed to identify eligible patients diagnosed with proximal femur fractures. The data items that were collected included: age, gender, comorbidities, bone marrow density, mechanism of injury, fracture classification, associated injuries, treatment modality, admission-to-surgery time, length of stay, and complications, reoperations and mortality.
Fracture classification
Fractures were classified according to the anatomic location of the fracture (femur head, femoral neck, intertrochanteric and subtrochanteric fractures) and the AO/OTA classification, which proposes a uniform alphanumerical classification [9]. Subclassifications were also performed to femur neck fractures as per Pauwels’ angle and Garden’s classification [10, 11].
Statistical analysis
The data analysis was done using IBM-SPSS v.25. Categorical variables were presented as counts and percentages whereas continuous variables were interpreted as mean, standard deviation and range. The difference in the characteristics according to the outcomes of the patients was done using Chi-square test and T-test for categorical and continuous variables, respectively. Any test with a P-value < 0.05 was considered significant.
Results
The total number of the included patients between Jan 2017 and Dec 2019 was 203, four of whom had bilateral injuries and one patient had two fractures on two separate occasions. The overall incidence of PFF fractures between 2017 and 2019 was 3.12 per 100,000 population per year. The incidence in 2017 was 2.89 per 100,000 population per year (61 cases). Moreover, the incidence was 3.46 (75 cases) and 3.02 (67 cases) per 100,000 population per year in 2018 and 2019, respectively (Fig. 1). Table 1 demonstrates the demographic characteristics of the participants.

Proximal femur fractures at HGH between 2017 and 2019. NOF Neck of femur, IT Intertrochanteric, ST Subtrochanteric
Trends in age and gender
The mean age of the included patients was 40.07 ± 11.76. The majority of the fractures were in the age group from 30 to 40 followed by the group from 40 to 50 while the lowest number of fractures was in the age group less than 20. Figure 2 shows the trends of fractures according to the age group. The majority of the patients were males (89.9%). The most common side of the injury was right side (53.1%) and 2.5% of the patients had bilateral injury.

Number of fractures according to age group
Mechanism of injury
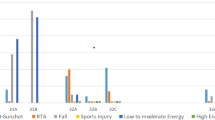
The majority of the injuries were due to fall from height (48.1%) while 26.9% of them were due to road traffic accidents (RTA). Figure 3 demonstrates the correlation between the mechanism of injury and age of the patients over the 3-year period. The majority of the fractures in the age groups higher than 30 years of age was due to fall from height, whereas the majority of fractures in the age groups 20–30 and less than 20 were due to RTA.

Mechanism of injury according to age group
Type of fractures and classifications
The most common type of proximal femoral fractures was intertrochanteric (36.1%) followed by femoral neck fractures (33.7%). Most of the fractures in the age groups 20–30, 30–40, and 40–50 were intertrochanteric fractures while the majority of the fractures in the age group ≥ 50 were femoral neck fractures (Fig. 4). Most of the fractures were classified as B2 (37.1%) followed by class A1 (22.6%) as per the AO/OTA classification. Additionally, 68.6% of the patients with femoral neck fractures were classified as P3 fractures and 30.1% of them were classified as G3 fractures (Table 2).

Fracture type according to age group
Treatment options
All patients were treated operatively. The most commonly utilized implant was caphalomedullary nail (46.7%) followed by cannulated screws (23%) and dynamic hips screw (22.5%). Only 2 patients with femoral neck fractures underwent uncemented hemiarthroplasty. The two cases of femoral head fractures were treated operatively with open reduction and screws fixation. Table 3 demonstrates a summary of treatment options.
Associated injuries, complications and length of hospital stay
The frequency of complications was 18.3% and the frequency of reoperations was 10.3%. On the other hand, there were no mortalities in 2017, 2018 and 2019. The mean length of hospital stays and follow up period were 10.30 ± 21.54 and 990.0 ± 128.38 days, respectively (Table 4).
Discussion
Our review demonstrated a total incidence rate of 3.12 proximal femur fractures per 100,000 population per year between 2017 and 2019, with the majority of fractures occurring in male patients and those between 30 and 40 years of age, predominantly due to falls from height. Whereas proximal femur fractures have been previously reported to affect women more than men globally, particularly in the older age group, our results showed the opposite to be true in those younger than 60 years of age. As previously noted, more than 70% of the population of Qatar is made up of migrant male workers who fall within this age group. A technical report conducted by the Gulf Research Centre surveying the demography, migration, and labour market of Qatar in 2014 found the average age of expatriate male labourers to be 34 years [12]. Another paper aiming to outline a socio-economic profile of migrants in Qatar identified a median age of 31 years [13]. It is likely that these factors have influenced the proportion of patient characteristics described above.
The leading mechanism of injury, identified as falls from height above the age of 30 and road traffic accidents below the age of 30, provides insight into the likely circumstances under which patients are exposed to risk. The prevalence of falls from height in the working population, most of which may be work-related injuries occurring at building sites, highlights the importance of ensuring and enforcing on-site occupational safety standards. Similarly, the high prevalence of road traffic accidents in younger people under the age of 30 has been well-documented. Specifically in Qatar, young drivers in the age group 25–34 have been shown to experience the highest rate RTAs, most of whom are male drivers [14]. Road safety awareness campaigns directed toward this group of drivers may show to be useful in decreasing the incidence of fractures within this age group in the long term.
The incidence of PFF is highly variable across the world depending on the region and ethnicity studied. The highest rates have been reported in Sweden and North America, with lower rates in European countries by seven-fold, and even lower across Asia [15]. However, it is projected that more than half of all hip fractures will occur in Asia by the year 2050 [16]. Table 5 shows the incidence rates reported in previous literature from different regions of the world. Notably, most reports studied the incidence of PFF in patients aged 50 and above, a group in which osteoporosis may lead to increasingly rising rates of fracture with the dominant risk factor being older age [41], and many of these studies excluded high-energy mechanism injuries in the younger age group. There are very few previous reports aiming to identify PFF incidence rates among the non-elderly adult population. One study conducted in the Netherlands and Sweden of 1115 proximal femur fractures in 1989–1990 found only 2% of patients under 50 years of age with proximal femur fractures, which were attributed to severe trauma [42]. Thus, it is difficult to ascertain whether proximal femur fractures occur at a greater incidence among the young age group in the State of Qatar as compared with other regions of the world.
Amongst our studied population, the most common pattern of proximal femur fractures was intertrochanteric (36.1%), followed by femoral neck fractures (33.7%). Similar findings have been reported in previous literature [43,44,45]. Intertrochanteric fractures were most observed in patients younger than 50 years of age, whereas femoral neck fractures were observed in those older than 50. The opposite is true in previous literature. A study of 737 patients conducted in Baltimore between 1984 and 1986 found intertrochanteric fracture patients were older than those with femoral neck fractures [46]. In New York, a study of 717 patients between 1987 and 1994 found patients with intertrochanteric fractures to be older than femoral neck fracture patients [47]. Similarly, a study of 248 patients in Istanbul Turkey in 2008 found intertrochanteric fracture patients were significantly older than femoral neck fracture patients [48]. Another retrospective study found lower bone mineral density values among patients with intertrochanteric fractures when compared to femoral neck fractures [49]. However, the majority of the patients included in previous studies were of the elderly population with higher rates of osteoporosis presenting after simple falls. The inclusion of younger patients and high-energy mechanism injuries in our study may have given rise to this variation.
Limitations
It is important to acknowledge that data was collected in a retrospective manner which might have introduced selection bias. In addition, the accuracy of the data is reliant upon the quality of documentation. Furthermore, as many patients return to their home country following the completion of their treatment, it was not possible to gather long-term follow up data and identify long-term complications.
Conclusion
This study provides the initial insights into the proximal femur fractures in the young population of Qatar, shedding light on their distinct characteristics. This is the first study to investigate of the epidemiology of such fractures in this particular patient group. Remarkably, Contrary to the existing literature on older age groups, the majority of the injuries were observed in males. Falls from height followed by road traffic accidents were the primary mechanisms leading to these fractures. Improved understanding of the profile of these injuries can aid in their prevention by implementing more effective safety measures.
Availability of code, data and material
Not applicable.
References
Lu Y, Uppal H (2019) Hip fractures: relevant anatomy, classification, and biomechanics of fracture and fixation. Geriatr Orthop Surg Rehabil 10:2151459319859139. https://doi.org/10.1177/2151459319859139
Cummings SR, Kelsey JL, Nevitt MC, O’Dowd KJ (1985) Epidemiology of osteoporosis and osteoporotic fractures. Epidemiol Rev 7:178–208. https://doi.org/10.1093/oxfordjournals.epirev.a036281
Maalouf G, Bachour F, Hlais S, Maalouf NM, Yazbeck P, Yaghi Y, Yaghi K, El Hage R, Issa M (2013) Epidemiology of hip fractures in Lebanon: a nationwide survey. Orthop Traumatol Surg Res 99(6):675–680. https://doi.org/10.1016/j.otsr.2013.04.009.2013
Egol KA, Leucht P (2018) Proximal femur fractures: an evidence-based approach to evaluation and management. Springer International Publishing, Cham
Roberts KC, Brox WT, Jevsevar DS, Sevarino K (2015) Management of hip fractures in the elderly. J Am Acad Orthop Surg 23(2):131–137
Cooper C (1997) The crippling consequences of fractures and their impact on quality of life. Am J Med 103(2):S12–S19. https://doi.org/10.1016/S0002-9343(97)90022-X
Ahmed M, Abuodeh Y, Alhammoud A, Salameh M, Hasan K, Ahmed G (2018) Epidemiology of acetabular fractures in Qatar. Int Orthop 42(9):2211–2217. https://doi.org/10.1007/s00264-018-3824-z
Population ages 15–64 (% of total population), World Bank Open Data. Available at: https://data.worldbank.org/indicator/SP.POP.1564.TO.ZS
Meinberg EG, Agel J, Roberts CS, Karam MD, Kellam JF (2018) Fracture and dislocation classification compendium—2018. J Orthop Trauma 32(Suppl 1):S1–S10. https://doi.org/10.1097/BOT.0000000000001063
Pauwels F (1935) Der Schenkenholsbruck, em mechanisches Problem. Grundlagen des Heilungsvorganges. Prognose und Kausale Therapie. Stuttgart, Beilageheft zur Zeitschrift fur Orthopaedische Chirugie, Ferdinand Enke
Van Embden D, Rhemrev SJ, Genelin F, Meylaerts SA, Roukema GR (2012) The reliability of a simplified garden classification for intracapsular hip fractures. Orthop Traumatol Surg Res 98(4):405–408. https://doi.org/10.1016/j.otsr.2012.02.003. (Epub 2012 May 3 PMID: 22560590)
De Bel-Air F (2014) Demography, migration, and labour market in Qatar. Gulf Research Center. Available at: https://cadmus.eui.eu/bitstream/handle/1814/32431/GLMM_ExpNote_08%E2%80%932014.pdf?sequence=1
Seshan G (2012) Migrants in Qatar: a socio-economic profile. J Arab Stud 2(2):157–171. https://doi.org/10.1080/21534764.2012.735458
Bener A (2012) A study on road traffic crashes and injuries in Qatar as reported by drivers. J Egypt Public Health Assoc 87(56):85–89. https://doi.org/10.1097/01.EPX.0000421566.38407.94
Dhanwal DK, Dennison EM, Harvey NC, Cooper C (2011) Epidemiology of hip fracture: worldwide geographic variation. Indian J Orthop 45(1):15–22. https://doi.org/10.4103/0019-5413.73656
Cooper C, Campion G, Melton LJ (1992) Hip fractures in the elderly: a world-wide projection. Osteoporos Int 2:285–289. https://doi.org/10.1007/BF01623184
Moayyeri A, Soltani A, Larijani B et al (2006) Epidemiology of hip fracture in Iran: results from the Iranian multicenter study on accidental injuries. Osteoporos Int 17:1252–1257. https://doi.org/10.1007/s00198-006-0105-2
Beyranvand M, Mohammadi G (2009) Incidence of hip fracture in Kermanshah, Iran. Arch Osteoporos 4:67–70. https://doi.org/10.1007/s11657-009-0030-z
Memon A, Pospula WM, Tantawy QY, Abdul-Ghafar S, Suresha A, Al-Rowaih A (1998) Incidence of hip fracture in Kuwait. Int J Epidemiol 27(5):860–865. https://doi.org/10.1093/ije/27.5.860
Azizieh FY (2015) Incidence of hip fracture in Kuwait: a national registry-based study. Arch Osteoporos 10:40. https://doi.org/10.1007/s11657-015-0248-x
Sibai AM, Nasser W, Ammar W et al (2011) Hip fracture incidence in Lebanon: a national registry-based study with reference to standardized rates worldwide. Osteoporos Int 22:2499–2506. https://doi.org/10.1007/s00198-010-1468-y
Saleh YAL, Sulimani RA, Alomary S et al (2022) Incidence of hip fracture in Saudi Arabia and the development of a FRAX model. Arch Osteoporos 17:56. https://doi.org/10.1007/s11657-022-01085-x
Yan L, Zhou B, Prentice A, Wang X, Golden MHN (1999) Epidemiological study of hip fracture in Shenyang People’s Republic of China. Bone 24(2):151–155. https://doi.org/10.1016/S8756-3282(98)00168-9
Lau E, Lee J, Suriwongpaisal P et al (2001) The Incidence of hip fracture in four Asian countries: the Asian osteoporosis study (AOS). Osteoporos Int 12:239–243. https://doi.org/10.1007/s001980170135
Hagino H, Yamamoto K, Ohshiro H, Nakamura T, Kishimoto H, Nose T (1999) Changing incidence of hip distal radius, and proximal humerus fractures in Tottori prefecture, Japan. Bone 24(3):265–270. https://doi.org/10.1016/S8756-3282(98)00175-6
Miyasaka D, Endo N, Endo E et al (2016) Incidence of hip fracture in Niigata, Japan in 2004 and 2010 and the long-term trends from 1985 to 2010. J Bone Miner Metab 34:92–98. https://doi.org/10.1007/s00774-015-0648-4
Lakho MT, Bughio S, Khan A et al (2022) The incidence of hip fractures in the study population: a retrospective study. Int J Curr Res Rev 14(10):67–70
El Maghraoui A, Koumba BA, Jroundi I et al (2005) Epidemiology of hip fractures in 2002 in Rabat, Morocco. Osteoporos Int 16:597–602. https://doi.org/10.1007/s00198-004-1729-8
El Maghraoui A, Ngbanda AR, Bensaoud N et al (2013) Age-adjusted incidence rates of hip fractures between 2006 and 2009 in Rabat, Morocco. Osteoporos Int 24:1267–1273. https://doi.org/10.1007/s00198-012-2061-3
Dela SS, Paruk F, Brown SL, Lukhele M, Kalla AA, Jordaan JD, Conradie M, Mohamed O, Chutterpaul P, Cassim B (2020) Ethnic and gender-specific incidence rates for hip fractures in South Africa: a multi-centre study. Bone 133:115253. https://doi.org/10.1016/j.bone.2020.115253
Kannus P, Parkkari J, Niemi S et al (2015) Low-trauma pelvic fractures in elderly Finns in 1970–2013. Calcif Tissue Int 97:577–580. https://doi.org/10.1007/s00223-015-0056-8
Wildner M, Casper W, Bergmann K (1999) A secular trend in hip fracture incidence in East Germany. Osteoporos Int 9:144–150. https://doi.org/10.1007/s001980050128
Lofthus CM, Osnes EK, Falch JA, Kaastad TS, Kristiansen IS, Nordsletten L, Stensvold I, Meyer HE (2001) Epidemiology of hip fractures in Oslo Norway. Bone 29(5):413–418. https://doi.org/10.1016/S8756-3282(01)00603-2
Czerwinski E, Kanis JA, Trybulec B et al (2009) The incidence and risk of hip fracture in Poland. Osteoporos Int 20:1363–1367. https://doi.org/10.1007/s00198-008-0787-8
Silva J, Linhares D, Ferreira M et al (2018) Epidemiological trends of proximal femoral fractures in the elderly population in Portugal. Acta Med Port 31(10):562–567. https://doi.org/10.20344/amp.10464
Bergh C, Wennergren D, Möller M, Brisby H (2020) Fracture incidence in adults in relation to age and gender: a study of 27,169 fractures in the Swedish fracture register in a well-defined catchment area. PLoS ONE 15(12):e0244291. https://doi.org/10.1371/journal.pone.0244291
Diez A, Puig J, Martinez MT et al (1989) Epidemiology of fractures of the proximal femur associated with osteoporosis in Barcelona, Spain. Calcif Tissue Int 44:382–386. https://doi.org/10.1007/BF02555965
Pang K, Ekeuku SO, Chin K-Y (2021) Particulate air pollution and osteoporosis: a systematic review. Risk Manag Healthc Policy 14:2715–2732
Morosano M, Masoni A, Sánchez A (2005) Incidence of hip fractures in the city of Rosario, Argentina. Osteoporos Int 16:1339–1344. https://doi.org/10.1007/s00198-005-1839-y
Bagur A, Mautalen C, Rubin Z (1994) Epidemiology of hip fractures in an urban population of Central Argentina. Osteoporosis Int 4:332–335. https://doi.org/10.1007/BF01622193
Hedlund R, Lindgren U (1987) Trauma type, age, and gender as determinants of hip fracture. J Orthop Res 5(2):242–246. https://doi.org/10.1002/jor.1100050210
Berglund-Rödén M, Swierstra BA, Wingstrand H, Thorngren KG (1994) Prospective comparison of hip fracture treatment: 856 cases followed for 4 months in the Netherlands and Sweden. Acta Orthop Scand 65(3):287–294. https://doi.org/10.3109/17453679408995455
Douša P, Čech O, Weissinger M, Džupa V (2013) Trochanteric femoral fractures. Acta Chir Orthop Traumatol Cech 80(1):15–26
Frisch NB, Wessell N, Charters M et al (2018) Hip fracture mortality: differences between intertrochanteric and femoral neck fractures. J Surg Orthop Adv Spring 27(1):64–71 (PMID: 29762119)
Huff S, Henningsen J, Schneider A, Hijji F, Froehle A, Krishnamurthy A (2022) Differences between intertrochanteric and femoral neck fractures in resuscitative status and mortality rates. Orthop Traumatol Surg Res 108(5):103231. https://doi.org/10.1016/j.otsr.2022.103231
Fox K, Cummings S, Williams E et al (2000) Femoral neck and intertrochanteric fractures have different risk factors: a prospective study. Osteoporos Int 11:1018–1023. https://doi.org/10.1007/s001980070022
Koval K, Aharonoff G, Rokito A, Lyon T, Zuckerman J (1996) Patients with femoral neck and intertrochanteric fractures: are they the same? Clin Orthop Relat Res 330:166–172
Kesmezacar H, Ayhan E, Unlu MC, Seker A, Karaca S (2010) Predictors of mortality in elderly patients with an intertrochanteric or a femoral neck fracture. J Trauma: Inj Infect Crit Care 68(1):153–158. https://doi.org/10.1097/TA.0b013e31819adc50
Cho Y, Lee I, Ha SH et al (2020) Comparison of hip subregion bone mineral density to the type of proximal femur fracture. Arch Osteoporos 15:122. https://doi.org/10.1007/s11657-020-00789-2
Funding
Open Access funding provided by the Qatar National Library. The authors did not receive support from any organization for the submitted work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors have no financial or proprietary interests in any material discussed in this article.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent to participate
Not applicable.
Consent for publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hantouly, A.T., AlBarazanji, A., Al-Juboori, M. et al. Epidemiology of proximal femur fractures in the young population of Qatar. Eur J Orthop Surg Traumatol 34, 21–29 (2024). https://doi.org/10.1007/s00590-023-03664-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-023-03664-1