
Abstract
Introduction
Despite ongoing discussions for the previous few decades, there is still no consensus regarding the optimal surgical technique for acromioclavicular joint instabilities. The purpose of this study was to determine the impact of various implant materials following arthroscopically assisted stabilization of acromioclavicular joint instabilities on tunnel widening and implant migration. We hypothesized an implant-dependent behavior for tunnel widening and implant migration with differences when comparing acute and chronic acromioclavicular joint instabilities.
Methods
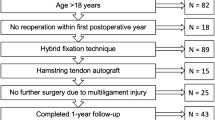
This study compared 105 patients with acromioclavicular joint instabilities that were managed operatively with coracoclavicular double button constructs. Two of the groups containing acute cases were treated with either a double button construct with a wire (TR) or a tape (D) as a central pillar. The two groups with chronic cases were either treated with a wire (T+) or tape D+ as a central pillar and additional hamstring tendon augmentation (+). One central transclavicular–transcoracoidal drill channel was made in the acute cases, while additional medial and lateral drill channels to augment the central pillar with the hamstring tendon were made. The central drill channel in all cases and the medial/lateral drill channels in chronic cases were subsequently radiologically analyzed immediately postoperatively and at follow-up. Following this, additional radiological analysis of the implant migration of the clavicular button took place.
Results
All groups showed significant tunnel widening of the central drill channel at follow-up (p ≤ 0.001). The TR+ technique demonstrated significant widening in both the medial (p ≤ 0.001) and lateral (p ≤ 0.001) drill channels. The D and D+ group displayed significant higher rates of clavicular button migration to a cortical and intraosseous level (p ≤ 0.002).
Conclusion
Tunnel widening and implant migration following arthroscopically assisted management of acromioclavicular joint instabilities are dependent on the chosen implant. The stable tape showed a significantly increased degree of tunnel widening with respect to the central drill channel in comparison with the wire. In contrast, a higher degree of load capacity of the tape ultimately favors a protected intraosseous graft healing for chronic cases, which leads to less tunnel widening of the medial and lateral drill channel. Finally, the D/D+ implant groups showed higher rates of implant migration due to lower contact surface area of the implant at the upper clavicular cortex.
Level of evidence IV.


Similar content being viewed by others

Data availability
The datasets analyzed during the current study are included in the published article as well as they are available from the corresponding author on reasonable request.
References
Mazzocca AD, Arciero RA, Bicos J (2007) Evaluation and treatment of acromioclavicular joint injuries. Am J Sports Med 35:316–329. https://doi.org/10.1177/0363546506298022
Beitzel K, Mazzocca AD, Bak K et al (2014) ISAKOS upper extremity committee consensus statement on the need for diversification of the rockwood classification for acromioclavicular joint injuries. Arthrosc J Arthrosc Relat Surg 30:271–278. https://doi.org/10.1016/j.arthro.2013.11.005
Tuecking LR, Erdle B, Bernstein A et al (2021) Ligamentous healing potential of the acromioclavicular ligament following acute anatomical reconstruction. Arch Orthop Trauma Surg. https://doi.org/10.1007/s00402-021-03936-7
Gowd AK, Liu JN, Cabarcas BC et al (2019) Current concepts in the operative management of acromioclavicular dislocations: a systematic review and meta-analysis of operative techniques. Am J Sports Med 47:2745–2758. https://doi.org/10.1177/0363546518795147
Millett PJ, Horan MP, Warth RJ (2015) Two-year outcomes after primary anatomic coracoclavicular ligament reconstruction. Arthrosc J Arthrosc Relat Surg 31:1962–1973. https://doi.org/10.1016/j.arthro.2015.03.034
Nolte PC, Lacheta L, Dekker TJ et al (2020) Optimal management of acromioclavicular dislocation: current perspectives. Orthop Res Rev 12:27–44. https://doi.org/10.2147/ORR.S218991
Wolf EM, Pennington WT (2001) Arthroscopic reconstruction for acromioclavicular joint dislocation. Arthroscopy. https://doi.org/10.1053/jars.2001.23578
Rosso C, Martetschläger F, Saccomanno MF et al (2021) High degree of consensus achieved regarding diagnosis and treatment of acromioclavicular joint instability among ESA-ESSKA members. Knee Surg Sports Traumatol Arthrosc 29:2325–2332. https://doi.org/10.1007/s00167-020-06286-w
Kraus N, Hann C, Minkus M et al (2019) Primary versus revision arthroscopically-assisted acromio- and coracoclavicular stabilization of chronic AC-joint instability. Arch Orthop Trauma Surg 139:1101–1109. https://doi.org/10.1007/s00402-019-03153-3
Berthold DP, Muench LN, Beitzel K et al (2020) Minimum 10-year outcomes after revision anatomic coracoclavicular ligament reconstruction for acromioclavicular joint instability. Orthop J Sports Med 8:1–7. https://doi.org/10.1177/2325967120947033
Berthold DP, Muench LN, Dyrna F et al (2020) Radiographic alterations in clavicular bone tunnel width following anatomic coracoclavicular ligament reconstruction (ACCR) for chronic acromioclavicular joint injuries. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-020-05980-z
Thangaraju S, Cepni S, Magosch P et al (2019) Arthroscopically assisted acromioclavicular joint stabilization leads to significant clavicular tunnel widening in the early post-operative period. Knee Surg Sports Traumatol Arthrosc 27:3821–3826. https://doi.org/10.1007/s00167-019-05662-5
Scheibel M, Dröschel S, Gerhardt C, Kraus N (2011) Arthroscopically assisted stabilization of acute high-grade acromioclavicular joint separations. Am J Sports Med 39:1507–1516. https://doi.org/10.1177/0363546511399379
Kraus N, Haas NP, Scheibel M, Gerhardt C (2013) Arthroscopically assisted stabilization of acute high-grade acromioclavicular joint separations in a coracoclavicular double-tightrope technique: V-shaped versus parallel drill hole orientation. Arch Orthop Trauma Surg 133:1431–1440. https://doi.org/10.1007/s00402-013-1804-8
Jensen G, Katthagen JC, Alvarado LE et al (2014) Has the arthroscopically assisted reduction of acute AC joint separations with the double tight-rope technique advantages over the clavicular hook plate fixation? Knee Surg Sports Traumatol Arthrosc 22:422–430. https://doi.org/10.1007/s00167-012-2270-5
Martetschläger F, Saier T, Weigert A et al (2016) Effect of coracoid drilling for acromioclavicular joint reconstruction techniques on coracoid fracture risk: a biomechanical study. Arthrosc-J Arthrosc Relat Surg 32:982–987. https://doi.org/10.1016/j.arthro.2015.11.049
Jensen G, Orijit R, Hazra D et al (2022) Arthroscopically assisted single tunnel reconstruction for acute high-grade acromioclavicular joint dislocation with an additional acromioclavicular joint cerclage. Eur J Orthop Surg Traumatol. https://doi.org/10.1007/s00590-022-03271-6
Dey Hazra RO, Hahner F, Ellwein A et al (2019) Additive minimally invasive horizontal cerclage in the arthroscopic treatment of acute higher grade AC joint instabilities. Obere Extremitat 14:292–294. https://doi.org/10.1007/s11678-019-00545-0
Cohen J (1988) Statistical power for the social sciences. Hillsdale NJ: Laurence Erlbaum and Associates
Gignac GE, Szodorai ET (2016) Effect size guidelines for individual differences researchers. Personal Individ Differ. https://doi.org/10.1016/j.paid.2016.06.069
Balke M, Schneider MM, Shafizadeh S et al (2015) Current state of treatment of acute acromioclavicular joint injuries in Germany: is there a difference between specialists and non-specialists? a survey of German trauma and orthopaedic departments. Knee Surg Sports Traumatol Arthrosc 23:1447–1452. https://doi.org/10.1007/s00167-013-2795-2
Martetschläger F, Horan MP, Warth RJ, Millett PJ (2013) Complications after anatomic fixation and reconstruction of the coracoclavicular ligaments. Am J Sports Med. https://doi.org/10.1177/0363546513502459
Cook JB, Shaha JS, Rowles DJ et al (2012) Early failures with single clavicular transosseous coracoclavicular ligament reconstruction. J Shoulder Elbow Surg. https://doi.org/10.1016/j.jse.2012.01.018
Kippe MA, Demetropoulos CK, Baker KC et al (2009) Failure of coracoclavicular artificial graft reconstructions from repetitive rotation. Arthrosc J Arthrosc Relat Surg. https://doi.org/10.1016/j.arthro.2009.03.016
Yoo JC, Choi NH, Kim SY, Lim TK (2006) Distal clavicle tunnel widening after coracoclavicular ligament reconstruction with semitendinous tendon: a case report. J Shoulder Elbow Surg. https://doi.org/10.1016/j.jse.2005.02.019
Schliemann B, Roßlenbroich SB, Schneider KN et al (2015) Why does minimally invasive coracoclavicular ligament reconstruction using a flip button repair technique fail? an analysis of risk factors and complications. Knee Surg Sports Traumatol Arthrosc 23:1419–1425. https://doi.org/10.1007/s00167-013-2737-z
Acknowledgements
The authors thank Mr. Robert Maximilian Blach for his organizational and language support.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
RDH was leading the project; principal investigator, data collection and was responsible for writing the manuscript, HEB was the second principal investigator and contributed to the writing of the manuscript, AE was responsible for project management, MH was responsible for project management and data collection, MW was responsible for project management and data collection, BWF was responsible for language edititng and project management, HL was responsible for surgical intervention, participated in the design and conduct of the trial and contributed to the project management, GJ was responsible for project management and contributed to the writing of the manuscript. All authors have revised the manuscript critically for important intellectual content and approved the final version.
Corresponding author
Ethics declarations
Conflict of interest
H. Lill is consultant with Arthrex (Naples, USA) and DePuy Synthes (Umkirch, Deutschland). R-O Dey Hazra, H. El Bajjati, A. Ellwein, Brad W Fossum, M. Hanhoff and G. Jensen state that there are no conflicts of interest.
Ethical approval
This study was carried out after consulting with the local institutional ethics committee (Medizinische Hochschule Hannover) and is in accordance with the national legal requirements. All procedures that were performed complied with the ethical standards of the institutional and/or national research committee, as well as with the 1975 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent to participate
Informed consent was obtained from all patients prior to their participation in this study.
Consent to publish
Though all patient information is blinded, in this retrospective study, all participants gave their written informed consent to publish the obtained data of the current study.
Informed consent
Informed consent was obtained from all patients prior to their participation in this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Dey Hazra, RO., El Bajjati, H., Hanhoff, M. et al. Implant-dependent behavior of tunnel widening and clavicular button migration after arthroscopic-assisted treatment of acromioclavicular joint instabilities. Eur J Orthop Surg Traumatol 33, 2533–2540 (2023). https://doi.org/10.1007/s00590-022-03466-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-022-03466-x