
Abstract
Introduction
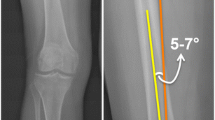
Currently, the best and simplest way that used to select the distal femoral valgus cut (DFVC) angle in total knee arthroplasty (TKA) is standing long leg radiograph. However, this kind of film is still not available in all hospitals. The purpose of this study is to compare the accuracy of different empirical DFVC angles in the restoration of the neutral mechanical alignment of the femoral component after TKA.
Method
125 patients who diagnosed primary osteoarthritic knee and underwent unilateral TKA were randomly assigned into three groups: A, B, and C, according to the use of an intramedullary guide with the DFVC angle of 4°, 5°, and 6°, respectively. At three months after surgery, anteroposterior hip-to-ankle computed tomography (CT) scanograms were evaluated. Mechanical axis angle (MAA), mechanical lateral distal femoral angle (LDFA), femoral bowing, femoral neck-shaft angle (FNSA), and outliers of femoral component position were measured and compared among three groups. Independent influencing factors for the outliers > ±3° were determined using binary logistic regression analysis.
Results
Group B was older than group A. There were no significant differences of postoperative MAA, LDFA, femoral bowing, and FNSA among three groups. Outliers > ±3° of femoral component position in each group were 14.6%, 19.0%, and 16.7%, respectively (p = 0.865). When considering the outliers > ±2°, group C (35.7%) had a trend to have fewer outliers than groups A and B (41.5 and 42.9%). However, this finding was not reached the statistical significance (p = 0.778). Femoral bowing was only significantly influencing factors that related to the outliers > ±3° (p = 0.003).
Conclusion
This study demonstrates that there are no significant differences in coronal femoral component alignment among using the DFVC angle of 4°, 5°, and 6°. The use of the DFVC angle of 6° had a trend to reduce the outliers. Nevertheless, femoral bowing is the crucial influencing factor for selecting the degree of DFVC angle.





Similar content being viewed by others


References
Ritter MA, Faris PM, Keating EM, Meding JB (1994) Postoperative alignment of total knee replacement. Its effect on survival. Clin Orthop 299:153–156
Insall JN (ed) (1984) The total knee replacement. In: Surgery of the knee. Churchill Livingstone, New York, pp 1447–64
Alcelik I, Blomfield M, Öztürk C, Soni A, Charity R, Acornley A (2017) A comparison of short term radiological alignment outcomes of the patient-specific and standard instrumentation for primary total knee arthroplasty: a systematic review and meta-analysis. Acta Orthop Traumatol Turc 51(3):215–222
Nam D, Vajapey S, Haynes JA, Barrack RL, Nunley RM (2016) Does use of a variable distal femur resection angle improve radiographic alignment in primary total knee arthroplasty? J Arthroplast 31(9 Suppl):91–96
Reed SC, Gollish J (1997) The accuracy of femoral intramedullary guides in total knee arthroplasty. J Arthroplast 12(6):677–682
Mullaji AB, Marawar SV, Mittal V (2009) A comparison of coronal plane axial femoral relationships in Asian patients with varus osteoarthritic knees and healthy knees. J Arthroplast 24(6):861–867
Drexler M, Abolghasemian M, Barbuto R, Naini MS, Voshmeh N, Rutenberg TF et al (2017) Patient’s height and hip medial offset are the main determinants of the valgus cut angle during total knee arthroplasty. J Arthroplast 32(5):1496–1501
Canale ST, Beaty JH (2008) Campbell’s operative orthopaedics, 11th edn. Elsevier Inc., Philadelphia
Mullaji AB, Shetty GM, Kanna R, Vadapalli RC (2013) The influence of preoperative deformity on valgus correction angle: an analysis of 503 total knee arthroplasties. J Arthroplast 28(1):20–27
McGrory JE, Trousdale RT, Pagnano MW, Nigbur M (2002) Preoperative hip to ankle radiographs in total knee arthroplasty. Clin Orthop 404:196–202
Whiteside LA, Arima J (1995) The anteroposterior axis for femoral rotational alignment in valgus total knee arthroplasty. Clin Orthop 321:168–172
Wangroongsub Y, Cherdtaweesup S (2009) Proper entry point for femoral intramedullary guide in total knee arthroplasty. J Med Assoc Thail Chotmaihet Thangphaet 92(Suppl 6):S1-5
Victor J, Dujardin J, Vandenneucker H, Arnout N, Bellemans J (2014) Patient-specific guides do not improve accuracy in total knee arthroplasty: a prospective randomized controlled trial. Clin Orthop 472(1):263–271
Deakin AH, Basanagoudar PL, Nunag P, Johnston AT, Sarungi M (2012) Natural distribution of the femoral mechanical–anatomical angle in an osteoarthritic population and its relevance to total knee arthroplasty. Knee 19(2):120–123
Lee C-Y, Huang T-W, Peng K-T, Lee MS, Hsu RW-W, Shen W-J (2015) Variability of distal femoral valgus resection angle in patients with end-stage osteoarthritis and genu varum deformity: radiographic study in an ethnic Asian population. Biomed J 38(4):350–355
Andrews SN, Beeler DM, Parke EA, Nakasone CK, Stickley CD (2018) Fixed distal femoral cut of 6° valgus in total knee arthroplasty: a radiographic review of 788 consecutive cases. J Arthroplast
Kobayashi H, Akamatsu Y, Kumagai K, Kusayama Y, Aratake M, Saito T (2017) Influence of coronal bowing on the lower alignment and the positioning of component in navigation and conventional total knee arthroplasty. Orthop Traumatol Surg Res OTSR 103(2):251–256
Lasam MPG, Lee KJ, Chang CB, Kang YG, Kim TK (2013) Femoral lateral bowing and varus condylar orientation are prevalent and affect axial alignment of TKA in Koreans. Clin Orthop 471(5):1472–1483
Yau WP, Chiu KY, Tang WM, Ng TP (2007) Coronal bowing of the femur and tibia in Chinese: its incidence and effects on total knee arthroplasty planning. J Orthop Surg Hong Kong 15(1):32–36
Kim J-M, Hong S-H, Kim J-M, Lee B-S, Kim D-E, Kim K-A et al (2015) Femoral shaft bowing in the coronal plane has more significant effect on the coronal alignment of TKA than proximal or distal variations of femoral shape. Knee Surg Sports Traumatol Arthrosc Off J ESSKA 23(7):1936–1942
Stucinskas J, Robertsson O, Lebedev A, Wingstrand H, Smailys A, Tarasevicius S (2016) Measuring long radiographs affects the positioning of femoral components in total knee arthroplasty: a randomized controlled trial. Arch Orthop Trauma Surg 136(5):693–700
Acknowledgements
The authors acknowledge the assistance given by Nichakorn Khomawut with data collection. We also acknowledge Suthipol Udompunthurak, MSc. (Applied Statistics), for his assistance with the statistical analyses.
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study included human participants. It had been approved by Siriraj Institutional Review Board (SIRB).
Informed consent
Since this study was a retrospective chart review. Informed consent was obtained by phone from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Pornrattanamaneewong, C., Ruangsomboon, P., Wingprawat, K. et al. Accuracy of empirical distal femoral valgus cut angle of 4° to 6° in total knee arthroplasty: a randomized controlled trial. Eur J Orthop Surg Traumatol 32, 175–181 (2022). https://doi.org/10.1007/s00590-021-02890-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-021-02890-9