
Abstract
Purpose
The aim of this study was to assess the usefulness and accuracy of a handheld ultrasound device (Accuro, Rivanna Medical, Charlottesville, VA, USA) for epidural landmark and depth assessment when epidural anesthesia is performed by residents.
Methods
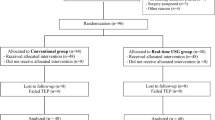
Patients scheduled to receive epidural anesthesia were randomly assigned to the Accuro group (group A) or control group (group C). In group A, the depth to the epidural space and the appropriate place for epidural insertion according to Accuro was recorded. In group C, epidural anesthesia was performed using a conventional method. The following were recorded and compared between the groups: time from puncture of the Tuohy needle to loss of resistance, number of Tuohy needle redirects, and epidural-related complications. In group A, depth to the epidural space estimated by Accuro (Accuro Depth) and the actual depth measured with a marker on the needle (Needle Depth) were recorded and compared.
Results
Sixty patients were enrolled during the study period. There was no significant difference between the groups regarding the median or range of time required to locate the epidural space.
The number of Tuohy needle redirects was 0 (0–3) in group A and 1.5 (0–7) in group C (P = 0.012). Accuro Depth was less than Needle Depth [mean difference, 0.85 cm (95% CI−1.10 to − 0.62), SD = 0.62].
Conclusions
Although there was no significant difference in time from Tuohy needle puncture to loss of resistance, Accuro reduced the number of Tuohy needle redirects and accurately indicated the depth to the epidural space. Accuro may be useful for identifying the needle insertion point and estimating depth to the epidural space when residents perform epidural anesthesia.



Similar content being viewed by others


References
Abrahams MS, Aziz MF, Fu RF, Horn JL. Ultrasound guidance compared with electrical neurostimulation for peripheral nerve block: a systematic review and meta-analysis of randomized controlled trials. Br J Anaesth. 2009;102:408–17.
Barrington MJ, Kluger R. Ultrasound guidance reduces the risk of local anesthetic systemic toxicity following peripheral nerve blockade. Reg Anesth Pain Med. 2013;38:289–99.
Furness G, Reilly MP, Kuchi S. An evaluation of ultrasound imaging for identification of lumbar intervertebral level. Anaesthesia. 2002;57:277–80.
Broadbent CR, Maxwell WB, Ferrie R, Wilson DJ, Gawne-Cain M, Russell R. Ability of anaesthesia to identify a marked lumbar interspace. Anaesthesia. 2000;55:1122–6.
Kim SW, Kim YM, Kim SH, Chung MH, Choi YR, Choi EM. Comparison of loss of resistance technique between Epidrum® and conventional method for identifying the epidural space. Korean J Anesthesiol. 2012;62:322–6.
Gülen G, Akkaya T, Ozkan D, Kaydul M, Gözaydin O, Gümüş H. Comparison of spring-loaded, loss of resistance and hanging drop techniques in lumbar epidural blocks. Agri. 2012;24:37–41.
Tawfik MM, Atallah MM, Elkharboutly WS, Allakkany NS, Abdelkhalek M. Does preprocedural ultrasound increase the first-pass success rate of epidural catheterization before cesarean delivery? A randomized controlled trial. Anesth Analg. 2017;124:851–6.
Seligman KM, Weiniger CF, Carvalho B. The accuracy of a handheld ultrasound device for neuraxial depth and landmark assessment: a prospective cohort trial. Anesth Analg. 2018;126:1995–8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Motonobu Kimizuka has no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Kimizuka, M., Tokinaga, Y., Taguchi, M. et al. Usefulness and accuracy of a handheld ultrasound device for epidurssal landmark and depth assessment by anesthesiology residents. J Anesth 36, 693–697 (2022). https://doi.org/10.1007/s00540-022-03096-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-022-03096-x