
Abstract
Purpose
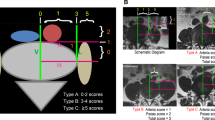
The primary aim was to measure the safe corridor (SC), surgical incision anterior margin (AM), and posterior margin (PM) for OLIF bilaterally from L1 to L5. The secondary aim was to determine the feasibility of approach via the SC. The tertiary aim was to analyze the influence of demographic and anthropometric factors on OLIF parameters.
Methods
We performed a radiographic analysis of 100 subjects who received an abdominal CT. Measurements of the AM, PM, and SC were obtained as well as patient age, sex, height, weight, and BMI. The intraclass correlation coefficient was used to evaluate interrater reliability. To assess associations among variables, Pearson’s correlation tests and multivariate linear regression models were constructed. Sex differences were analyzed using Student’s t tests.
Results
At L1-2, L2-3, L3-4, and L4-5, the PM was 6.6, 8.2, 9.4, and 10.2 cm on the left side and 7.2, 7.7, 8.8, and 9.5 cm on the right side in relation to the disk space center. The SC was less than 1 cm 1%, 3%,3%, and 18% of the time on the left side, and 15%, 12%,29%, and 60% on the right side. None of the anthropometric factors demonstrated a strong correlation with incision location. SC was larger on the left side. Interrater ICC was .934.
Conclusions
This study is the first to provide guidelines on the appropriate location of the incision line during OLIF based on SC from L1 to L5. SC measurements do not vary by sex. OLIF is more feasible via a left-sided approach.

Similar content being viewed by others


Availability of data and material
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Wang K, Zhang C, Wu H, Chen Z, Chou D, Jian F (2019) The anatomic characteristics of the retroperitoneal oblique corridor to the L1–S1 intervertebral disc spaces. Spine 44(12):E697–E706
Kanemura T, Satake K, Nakashima H et al (2017) Understanding retroperitoneal anatomy for lateral approach spine surgery. Spine Surg Relat Res 1(3):107–120
Quillo-Olvera J, Lin GX, Jo HJ, Kim JS (2018) Complications on minimally invasive oblique lumbar interbody fusion at L2–L5 levels: a review of the literature and surgical strategies. Ann Transl Med 6(6):101
Xiao L, Xu Z, Liu C, Zhao Q, Zhang Y, Xu H (2019) Anatomic relationship between ureter and oblique lateral interbody fusion access: analysis based on contrast-enhanced computed tomographic urography. World Neurosurg 123:e717–e722. https://doi.org/10.1016/j.wneu.2018.12.011
Julian Li JX, Mobbs RJ, Phan K (2018) Morphometric MRI imaging study of the corridor for the oblique lumbar interbody fusion technique at L1–L5. World Neurosurg 111:e678–e685. https://doi.org/10.1016/j.wneu.2017.12.136
Fujibayashi S, Otsuki B, Kimura H, Tanida S, Masamoto K, Matsuda S (2017) Preoperative assessment of the ureter with dual-phase contrast-enhanced computed tomography for lateral lumbar interbody fusion procedures. J Orthop Sci 22(3):420–424. https://doi.org/10.1016/j.jos.2017.01.009
Wang H, Zhang Y, Ma X, Xia X, Lu F, Jiang J (2018) Radiographic study of lumbar sympathetic trunk in oblique lateral interbody fusion surgery. World Neurosurg 116:e380–e385. https://doi.org/10.1016/j.wneu.2018.04.212
Wu T, Xiao L, Liu C, Tao X, Xu H (2020) Anatomical study of the lumbar segmental arteries in relation to the oblique lateral interbody fusion approach. World Neurosurg 138:e778–e786. https://doi.org/10.1016/j.wneu.2020.03.080
Chen X, Chen J, Zhang F (2019) Imaging anatomic research of oblique lumbar interbody fusion in a chinese population based on magnetic resonance. World Neurosurg 128:e51–e58. https://doi.org/10.1016/j.wneu.2019.03.244
Liu L, Liang Y, Zhang H et al (2016) Imaging anatomical research on the operative windows of oblique lumbar interbody fusion. PLoS ONE 11(9):e0163452. https://doi.org/10.1371/journal.pone.0163452
Parra-Frutos I (2013) Testing homogeneity of variances with unequal sample sizes. Comput Stat 28(3):1269–1297. https://doi.org/10.1007/s00180-012-0353-x
Vetter TR (2017) Fundamentals of research data and variables: the devil is in the details. Anesth Analg 125(4):1375–1380. https://doi.org/10.1213/ANE.0000000000002370
Vetter TR (2017) Descriptive statistics: reporting the answers to the 5 basic questions of Who, What, Why, When, Where, and a sixth, so What? Anesth Analg 125(5):1797–1802. https://doi.org/10.1213/ANE.0000000000002471
Ratner B (2009) The correlation coefficient: Its values range between +1/−1, or do they? J Target Meas Anal Mark 17(2):139–142. https://doi.org/10.1057/jt.2009.5
Fleiss J (2011) Design and analysis of clinical experiments. Vol 73. Wiley
Shrout PE, Fleiss JL (1979) Intraclass correlations: uses in assessing rater reliability. Psychol Bull 86(2):420–428. https://doi.org/10.1037//0033-2909.86.2.420
Koo TK, Li MY (2016) A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med 15(2):155–163. https://doi.org/10.1016/j.jcm.2016.02.012
Molinares DM, Davis TT, Fung DA (2016) Retroperitoneal oblique corridor to the L2–S1 intervertebral discs: an MRI study. J Neurosurg Spine 24(2):248–255. https://doi.org/10.3171/2015.3.SPINE13976
Boghani Z, Steele WI, Barber SM et al (2020) Variability in the size of the retroperitoneal oblique corridor: a magnetic resonance imaging-based analysis. Surg Neurol Int 11:54. https://doi.org/10.25259/SNI_438_2019
Wu AM, Tian NF, Wu LJ et al (2013) A radiological and cadaveric study of oblique lumbar interbody fixation in patients with normal spinal anatomy. B Jt J 95-B(7):977–982. https://doi.org/10.1302/0301-620X.95B7.31393
Davis TT, Hynes RA, Fung DA et al (2014) Retroperitoneal oblique corridor to the L2–S1 intervertebral discs in the lateral position: an anatomic study. J Neurosurg Spine 21(5):785–793. https://doi.org/10.3171/2014.7.SPINE13564
Deng D, Liao X, Wu R et al (2022) Surgical safe zones for oblique lumbar interbody fusion of L1–5: a cadaveric study. Clin Anat 35(2):178–185. https://doi.org/10.1002/ca.23804
Zhang F, Xu H, Yin B et al (2017) Does right lateral decubitus position change retroperitoneal oblique corridor? A radiographic evaluation from L1 to L5. Eur Spine J 26(3):646–650. https://doi.org/10.1007/s00586-016-4645-7
Berry CA (2019) Oblique lumbar interbody fusion in patient with persistent left-sided inferior vena cava: case report and review of literature. World Neurosurg 132:58–62. https://doi.org/10.1016/j.wneu.2019.08.176
Yang F, Dou C, Cheng X, Chen B (2021) Oblique lateral interbody fusion to treat lumbar spinal stenosis in a patient with situs inversus totalis: a case report. J Int Med Res 49(7):3000605211032809. https://doi.org/10.1177/03000605211032809
Acknowledgements
We would like to thank Elisabeth Clarke for her continual support of our work at the Department of Orthopedic Surgery at Loma Linda University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors received no financial support for the research, authorship, or publication of this article. The authors have no personal, financial, or institutional interest in this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Razzouk, J., Ramos, O., Mehta, S. et al. CT-based analysis of oblique lateral interbody fusion from L1 to L5: location of incision, feasibility of safe corridor approach, and influencing factors. Eur Spine J 32, 1947–1952 (2023). https://doi.org/10.1007/s00586-023-07555-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-023-07555-1