
Abstract
Purpose
The purpose was to quantify the structural integrity of annulus fibrosis (AF) after injuries with repair.
Methods
Punctures in the AF of 6-month-old porcine spine specimens were made with 18-, 20-, 22-, 24-, and 26-gauge needles. Leakage testing was performed immediately after needle puncture (Group 1), after the puncture was repaired with a modified purse-string suture (MPSS) (Group 2), and after needle puncture with immediate repair (Group 3). Punch injuries repaired with the MPSS alone, or with an AF graft and MPSS were also examined.
Results
There was no leakage from 26-gauge needle punctures. Pressures at which the nucleus pulposus leaked from the 24-, 22-, 20- and 18-gauge needle punctures (Group 1) were 4.28, 2.03, 1.27, and 1.06 MPa, respectively. Failure pressure after repair (Group 2, 3) was significantly greater than without (Group 1). Failure pressure in Group 3 was much greater than in Group 2 with 18- and 20-gauge punctures. Punch injury repaired with a graft and MPSS had significantly greater failure pressure than repair with MPSS alone (1.88 vs. 1.02 MPa, p = 0.0001).
Conclusions
The MPSS can restore the mechanical integrity of the AF after needle puncture. An annular graft along with a MPSS may increase the structural integrity of the AF after a punch injury. As this was an acute animal study, the measurements and results may not directly translate to the human intervertebral disc.
Similar content being viewed by others


Introduction
Degenerative disc disorders are associated with mechanical failure of the annulus fibrosus (AF) as evidenced by the presence of annular tears, fissures, and herniation [1–4]. These small tears coalesce and form radial annular tears allowing the pressurized nucleus pulposus (NP) to extrude through the defect resulting in disc herniation [3].
Symptomatic lumbar disc herniation is often treated by discectomy. A review of the literature indicated a greater incidence of long-term recurrent back and leg pain after aggressive discectomy, but a greater reported incidence of recurrent disc herniation after limited discectomy [5]. Less invasive procedures for the diagnosis and treatment of intervertebral disc (IVD) disease, such as discography, intradiscal electrothermal treatment, growth factor injection, or gene therapy typically require needle puncture to the nucleus through the AF which compromises the mechanical integrity of the disc and can lead to degeneration [2, 6, 7]. Even discography performed with a small gauge needle and limited pressurization can result in accelerated disc degeneration, disc herniation, and loss of disc height [8].
Study using a sheep model has shown that the biomechanical properties of the lumbar disc can be affected by the type of annular incision [9], and change in proportion with the size of a defect [6, 10–12]. Methods of repairing and reinforcing the AF after needle injection or discectomy have been investigated [13]. Suturing of the annular defect may be performed for containment of the NP, but this does not compensate for the loss of annulus material or reverse biomechanical changes [14]. An animal model showed that direct repair of annular incisions does not significantly alter the healing strength of the IVD after lumbar discectomy [15]. We previously reported a new suturing technique, a modified purse-string suture (MPSS), that preserves the competence of the disc and withstands increased stresses after annulotomy [16, 17].
The objective of this study was to determine leakage pressure of the lumbar IVD after a puncture injury of the AF with different sized needles, and puncture and punch injuries repaired with the MPSS technique. Leakage pressure after a punch injury repaired with a graft of AF taken from another disc was also examined. While only a single biomechanical test was performed, use of an AF graft and suture of AF defects is a new idea of dealing with disc problem and we believe this study may provide the basis for future research for the treatment of IVD disease.
Methods
This study was approved by the institutional animal care and use committee of (Blinded). Spines of 6-month-old pigs weighing 80–100 kg were purchased from a slaughterhouse, and 40 motion segments comprising an intervertebral disc and its adjoining two intact vertebrae were isolated. There are six lumbar vertebral bodies in a porcine. Because a complete motion segment was used, the level of removal was L1–L2, L3–L4, L5–L6. The discs were 5 cm in width, 3.5 cm in anteroposterior diameter, and 8 mm in height. The thickness of annulus tissue in anterior portion was 11–12 mm, in the posterior 3–5 mm, and in the lateral 8–9 mm. Before experimentation, all adjacent soft tissues and muscles were removed keeping the anterior/posterior ligaments intact, and the spines were kept in normal saline at 4 °C to ensure a consistent level of pretest hydration.
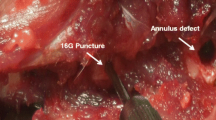
Two types of annular injuries were investigated, annular puncture injury and annular punch injury (Fig. 1).

Experimental flow chart. a Annular puncture injury. Discs underwent leakage testing immediately after puncture injury, and after repair with the modified purse-string suture (MPSS) technique. In another set of punctured discs, annular MPSS repair was performed immediately after the puncture injury. b Annular punch injury. Leakage testing of punch-injured discs was performed after repair with the MPSS alone, and after repair with a graft and the MPSS
Annular puncture injury
For an annular puncture injury, a 26-gauge needle was inserted from the anterolateral side of the disc in each motion segment. A 26-gauge needle was used because when discography is performed 17- to 22-gauge needles are commonly used, and when a double-needle approach is used a 26-gauge needle is used as the inner needle to decrease the size of the puncture hole [18]. Another puncture injury on the opposite side was made by randomly using one of four different diameter needles (18-, 20-, 22-, and 24-gauge). Punctures were 11–12 mm deep, and were assumed to penetrate deep into the NP. Since a needle was used, in theory this should only sever some collagen fibers and not remove AF tissue.
Testing was performed in two ways (Fig. 1). One set (n = 6) of punctured discs underwent leakage testing immediately after the puncture. Internal pressure was applied with an influx of align gel through a stainless steel tube inserted into the IVD and failure pressures were recorded (Group 1). After testing, all punctures were repaired by the MPSS technique (Fig. 2), and another pressure test was performed (Group 2, delayed repair group). In another set of punctured discs (n = 6) annular MPSS repair was performed immediately after the puncture injury, and testing performed (Group 3, instant repair group).

Modified purse-string suture (MPSS). The MPSS technique consists of two loop structures and a cross-over compression suture. The technique provides a near watertight seal of the annular orifice
Annular punch injury
An annular defect of approximately 3 × 4×11 mm was made in the anterolateral aspect of the disc (n = 6; Group 4) with a curved woodcutting knife. Force was applied vertically to the annulus surface, which caused the blade to quickly cut the fibers and controlled the orientation of the injury. Because the blade was curved, 2 punches were able to produce a roughly rhombic defect. The defect was repaired with the MPSS technique, and leakage testing performed.
In another set of discs (n = 6; Group 5), grafts were used to repair the annular defects (Fig. 3). Annulus tissue was harvested from another porcine disc, and cut to 3 × 4×11 mm. The tissue was dehydrated in 75 % alcohol for 30 min, cleaned with alcohol-soaked gauze, then stored in PBS buffer solution. Because the annulus fibrosus is 70 % water and 15 % collagen, alcohol was used to remove water from the annulus. This shrank the volume of the tissue made the graft tissue easily plugged into the defect and facilitated suturing of the tissue. The defect was repaired with the graft and the MPSS technique, and leakage testing performed.

Modified purse-string suture (MPSS) and annular graft. a An annular graft harvested from another porcine disc. b An annular defect of 3 × 4 × 11 mm was created by a punch injury. The defect was closed with a graft and MPSS
Leakage testing
Leakage testing was based on a method previously described [19]. Briefly, the motion segment was fixed in an adjustable harness to prevent the IVD from expanding longitudinally during pressurization. A 0.9 mm stainless steel tube was inserted vertically through one of the attached vertebra and endplate into the nucleus, thus eliminating damage to the annulus (Fig. 4a, b). The tube was connected to a pressure generating system, which consisted of a piston, a stainless steel syringe filled with blue-colored algin gel, and an Instron 4467 servohydraulic testing system (Instron Norwood, MA) (Fig. 4c). Therefore, AF damage is entirely due to the increased pressure within the IVD and that caused by the nucleus tissue and injected colored gel to be expelled.

Porcine lumbar disc and servohydraulic testing system. a Gross appearance of the intervertebral segment. b Sagittal section of the intervertebral segment. The tube was inserted longitudinally through one of the attached vertebra and endplate into the nucleus (red arrow indicates tract of the tube). c Diagram of the Instron 4467 servohydraulic testing system
For testing, the piston was compressed a constant rate of 5 mm/min. Internal pressure was applied to the IVD by gel influx, and the pressure at the initial leakage of algin (failure pressure) from the annular orifice was recorded.
Statistical analysis
Continuous data of rupture pressure were expressed as mean ± standard deviation (SD) for each experimental group. Differences in rupture pressure between two groups were detected by paired t test for dependent samples, and by independent t test for independent samples. Bonferroni correction was applied for type I error adjustment when multiple pairwise comparisons were performed. Statistical analyses were performed with SAS software version 9.2 (SAS Institute Inc., Cary, NC). A 2-tailed p < 0.05 indicated statistical significance.
Results
In Group 1, there was no align leakage from the punctures created by the 26-gauge needle. The pressures at which gel leaked from 24-, 22-, 20-, and 18-gauge needle punctures were 4.28 ± 0.51, 2.03 ± 0.42, 1.27 ± 0.44, and 1.06 ± 0.31 MPa, respectively. After annular repair, the mean failure pressures of Group 2 (delayed repair) were greater than Group 1 (Fig. 5). There were significant differences between Group 2 and Group 1 with 22-, and 20-gauge needle punctures (both, p ≤ 0.05), but not with the 18-gauge needle puncture (p = 0.235).

Comparison of failure pressure of puncture injury alone (Group 1), puncture injury with delayed repair (Group 2), and puncture injury with instant repair (Group 3) with different size (18-, 20-, 22-, and 24- gauge) needle punctures. Data are presented as mean ± SD. *Compared to Group 1, p < 0.05; †Compared to Group 2, p < 0.05 (both, after Bonferroni correction)
In Group 3 (instant repair group), failure pressures were significantly greater than in Group 2 (delayed repair group) with 18-gauge (4.87 ± 0.42 vs. 1.28 ± 0.13 MPa, p < 0.001) and 20-gauge needle punctures (5.65 ± 0.611 vs. 2.48 ± 0.31 MPa, p < 0.05), but not with 22- and 24-gauge punctures. Values were also significantly greater than those in Group 1 with 18-, 20-, 22-, and 24-gauge needle punctures (all, p < 0.001, Fig. 5).
The failure pressures of Group 4 and Group 5 are shown in Fig. 6. Injured discs treated with the annular graft combined with MPSS technique had a significantly greater failure pressure than those treated with the MPSS technique alone (1.88 ± 0.30 vs. 1.02 ± 0.18 MPa, p = 0.0001).

Failure pressure of punch-injured discs treated with a modified purse-string suture (MPSS) alone and with a graft. Data are presented as mean ± standard deviation (SD). *p < 0.05; independent t test
A sagittal section of the intervertebral segment after leakage testing is shown in Fig. 7.

Sagittal section of the intervertebral segment after mechanical testing. An irregular tract of gel leakage from the central nucleus extending through inner annulus to the suture area was noted (red arrow, tract tube; orange arrow, leak tract; black arrow, suture area)
Discussion
The results of this study suggest that there may be a minimum size of needle that can prevent impairment of AF mechanical integrity. The study also showed the MPSS technique can restore the mechanical integrity of the AF after needle puncture, and that an annular graft may improve the structural integrity of the AF.
This study measured AF leakage pressure following injury and repair; there was no direct measure of damage and structural integrity of the IVD, and it was only an acute study without an examination of fatigue or in vivo healing response; the results must be interpreted within this context. A modified quantitative discomanometry technique [19] was used in order not to damage the annulus during the production of hydrostatic pressure. A stainless steel tube was inset into the disc through the vertebral body and influx gel to increase disc internal pressure. With this method the tube is placed in the IVD, and IVD structural damage is entirely due to an increase in pressure in the IVD. Though disc structural integrity was not precisely studied, the cross-sectional diagram of the motion segment in the experiment revealed that the IVD structure suffered damage (Fig. 7), though the damage was not quantified.
While it has been shown that the mechanical properties of a disc change in relationship with the size of annular defect [6, 10–12], and with the depth of needle puncture [20], the minimum size of an annular defect necessary to compromise the functional integrity of a disc has not been determined. Results of the puncture group showed a decrease in rupture pressure from 4.28 to 1.06 MPa after puncture with an increasing needle diameter from 24 gauge (7 % of disc height) to 18 gauge (16 % of disc height). This is consistent with the results of Elliott et al. [6] who found that disc changes depend on the ratio of needle diameter to disc height, and that significant changes were not observed for needle:height ratio less than 40 %, whereas changes were universally present for needle:height ratio over 40 %.
In the normal IVD, the annulus-nucleus-vertebral endplates act as a closed system. IVD herniation can occur due to an annular fissure caused by a natural degeneration process or after damage [2, 7]. A needle puncture through the AF can be considered a man-made annular fissure. Suture can be used to reinforce the mechanical function of the disc after an annular defect, and effective sealing of the defect may slow IVD degenerative processes [16].
The MPSS technique provides a 3-dimensional construction that tightly contracts the defect without leaving a fenestration, withstands a greater pressure than a simple suture, and has been proven to increase annular strength against intradiscal pressure [16, 17]. In the current study, discs with needle punctures and nuclear leakage were shown to have an increase in ability to resist internal hydrostatic pressure after repair with the MPSS technique. Failure pressure was inversely related to the needle diameter with delayed repair, and may be because the inner annulus and interconnections of the lamella are disrupted to a greater extent after leakage of the nuclear material. Interestingly, the failure pressure of puncture injury with instant repair was much greater than that with delayed repair in the 18- and 20-gauge groups. It is possible that damage to interlamellar interconnections in the instant repair group was likely less than in the delayed repair group making the effect of suturing in the larger size needle groups more obvious. The current study, however, did not include a histological study of the annulus after damage/testing to examine these possibilities.
Repair of an AF defect must be able to withstand the normal loading pressures of the IVD. Intradiscal pressure is reported to be around 1 MPa in the normal upright position, and up to 3 MPa for maintaining normal daily loading [21, 22]. The current pressure data showed that an annular defect repaired using the MPSS technique can withstand normal daily loading pressures, and that an annular graft with MPSS provided a significantly greater failure pressure than MPSS alone.
This experiment used annular tissue from another disc to prove the effectiveness of an annular graft. The method is not feasible clinically, but we believe that proof of concept was shown. To use the method clinically, it will be necessary to develop biological annulus material, such as the biological valves taken from porcine, bovine, or human sources used in valvular surgery. It may also be possible to create suitable tissue scaffolds as Ledet et al. [23] have done from the small intestine as a scaffold in closing annular defects. Because annular injuries are typically very small, there are nerves nearby, and the surgical work space is very small, it is extremely difficult to suture annular tears or defects. It will therefore be necessary to design a device to achieve successfully suturing of the annulus.
There are a number of limitations in this study that should be considered. While porcine discs are morphologically similar to human discs [24], the results, including cut-off pressures and minimum puncture size may need more validation test before it applied to the human disc. Only pressure was studied; other mechanical properties such as compressive stiffness, bending compliance, and viscoelastic creep were not examined. Factors such as volume of injected algin, location, direction, and depth of the needle puncture, and wall thickness of the annulus were not analyzed. In addition, various types of annular incisions may be used during discectomy, and annular tears that occur as a result of disc herniation can result in significant destruction of many layers of the AF, and in this study only fresh puncture and punch injuries were examined. This was an acute study, and fatigue and in vivo healing response were not examined.
Conclusions
The results of this acute biomechanical study on porcine IVDs suggest that there may be a minimum size of needle that can prevent impairment of AF mechanical integrity and that the MPSS technique can restore the mechanical integrity of the AF after needle puncture to a degree sufficient to resist normal loading of the spine. An annular graft may improve the structural integrity of the AF. However, current data may be valid for specific animal model on 6-month-old pigs and cannot be transferred to the clinical situations; similarly the MPSS technique will be difficult to transfer into clinical application. Further study of the applicability of the techniques to the human spine may be warranted.
References
Ebara S, Iatridis JC, Setton LA, Foster RJ, Mow VC, Weidenbaum M (1996) Tensile properties of nondegenerate human lumbar anulus fibrosus. Spine (Phila Pa 1976) 21:452–461
Inoue N, Espinoza Orias AA (2011) Biomechanics of intervertebral disk degeneration. Orthop Clin North Am 42:487–499
Kim Y (2000) Prediction of peripheral tears in the anulus of the intervertebral disc. Spine (Phila Pa 1976) 25:1771–1774
Osti OL, Vernon-Roberts B, Fraser RD (1990) 1990 Volvo Award in experimental studies. Anulus tears and intervertebral disc degeneration. An experimental study using an animal model. Spine (Phila Pa 1976) 15:762–767
McGirt MJ, Ambrossi GL, Datoo G, Sciubba DM, Witham TF, Wolinsky JP, Gokaslan ZL, Bydon A (2009) Recurrent disc herniation and long-term back pain after primary lumbar discectomy: review of outcomes reported for limited versus aggressive disc removal. Neurosurgery 64:338–344
Elliott DM, Yerramalli CS, Beckstein JC, Boxberger JI, Johannessen W, Vresilovic EJ (2008) The effect of relative needle diameter in puncture and sham injection animal models of degeneration. Spine (Phila Pa 1976) 33:588–596
Korecki CL, MacLean JJ, Iatridis JC (2007) Characterization of an in vitro intervertebral disc organ culture system. Eur Spine J 16:1029–1037
Carragee EJ, Don AS, Hurwitz EL, Cuellar JM, Carrino JA, Herzog R (2009) 2009 ISSLS prize winner: does discography cause accelerated progression of degeneration changes in the lumbar disc: a ten-year matched cohort study. Spine (Phila Pa 1976) 34:2338–2345
Ahlgren BD, Vasavada A, Brower RS, Lydon C, Herkowitz HN, Panjabi MM (1994) Anular incision technique on the strength and multidirectional flexibility of the healing intervertebral disc. Spine (Phila Pa 1976) 19:948–954
Martin JT, Gorth DJ, Beattie EE, Harfe BD, Smith LJ, Elliott DM (2013) Needle puncture injury causes acute and long-term mechanical deficiency in a mouse model of intervertebral disc degeneration. J Orthop Res 31:1276–1282
Michalek AJ, Iatridis JC (2011) Penetrating annulus fibrosus injuries affect dynamic compressive behaviors of the intervertebral disc via altered fluid flow: an analytical interpretation. J Biomech Eng 133:084502
Michalek AJ, Iatridis JC (2012) Height and torsional stiffness are most sensitive to annular injury in large animal intervertebral discs. Spine J 12:425–432
Wilke HJ, Ressel L, Heuer F, Graf N, Rath S (2013) Can prevention of a reherniation be investigated? Establishment of a herniation model and experiments with an anular closure device. Spine (Phila Pa 1976) 38:E587–E593
Bron JL, Helder MN, Meisel HJ, Van Royen BJ, Smit TH (2009) Repair, regenerative and supportive therapies of the annulus fibrosus: achievements and challenges. Eur Spine J 18:301–313
Ahlgren BD, Lui W, Herkowitz HN, Panjabi MM, Guiboux JP (2000) Effect of anular repair on the healing strength of the intervertebral disc: a sheep model. Spine (Phila Pa 1976) 25:2165–2170
Chiang CJ, Cheng CK, Sun JS, Liao CJ, Wang YH, Tsuang YH (2011) The effect of a new anular repair after discectomy in intervertebral disc degeneration: an experimental study using a porcine spine model. Spine (Phila Pa 1976) 36:761–769
Chiang YF, Chiang CJ, Yang CH, Zhong ZC, Chen CS, Cheng CK, Tsuang YH (2012) Retaining intradiscal pressure after annulotomy by different annular suture techniques, and their biomechanical evaluations. Clin Biomech (Bristol, Avon) 27:241–248
Peh W (2005) Provocative discography: current status. Biomed Imaging Interv J 1:e2
Schechtman H, Robertson PA, Broom ND (2006) Failure strength of the bovine caudal disc under internal hydrostatic pressure. J Biomech 39:1401–1409
Aoki Y, Akeda K, An H, Muehleman C, Takahashi K, Moriya H, Masuda K (2006) Nerve fiber ingrowth into scar tissue formed following nucleus pulposus extrusion in the rabbit anular-puncture disc degeneration model: effects of depth of puncture. Spine (Phila Pa 1976) 31:E774–E780
Wilke HJ, Neef P, Caimi M, Hoogland T, Claes LE (1999) New in vivo measurements of pressures in the intervertebral disc in daily life. Spine (Phila Pa 1976) 24:755–762
Wilke H, Neef P, Hinz B, Seidel H, Claes L (2001) Intradiscal pressure together with anthropometric data–a data set for the validation of models. Clin Biomech (Bristol, Avon) 16(Suppl 1):S111–S126
Ledet EH, Jeshuran W, Glennon JC, Shaffrey C, De Deyne P, Belden C, Kallakury B, Carl AL (2009) Small intestinal submucosa for anular defect closure: long-term response in an in vivo sheep model. Spine (Phila Pa 1976) 34:1457–1463
Callaghan JP, McGill SM (2001) Intervertebral disc herniation: studies on a porcine model exposed to highly repetitive flexion/extension motion with compressive force. Clin Biomech (Bristol, Avon) 16:28–37
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interests
All the authors declare that no competing interests exist.
Financial disclosure
No authors received any specific funding for this work.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Yang, CH., Chiang, YF., Chen, CH. et al. The effect of annular repair on the failure strength of the porcine lumbar disc after needle puncture and punch injury. Eur Spine J 25, 906–912 (2016). https://doi.org/10.1007/s00586-015-4316-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-015-4316-0