
Abstract
Purpose
To highlight cervical spondylodiscitis as an infrequent complication following an invasive procedure on the neopharynx in patients previously treated with circumferential pharyngolaryngectomy with pectoralis major myocutaneous flap reconstruction.
Methods
Patients diagnosed with cervical spondylodiscitis after circumferential pharyngolaryngectomy between 2001 and 2013 were retrospectively studied using a questionnaire sent to the French head and neck tumour study group. Medical history; tumour management; clinical symptoms; biological, microbiological and imaging results; and management of the infection were collected for each patient.
Results
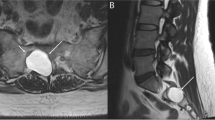
Six men aged 51–66 years were diagnosed with spondylodiscitis on average 5.6 years after circumferential pharyngolaryngectomy, and a mean 2 months following an invasive procedure on the neopharynx (oesophageal dilatation, phonatory prosthesis insertion). The patients presented with cervical pain and increased CRP level. MRI showed epidural abscess and communication between the pharynx and vertebral bodies in most cases. Microbiological samples yielded bacteria from the pharynx flora. Infection was managed using antibiotics adjusted according to the culture results and spinal immobilisation for duration of 6–12 weeks. No surgical treatment was required. During follow-up, no patient experienced recurrence or residual disability.
Conclusions
Cervical spondylodiscitis is a rare but potentially severe complication following an invasive procedure on the neopharynx after circumferential pharyngolaryngectomy. Therefore, the onset of nonspecific symptoms should not be overlooked, and MRI must be performed if infection is suspected. Microbiological confirmation is critical in optimising treatment, which should be aggressive, even if overall prognosis seems to be good.



Similar content being viewed by others


References
Espitalier F, Ferron C, Leux C et al (2012) Results after U-shaped pectoralis major myocutaneous flap reconstruction of circumferential pharyngeal defects. Laryngoscope 122:2677–2682
Bolzoni A, Peretti G, Piazza C et al (2006) Cervical spondylodiscitis: a rare complication after phonatory prosthesis insertion. Head Neck 28:89–93
Shousha M, Heyde C, Boehm H (2015) Cervical spondylodiscitis: change in clinical picture and operative management during the last two decades. A series of 50 patients and review of literature. Eur Spine J 24:571–576
Urrutia J, Zamora T, Campos M (2013) Cervical pyogenic spinal infections: are they more severe diseases than infections in other vertebral locations? Eur Spine J 22:2815–2820
Hadjipavlou AG, Mader JT, Necessary JT et al (2000) Hematogenous pyogenic spinal infections and their surgical management. Spine 25:1668–1679
Stramandinoli E, Ayache S, de la Roche Saint Andre G et al (2001) Cervical spondylodiscitis: a rare complication of phonatory implants. Ann Otolaryngol Chir Cervicofac 118:382–385
Korovessis P, Repantis T, Hadjipavlou AG (2012) Hematogenous pyogenic spinal infection: current perceptions. Orthopedics 35:885–892
Cottle L, Riordan T (2008) Infectious spondylodiscitis. J Infect 56:401–412
McDermott H, Bolger C, Humphreys H (2012) Postprocedural discitis of the vertebral spine: challenges in diagnosis, treatment and prevention. J Hosp Infect 82:152–157
Fabian R (1988) Pectoralis major myocutaneous flap reconstruction of the laryngopharynx and cervical esophagus. Laryngoscope 98:1227–1231
Spriano G, Pellini R, Roselli R (2002) Pectoralis major myocutaneous flap for hypopharyngeal reconstruction. Plast Reconstr Surg 110:1408–1413 (discussion 1414–1416)
SPILF (2007) Primary infectious spondylitis, and following intradiscal procedure without prothesis. Short text. Med Mal Infect 37:554–572
Berbari EF, Kanj SS, Kowalski TJ et al (2015) 2015 Infectious Diseases Society of America (IDSA) clinical practice guidelines for the diagnosis and treatment of native vertebral osteomyelitis in adults. Clin Infect Dis 61:e26–e46
Enoch DA, Cargill JS, Laing R et al (2008) Value of CT-guided biopsy in the diagnosis of septic discitis. J Clin Pathol 61:750–753
McHenry MC, Easley KA, Locker GA (2002) Vertebral osteomyelitis: long-term outcome for 253 patients from 7 Cleveland-area hospitals. Clin Infect Dis 34:1342–1350
Mahalingam S, Srinivasan R, Spielmann P (2016) Quality-of-life and functional outcomes following pharyngolaryngectomy: a systematic review of literature. Clin Otolaryngol 41:25–43
Radulovic D, Vujotic L (2013) Cervical spinal epidural abscess after oesophagoscopy. Eur Spine J 22(Suppl 3):S369–S372
Demont G, Cournac JM, Poisnel E et al (2011) Parvimonas micra iatrogenic cervical spondylodiscitis. Rev Med Interne 32:S329–S330
Holmgaard R, Jakobsen LP (2008) Cervical spondylodiscitis—a rare complication of palatopharyngeal flap surgery. Cleft Palate-Craniofac J 45:674–676
Honda K, Asato R, Tsuji J et al (2013) Pyogenic spondylodiscitis after transoral surgery for oropharyngeal cancer. Auris Nasus Larynx 40:320–322
Curry JM, Cognetti DM, Harrop J et al (2007) Cervical discitis and epidural abscess after tonsillectomy. Laryngoscope 117:2093–2096
Van Ooij A, Manni JJ, Beuls EA et al (1999) Cervical spondylodiscitis after removal of a fishbone. A case report. Spine 24:574–577
Brunet A, Guillemin F, Bichet G et al (1989) Cervical spondylodiscitis. A rare complication of intubation. Ann Otolaryngol Chir Cervicofac 106:40–43
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None declared.
Additional information
A. de Keating-Hart contributed equally to this work.
Rights and permissions
About this article

Cite this article
Espitalier, F., de Keating-Hart, A., Morinière, S. et al. Cervical spondylodiscitis following an invasive procedure on the neopharynx after circumferential pharyngolaryngectomy: a retrospective case series. Eur Spine J 25, 3894–3901 (2016). https://doi.org/10.1007/s00586-016-4741-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-016-4741-8