
Abstract
Introduction
Cervical subaxial malalignment due to complete or partial post-traumatic dislocation is generally associated to neurological impairment of ranging severity. Literature lacks reporting this entity in patients with no neurological issues. Cervical traction is not widely accepted in treating this kind of injury, due to its potential for neurological damage, although surgery seems to represent the gold standard.
Materials and methods
We studied in detail 18 cervical subaxial severe dislocations and ptosis, especially analyzing 2 personal cases plus 5 from the literature without neurological impairment. We discuss the role of pre-operative cervical traction and its influence on the overall surgical planning and outcome.
Results
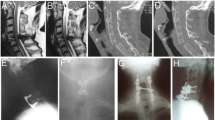
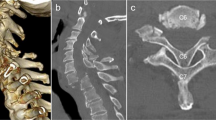
Sixteen cases of anterior complete luxation were described in detail by literature. Five patients were reported having no associated neurological impairment and three were treated by pre-operative traction. Our two cases of cervical subaxial dislocation due to bi-pedicular fractures without neurological deficits were treated by traction and surgical fixation.
Conclusions
Subaxial bi-pedicular fracture is a highly unstable condition of the cervical spine. Complete or incomplete dislocation requires instrumented fixation. An intact neurological status is very rare. Pathological canal enlargement seems to be able to protect the spinal cord, during trauma and/or traction. For these findings, cervical traction could be applied with no excessive worrying. We prefer a progressive traction up to 20 lb, administered in 7–10 days with no intubation and close neuro-vascular status monitoring. Good pre-operative realignment can be properly achieved in the majority of cervical dislocations, thus avoiding three-stage surgery and somatectomy.


Similar content being viewed by others

References
Perlman R, Hawes LE (1951) Cervical spondylolisthesis. J Bone J Surg 33A:1012–1013
Durbin FC (1956) Spondylolisthesis of the cervical spine. J Bone J Surg 38B:734–735
Lee CW, Hwang SC, Im SB et al (2004) Traumatic thoracic spondyloptosis: case report. J Korean Neurosurg Soc 35:622–624
Amacher AL (1993) Cervical spondyloptosis. J Neurosurg 78:853 (letter)
Bellamy R, Liober A, Smith SD (1974) Congenital spondylolisthesis of the sixth cervical vertebra: case report and description of operative findings. J Bone J Surg 56A:405–407
Sheikholeslamzadeh S, Aalami-Harandi B, Fateh H (1977) Spondylolisthesis of the cervical spine. Report of a case. J Bone J Surg 59B:95–96
Wild A, Jager M, Werner A et al (2001) Treatment of congenital spondyloptosis in a 18-month-old patient with a 10-year follow-up. Spine 26:502–505
Muzumdar DP, Goel A (2004) C2 over C3 spondyloptosis in case with absent posterior elements: report of unusual case and analysis of treatment options. J Clin Neurosci 11:675–677
Goffin G, Grob D (1999) Spondyloptosis of the cervical spine in neurofibromatosis. A case report. Spine 24:587–590
Garneti N, Dunn D, El Gamal E et al (2003) Cervical spondyloptosis caused by aneurysmal bone cyst: a case report. Spine 228:68–70
Riggins RS, Kraus JF (1977) The risk of neurologic damage with fracture of the vertebrae. J Trauma 17:126–133
Ido K, Murakami H, Kawagushi H et al (2002) An unusual reduction technique prior to surgical treatment for traumatic spondylolisthesis in the lower cervical spine. J Clin Neurosci 9:664–666 (discussion 7)
Menku A, Kurtsoy A, Tucer B et al (2004) The surgical management of traumatic C6-C7 spondyloptosis in a patient without neurological deficits. Minim Invasive Neurosurg 47:242–244
Tumialan LM, Dadashev V, Laborde DV, Gupta SK (2009) Management of traumatic cervical spondyloptosis in a neurologically intact patient. Case report. Spine 34:E703–E708
Mahale YJ, Silver JR, Henderson NJ (1993) Neurological complications of the reduction of cervical spine dislocations. J Bone J Surg 75B:403–409
Akay KM, Ersahin Y, Tabur E (2002) Cervical spondyloptosis. A case report. Minim Invasive Neurosurg 45:169–172
Bhojraj SY, Shahane SM (1992) Posttraumatic cervical spondyloptosis at C6–C7 with late–onset cord compression: a new clinical entity. Case report. J Neurosurg 177:792–794
Lee DG, Hwang SH, Lee CH, Kang DH (2007) Clinical experience of traumatic C7-T1 spondyloptosis. J Korean Neurosurg Soc 41:127–129
Shah KC, Rajshekhar V (2004) Successful management of posttraumatic C7-T1 with uninstrumented ventral surgery. Surg Neurol 62:431–434
Tiberin P, Hertzanu Y (1994) Complete traumatic dislocation of the cervical spine without permanent neurologic sequelae. Neurochirurgie 40:381–387
Srivastava SK, Agrawal KM, Sharma AK et al (2010) C3-C4 spondyloptosis without neurological deficits-a case report. Spine J 10:e16–e20
Acikbas C, Gurkanlar D (2010) Post-traumatic C7-T1 spondyloptosis in a patient without neurological deficit: a case report. Turkish Neurosurg 20:257–260
Chadha M, Singh AP, Singh AP (2010) Spondyloptosis of C6-C7: a rare case report. Chin J Traumatol 13:377–379
Tumialan LM, Theodore N (2012) Basilar artery thrombosis after reduction of cervical spondyloptosis: a cautionary report. J Neurosurg Spine 16:492–496
Sulla I, Mach P (2001) A patient with spontaneous healing of traumatic spondylolisthesis of the cervical vertebrae. Case report. Rozhl Chir 80:217–219
Gasco J, Dilorenzo DJ, Patterson JT (2013) C4-C5 post-traumatic spondyloptosis with in situ fusion: Systematic literature review and case report. Spine 38:E621–E625
Merianos P, Manousidis D, Samsonas P et al (1994) Injuries of the lower cervical spine associated with widening of the spinal canal. Injury 25:645–648
Eismont F, Clifford S, Goldberg M, Green B (1984) Cervical sagittal spinal canal size in spine injury. Spine 9:663–666
Jeanneret B, Magerl F, Ward JC (1991) Overdistraction: a hazard of skull traction in the management of acute injuries of the cervical spine. Arch Orthop Trauma Surg 110:242–245
Maiman DJ, Barolat G, Larson SJ (1986) Management of bilateral locked facets of the cervical spine. Neurosurgery 18:542–547
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ramieri, A., Domenicucci, M., Cellocco, P. et al. Traumatic spondylolisthesis and spondyloptosis of the subaxial cervical spine without neurological deficits: closed re-alignment, surgical options and literature review. Eur Spine J 23 (Suppl 6), 658–663 (2014). https://doi.org/10.1007/s00586-014-3560-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-014-3560-z