
Abstract
Purpose
To compare the long-term clinical results and complications of two revision strategies for patients with failed total disc replacements (TDRs).
Methods
In 19 patients, the TDR was removed and the intervertebral defect was filled with a femoral head bone strut graft. In addition, instrumented posterolateral fusion was performed (removal group). In 36 patients, only a posterolateral instrumented fusion was performed (fusion group). Visual Analogue Scale (VAS) for pain and Oswestry Disability Index (ODI) were completed pre- and post-revision surgery. Intra- and post-operative complications of both revision strategies were assessed.
Results
The median follow-up was 12.3 years (range 5.3–24.3). In both the removal and fusion groups, a similar (p = 0.515 and p = 0419, respectively) but significant decrease in VAS (p = 0.001 and p = 0.001, respectively) and ODI score (p = 0.033 and p = 0.013, respectively) at post-revision surgery compared to pre-revision surgery was seen. A clinically relevant improvement in VAS and ODI score was found in 62.5% and 43.8% in the removal group and in 43.5% and 39.1% in the fusion group (p = 0.242 and p = 0.773, respectively). Removal of the TDR was associated with substantial intra-operative complications such as major vessel bleeding and ureter lesion. The percentage of late re-operations for complications such as pseudarthrosis were comparable for both revision strategies.
Conclusions
Revision of a failed TDR is clinically beneficial in about half of the patients. No clear benefits for additional TDR removal as compared to posterolateral instrumented fusion alone could be identified. In particular, when considering the substantial risks and complications, great caution is warranted with removal of the TDR.
Graphic abstract
These slides can be retrieved under Electronic Supplementary Material.

Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Fusion of a symptomatic lumbar spinal motion segment is still considered the gold standard of operative treatments of patients with degenerative disc disease (DDD) not responding to conservative care [1,2,3,4,5,6,7]. As spinal fusion is associated with side effects such as cranial facet joint violations, loss of segmental motion, pseudarthrosis and symptomatic adjacent level disease [8, 9], total lumbar disc replacement (TDR) has been introduced to avoid those fusion-related side effects. However, TDR may have serious drawbacks [10,11,12], such as subsidence, facet joint degeneration, dislocation or malposition of the implant, requiring surgical revision [13,14,15,16]. According to the literature, 6–14% of patients needed revision fusion surgery after TDR [10, 11, 17,18,19].
There is an ongoing discussion whether revision surgery for failed TDR is beneficial, and if so, what the optimal revision strategy should be [13, 15, 20, 21]. In a previous study within a smaller patient group at midterm follow-up (mean 3.7 years, range 0.7–11.0), patients significantly improved in terms of pain and function after TDR removal combined with posterolateral instrumented fusion, whereas improvement did not appear to be significant after posterolateral fusion alone. However, the VAS and ODI scores were comparable for both groups at both time points [15]. Therefore, the potential benefit of TDR removal in addition to posterolateral fusion was not fully substantiated in this study, especially considering the significant additional risks and complications of this procedure [13,14,15,16, 22, 23].
Up till now, little is known about the long-term effects of posterolateral instrumented fusion combined with TDR removal or fusion alone. The purpose of this study was to compare the long-term clinical results (minimal follow-up of 5 years) and complications of these two revision strategies for patients with a failed SB Charité III TDR.
Materials and methods
Patient selection
The current study was approved by the Medical Ethics Committee (MEC) Z (16-N-22) and registered at the Dutch Trial Registry (NTR5710). The medical records of all patients who had undergone a TDR by a single surgeon using a SB Charité III between 1989 and 2003 were reviewed. After evaluation, in 63 patients one or more revision spinal fusion operations had been performed at the Zuyderland Medical Center in Sittard or at the Maastricht University Medical Center in Maastricht, between 1991 and 2014. Informed consent was acquired in all patients. Indications for revision were recurrent back and/or leg pain with failure of appropriate conservative measures and the presence of a TDR-related pathology such as facet joint degeneration, adjacent disc disease, malposition or subsidence as determined by plain radiographs, CT scan, MRI and/or facet blocks (Table 1).
Clinical outcome measurements
The clinical evaluation included a Visual Analogue Scale (VAS) for pain (0–100 points) and the Oswestry Disability Index (ODI) for function (0–100 points). Minimally clinically important difference (MCID) was defined as at least 25% improvement [2, 15, 21], or a minimal reduction of 20 points [24] in VAS score between pre- and post-revision surgery [2, 15, 21]. For the ODI score, a minimal reduction of 12.8 points was applied [24].
Statistical analysis
Patient characteristics at the time of revision were summarized using mean and standard deviation (SD) or count and percentage for categorical variables. Continuous outcome parameters were described using mean and standard error of the mean (SEM). The independent and paired sample t tests were used to test for a difference in mean. Differences in the distribution of categorical variables were tested using the Chi-squared test. A multivariable logistic regression model was utilized to identify independent risk factors associated with an insufficient MCID (applied for both definitions) in VAS or ODI score at the latest follow-up compared to pre-revision surgery. p values < 0.05 were considered statistically significant.
Results
In total, 63 patients were included. In 25 patients, the TDR was removed, and after removal of periprosthetic fibrous tissue and sclerotic bone, the intervertebral defect was filled with a femoral head bone strut graft. In addition, an instrumented posterolateral fusion was performed (removal group). In the other 38 patients, posterolateral instrumented fusion alone without TDR removal was performed (fusion group). The type of revision procedure was chosen according to the patient’s preference after a detailed explanation of the potential benefits and risks. The exception in this matter was malposition or migration of the TDR. In all these patients (n = 6), the TDR was removed. The presence of heterotopic ossification (HO) did not influence this decision [25]. Patients with complaints attributed to ASD were only included when spinal fusion of both the index and the affected adjacent segment was performed (n = 8). The surgical technique of both surgeries (Fig. 1) has been described in detail by de Maat et al. [14].

Example case before and after revision of the TDR by posterolateral instrumented spinal fusion and after second-stage removal of the TDR
For all 63 patients, intra- and post-operative complications were assessed. At a minimum of 5-year follow-up, 8 patients (12.7%) were lost to follow-up. The median follow-up after revision surgery (n = 55) was 12.3 years (range 5.3–24.3 years). This was 10.0 years (range 5.3–21.3 years) in the removal group (n = 19) and 14.3 years (n = 36, range 5.7–24.3 years) in the fusion group (p = 0.008). In 16 patients (25.4%), pre-revision clinical evaluation was not available (3 patients in the removal and 13 in the fusion group). An overview of the included patients is shown in Fig. 2. Because of persisting pain, in 8 patients within the fusion group (22.2%), TDR removal was performed as a second-stage revision surgery. In 6 out of these 8 patients, data were available before and after fusion (stage 1) and after removal of the TDR (stage 2).

Overview of the included patients
There were no significant differences for the baseline characteristics with respect to gender, age at insertion of the TDR, body mass index (BMI), surgical levels or number of operated levels between the two groups (Table 1). Significantly more patients had facet joint degeneration in the fusion group (p = 0.004), whereas more patients with either ASD or subsidence were in the removal group (p = 0.072 and p = 0.093).
VAS scores
The mean ± SEM pre-revision VAS score was 79.7 ± 1.48 in the removal and 77.5 ± 2.31 in the fusion group (p = 0.481). Post-revision VAS scores were 54.3 ± 5.93 and 57.4 ± 5.65 in the removal and fusion group, respectively (p = 0.712). In both the removal and the fusion groups, a similar (p = 0.515) but significant decrease in VAS score (p = 0.001 and p = 0.001, respectively) at post-revision surgery compared to pre-revision surgery was seen (Fig. 3a).

a Mean VAS scores for both groups pre- and post-revision surgery. b Mean Oswestry Disability Index for both groups during pre- and post-revision surgery. The error bars represent standard error of the mean
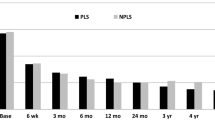
The percentage of improvement after revision surgery in both groups is shown in Fig. 4a. When a minimal improvement of 25% is warranted, 10 out of 16 patients (62.5%) in the removal group and 10 out of 23 patients (43.5%) in the fusion group showed a clinically relevant improvement (p = 0.242). If a minimal reduction of 20 points is applied, 9 out of 16 patients (56.3%) in the removal and 11 out of 23 patients (47.8%) in the fusion group improved (p = 0.987).

a Box plot with a percentage change in VAS score in both revision strategy groups during pre- and post-revision surgery, b percentage change in ODI score in both revision strategy groups during pre- and post-revision surgery. The line represents a clinical success rate of 25%. The error bars represent the upper and lower quartiles
We considered the variables provided in Table 1 as potential risk factors for a lack of improvement in VAS score. These variables were included in a multivariable logistic regression model. Level L2–L3 and level L3–L4 had to be omitted because of too few events to reliably estimate the odds ratio (OR). None of the potential risk factors (including indications for revision surgery) were associated with a lack of clinically relevant improvement in VAS score.
Oswestry Disability Index
The mean ± SEM pre-revision surgery ODI score was 52.9 ± 3.87 in the removal and 55.0 ± 3.85 in the fusion group (p = 0.707). Post-revision ODI scores were 40.0 ± 5.89 and 46.9 ± 3.79 in the removal and fusion group, respectively (p = 0.309). In both the removal and the fusion groups, a similar (p = 0.419) but significant decrease in ODI score (p = 0.033 and p = 0.013, respectively) at post-revision surgery compared to pre-revision surgery was seen (Fig. 3b).
The percentage of improvement after revision surgery in both groups is shown in Fig. 4b. A clinically relevant improvement of 25% was present in 7 out of 16 patients (43.8%) in the removal and in 9 out of 23 patients (39.1%) in the fusion group (p = 0.773). If a minimal reduction of 12.8 points is applied, 7 out of 16 patients (43.8%) in the removal and 10 out of 23 patients in the fusion group (43.5%) improved (p = 0.411). When the above-mentioned multivariable logistic regression model is applied, none of the potential risk factors were statistically significantly associated with a lack of clinically relevant improvement in ODI score.
Second-stage revision surgery
In the fusion group, the eight patients with persisting symptoms underwent TDR removal as a second-stage revision surgery after a median time of 3.3 years (range 1.2–4.4 years). After their second-stage revision surgery, a median follow-up of 7.4 years (range 1.4–11.4 years) was available. A difference in mean VAS score of 14.6 ± 4.11 was seen post-revision surgery (stage 1), between the patients who underwent TDR removal at a later time point and those who did not (p = 0.880). There was not a clear difference for the mean ODI score (2.5 ± 3.49, p = 0.760).
Patients who underwent removal of the TDR as a second-stage revision surgery had a slight but not substantial decrease in their VAS scores (11.6 ± 7.20, p = 0.396) and virtually no decrease in their mean ODI scores (2.3 ± 5.1, p = 0.512) at the latest follow-up. Only in two out of 6 patients (33.3%), an MCID (both definitions) was achieved for both the VAS and ODI scores.
Complications
An overview of the complications for both revision procedures is shown in Table 2. One or more intra- or direct post-operative complications were reported in 7 patients (63.6%) in the removal group and in 4 patients (36.4%) in the fusion group (p = 0.097) with a median time till complication of 0.16 months (range 0–12.1 months).
Intra-operatively, no complications were seen in the fusion group. In the removal group, one patient (4.0%) sustained a small colon lesion, and three patients (12.0%) had a major vessel bleeding (estimated blood loss > 1500 cc). One of these patients sustained a lesion of the ureter as well, which necessitated resection of the left kidney at a second stage. In another patient with a major vessel bleeding, a lung embolus was diagnosed post-operatively. In one patient (4.0%), TDR removal was planned; however, due to an intra-operative rupture of the small intestine, this procedure was abandoned and only posterior fusion was performed. This patient was thus included in the fusion group for further analysis.
Post-operatively, in one patient (2.6%) in the fusion group a malposition of a pedicle screw was diagnosed, which was revised at a second stage. In both groups (2 or 8.0% in the removal and 3 or 7.9% in the fusion group), deep surgical site infection of the dorsal wound, warranting debridement and lavage, was observed.
In six patients (24.0%) in the removal and eleven patients (28.9%) in the fusion group (p = 0.558), a reoperation for persisting symptoms of low back pain was performed with a median time of 70.1 months (range 10.3–164.8) after revision. In both the removal (n = 5, 20.0%) and the fusion groups (n = 7, 18.4%), pseudarthrosis occurred, necessitating revision posterior spinal fusion. In the removal group, one patient (4.0%) developed a junctional kyphosis; in the fusion group, four patients (10.5%) developed adjacent segment disease. Both groups were treated with elongation of the levels previously fused.
Discussion
This study reports the long-term clinical results of two revision strategies for failed TDR with a minimal follow-up of 5 years (median of 12.3 years). Both revision strategies showed clinical improvement, with no additional benefits of removing the TDR in combination with anterior interbody fusion, as compared to posterolateral instrumented spinal fusion alone.
In a previous study within a smaller patient group at mean follow-up of 3.7 years (range 0.7–11 years), we reported a small benefit of TDR removal in terms of improvement in mean VAS and ODI scores [15]. However, in the current study mean VAS and ODI scores were comparable for the removal and fusion groups at both time points. Furthermore, the VAS and ODI score significantly improved in both groups compared to pre-revision surgery. Based on these results, there was no clear benefit from the removal of the TDR.
An MCID was found in 56.3–62.5% in the removal and in 43.5–47.8% in the fusion group for pain (VAS score) and 43.8% and 39.1–43.5%, respectively, for functionality (ODI score). Although not statistically significant, MCID seemed slightly better in the removal group. These differences are, however, less pronounced than previously reported [15]. Unfortunately, we did not obtain psychological testing, so we were not able to study the psychological profile in relation to clinical outcome. The results of additional TDR removal, as a second-stage procedure, because of persisting complaints after posterolateral fusion were disappointing in most patients.
In the ongoing discussion about the optimal revision strategy for failed TDRs, it is suggested that in the case of an intact implant in an acceptable position, posterior fusion can be addressed for the treatment of recurrent back pain presumably caused by facet joint degeneration. When the TDR has subsided or mechanically failed, TDR removal could be considered [15]. However, in the current study, patients with subsidence of the TDR were treated in both groups and no significant changes in terms of VAS and ODI scores were seen at the latest follow-up.
In a previous study by Punt et al., the periprosthetic fibrous tissues of 16 consecutive patients with TDR removal were investigated [26]. Results of that study demonstrated the presence of polyethylene wear particles and of periprosthetic inflammatory reactions around a failed TDR in 15 out of 16 patients. These findings were consistent with other studies [27, 28]. It was therefore hypothesized that TDR removal might reduce back and leg pain in failed TDRs because the source of wear debris generation is removed, which may diminish inflammatory mediated pain. However, in terms of both VAS and ODI scores, no additional benefits of removing the TDR were seen in this study.
An important point to consider is that removal of the TDR was associated with substantial intra-operative complications. This is consistent with other studies reporting considerable iatrogenic injury during revision exposure [13,14,15,16, 22, 23]. Moreover, the percentage of late re-operations (median 70.1 months) for complications such as pseudarthrosis were comparable for both groups.
The current study was limited by its retrospective nature and the fact that patients were not randomized, but the type of revision procedure was chosen according to the surgeon’s and the patient’s preference. The number of patients included in any study has a vital influence on the outcome and whether a study is representative or not. We included a total of 55 patients with a minimal follow-up of 5 years. Only 8 patients (12.8%) were lost to follow-up. This study on revision surgery after TDR reports on the largest number of patients and with the longest follow-up available in the literature.
In conclusion, revision of a failed TDR is clinically beneficial in about half of the patients. No clear benefit from additional TDR removal as compared to posterolateral instrumented fusion alone could be identified. In particular, when considering the substantial risks and complications, great caution is warranted with removal of the TDR.
References
Berg S et al (2009) Total disc replacement compared to lumbar fusion: a randomised controlled trial with 2-year follow-up. Eur Spine J 18(10):1512–1519
Blumenthal S et al (2005) A prospective, randomized, multicenter Food and Drug Administration investigational device exemptions study of lumbar total disc replacement with the CHARITE artificial disc versus lumbar fusion: part I: evaluation of clinical outcomes. Spine (Phila Pa 1976) 30(14):1565–1575 (discussion E387–91)
Gornet MF et al (2011) Lumbar disc arthroplasty with Maverick disc versus stand-alone interbody fusion: a prospective, randomized, controlled, multicenter investigational device exemption trial. Spine (Phila Pa 1976) 36(25):E1600–E1611
Guyer RD et al (2009) Prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of lumbar total disc replacement with the CHARITE artificial disc versus lumbar fusion: five-year follow-up. Spine J 9(5):374–386
Zigler J et al (2007) Results of the prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of the ProDisc-L total disc replacement versus circumferential fusion for the treatment of 1-level degenerative disc disease. Spine (Phila Pa 1976) 32(11):1155–1162 (discussion 1163)
Zigler JE, Glenn J, Delamarter RB (2012) Five-year adjacent-level degenerative changes in patients with single-level disease treated using lumbar total disc replacement with ProDisc-L versus circumferential fusion. J Neurosurg Spine 17(6):504–511
Skold C, Tropp H, Berg S (2013) Five-year follow-up of total disc replacement compared to fusion: a randomized controlled trial. Eur Spine J 22(10):2288–2295
Gillet P (2003) The fate of the adjacent motion segments after lumbar fusion. J Spinal Disord Tech 16(4):338–345
Lee CK (1988) Accelerated degeneration of the segment adjacent to a lumbar fusion. Spine (Phila Pa 1976) 13(3):375–377
van den Eerenbeemt KD et al (2010) Total disc replacement surgery for symptomatic degenerative lumbar disc disease: a systematic review of the literature. Eur Spine J 19(8):1262–1280
Jacobs W et al (2012) Total disc replacement for chronic back pain in the presence of disc degeneration. Cochrane Database Syst Rev 9:CD008326
Siepe CJ et al (2010) The fate of facet joint and adjacent level disc degeneration following total lumbar disc replacement: a prospective clinical, X-ray, and magnetic resonance imaging investigation. Spine (Phila Pa 1976) 35(22):1991–2003
Cunningham BW et al (2009) Revision strategies for single- and two-level total disc arthroplasty procedures: A biomechanical perspective. Spine J 9(9):735–743
de Maat GH et al (2009) Removal of the Charite lumbar artificial disc prosthesis: surgical technique. J Spinal Disord Tech 22(5):334–339
Punt I et al (2012) Clinical outcomes of two revision strategies for failed total disc replacements. Eur Spine J 21(12):2558–2564
Punt IM et al (2008) Complications and reoperations of the SB Charite lumbar disc prosthesis: experience in 75 patients. Eur Spine J 17(1):36–43
Lu SB et al (2015) An 11-year minimum follow-up of the Charite III lumbar disc replacement for the treatment of symptomatic degenerative disc disease. Eur Spine J 24(9):2056–2064
Siepe CJ et al (2014) Mid- to long-term results of total lumbar disc replacement: a prospective analysis with 5- to 10-year follow-up. Spine J 14(8):1417–1431
Guyer RD et al (2016) Five-year follow-up of a prospective, randomized trial comparing two lumbar total disc replacements. Spine (Phila Pa 1976) 41(1):3–8
Malham GM, Parker RM (2017) Early experience with lateral lumbar total disc replacement: utility, complications and revision strategies. J Clin Neurosci 39:176–183
Alahmadi H, Deutsch H (2014) Outcome of salvage lumbar fusion after lumbar arthroplasty. Asian Spine J 8(1):13–18
Leary SP et al (2007) Revision and explantation strategies involving the CHARITE lumbar artificial disc replacement. Spine (Phila Pa 1976) 32(9):1001–1011
McAfee PC et al (2006) Revisability of the CHARITE artificial disc replacement: analysis of 688 patients enrolled in the U.S. IDE study of the CHARITE Artificial Disc. Spine (Phila Pa 1976) 31(11):1217–1226
McCormick JD, Werner BC, Shimer AL (2013) Patient-reported outcome measures in spine surgery. J Am Acad Orthop Surg 21(2):99–107
Park HJ et al (2018) Radiological and clinical long-term results of heterotopic ossification following lumbar total disc replacement. Spine J 18(5):762–768
Punt IM et al (2009) Periprosthetic tissue reactions observed at revision of total intervertebral disc arthroplasty. Biomaterials 30(11):2079–2084
Veruva SY et al (2017) Periprosthetic UHMWPE wear debris induces inflammation, vascularization, and innervation after total disc replacement in the lumbar spine. Clin Orthop Relat Res 475(5):1369–1381
Wright TM (2017) CORR insights((R)): periprosthetic UHMWPE wear debris induces inflammation, vascularization, and innervation after total disc replacement in the lumbar spine. Clin Orthop Relat Res 475(5):1382–1385
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Kitzen, J., Vercoulen, T.F.G., van Kuijk, S.M.J. et al. Long-term clinical outcome of two revision strategies for failed total disc replacements. Eur Spine J 29, 1536–1543 (2020). https://doi.org/10.1007/s00586-019-06184-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-019-06184-x