
Abstract
Purpose
The aim of this study was to explore the clinical utility of urinary L-FABP for earlier prediction of acute kidney injury (AKI) after emergency laparotomy, and to assess the clinical utility of a point-of-care (POC) kit for urinary L-FABP.
Methods
Forty-eight patients undergoing emergency laparotomy were divided into AKI and non-AKI groups by the kidney diseases: improving global outcome (KDIGO) criteria. Ten patients were included in the AKI group. Urinary L-FABP, albumin, N-acetyl-β-d-glucosaminidase (NAG), TIMP-2, IGFBP7, serum creatinine (SCr), and blood presepsin were measured perioperatively and compared between groups. Perioperative urinary L-FABP was also evaluated qualitatively using a POC kit.
Results
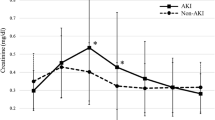
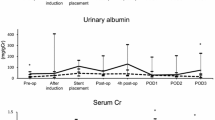
L-FABP and albumin levels were significantly higher in the AKI group at all measurement points. NAG was significantly higher only postoperatively in the AKI group. There were no inter-group differences in [TIMP-2] × [IGFBP7] at any measuring point. The area under the receiver operating characteristic curve of urinary L-FABP was greater than 0.8 perioperatively, which was larger than that of other biomarkers throughout the study period. The correlation coefficient at 2 h after entering the operating room between quantitative and qualitative tests for urinary L-FABP was 0.714, which was the maximum. The sensitivity, specificity, and negative predictive value of the urinary L-FABP POC kit at 2 h after entry were 55.6%, 91.9%, and 89.5%, respectively.
Conclusion
Quantitative L-FABP analyses is suitable for predicting postoperative AKI earlier in the perioperative period of emergency laparotomy. Conversely, the higher specificity of qualitative L-FABP analysis suggests that it may be useful for excluding the risk of AKI but its overall clinical validity should be further investigated.

Similar content being viewed by others

References
Kheterpal S, Tremper KK, Heung M, Rosenberg AL, Englesbe M, Shanks AM, Campbell DA. Development and validation of an acute kidney injury risk index for patients undergoing general surgery: results from a national data set. Anesthesiology. 2009;110:505–15.
Grams ME, Sang Y, Coresh J, Ballew S, Matsushita K, Molnar MZ, Szabo Z, Kalantar-Zadeh K, Kovesdy CP. Acute kidney injury after major surgery: a retrospective analysis of Veterans Health Administration data. Am J Kidney Dis. 2016;67:872–80.
Kidney disease: improving global outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2:1–138.
Doi K, Nishida O, Shigematsu T, Sadahiro T, Itami N, Iseki K, Yuzawa Y, Okada H, Koya D, Kiyomoto H, Shibagaki Y. The Japanese Clinical Practice Guideline for acute kidney injury 2016. J Intensive Care. 2018;6:48.
Doi K, Yuen PS, Eisner C, Hu X, Leelahavanichkul A, Schnermann J, Star RA. Reduced production of creatinine limits its use as marker of kidney injury in sepsis. J Am Soc Nephrol. 2009;20:1217–21.
Godin M, Murray P, Mehta RL. Clinical approach to the patient with AKI and sepsis. Semin Nephrol. 2015;35:12–22.
Matsui K, Kamijo-Ikemori A, Sugaya T, Yasuda T, Kimura K. Usefulness of urinary biomarkers in early detection of acute kidney injury after cardiac surgery in adults. Circ J. 2012;76:213–20.
Obata Y, Kamijo-Ikemori A, Ichikawa D, Sugaya T, Kimura K, Shibagaki Y, Tateda T. Clinical usefulness of urinary liver-type fatty-acid-binding protein as a perioperative marker of acute kidney injury in patients undergoing endovascular or open-abdominal aortic aneurysm repair. J Anesth. 2016;30:89–99.
Ware LB, Johnson AC, Zager RA. Renal cortical albumin gene induction and urinary albumin excretion in response to acute kidney injury. Am J Physiol Ren Physiol. 2011;300:F628–38.
Mårtensson J, Martling CR, Bell M. Novel biomarkers of acute kidney injury and failure: clinical applicability. Br J Anaesth. 2012;109:843–50.
Kianoush K, Xiaoyan W. Kidney stress biomarkers. Crit Care Nephrol. 2019;e3:148–53.
Kashani K, Cheungpasitporn W, Ronco C. Biomarkers of acute kidney injury: the pathway from discovery to clinical adoption. Clin Chem Lab Med. 2017;55:1074–89.
Kianoush K, Ali Al K, Thomas A, Antonio A, Sean MB, Max B, Azra B, Robert B, Cynthia MC, Lakhmir SC, Danielle LD, Thorsten F, Lui GF, Michelle NG, Kyle JG, Michael H, James H, Patrick MH, Eric AJH, Olivier JB, Michael J, Patrick K, Jay LK,Daniel TL, Matthew EL, Gernot M, Peter AM, Scott M, Marlies O, Thomas R, Nathan IS, Andrew DS, Jing S, Amy MS, Jean LV, Christophe V, Ludwig W, Michael GW, R Gentry W, Kai Z, John AK. Discovery and validation of cell cycle arrest biomarkers in human acute kidney injury. Clin Trials. 2013;17:R25.
Gunnerson KJ, Shaw AD, Chawla LS, Bihorac A, Al-Khafaji A, Kashani K, Lissauer M, Shi J, Walker MG, Kellum JA. TIMP2•IGFBP7 biomarker panel accurately predicts acute kidney injury in high-risk surgical patients. J Trauma Acute Care Surg. 2016;80:243–9.
Kamijo A, Sugaya T, Hikawa A, Okada M, Okumura F, Yamanouchi M, Honda A, Okabe M, Fujino T, Hirata Y, Omata M. Urinary excretion of fatty acid-binding protein reflects stress overload on the proximal tubules. Am J Pathol. 2004;165:1243–55.
Tanabe J, Ogura Y, Nakabayashi M, Nagai Y, Watanabe S, Sugaya T, Ohata K, Ichikawa D, Inoue K, Hoshino S, Kimura K. The possibility of urinary liver-type fatty acid-binding protein as a biomarker of renal hypoxia in spontaneously diabetic Torii fatty rats. Kidney Blood Press Res. 2019;44:1476–92.
Ribichini F, Graziani M, Gambaro G, Pasoli P, Pighi M, Pesarini G, Abaterusso C, Yabarek T, Brunelleschi S, Rizzotti P, Lupo A. Early creatinine shifts predict contrast-induced nephropathy and persistent renal damage after angiography. Am J Med. 2010;123:755–63.
Sato E, Kamijo-Ikemori A, Oikawa T, Okuda A, Sugaya T, Kimura K, Nakamura T, Shibagaki Y. Urinary excretion of liver-type fatty acid-binding protein reflects the severity of sepsis. Ren Replace Ther. 2017;3:26.
Doi K, Katagiri D, Negishi K, Hasegawa S, Hamasaki Y, Fujita T, Matsubara T, Ishii T, Yahagi N, Sugaya T, Noiri E. Mild elevation of urinary biomarkers in prerenal acute kidney injury. Kidney Int. 2012;82:1114–20.
Cummings JJ, Shaw AD, Shi J, Lopez MG, O’Neal JB, Billings FT. Intraoperative prediction of cardiac surgery–associated acute kidney injury using urinary biomarkers of cell cycle arrest. J Thorac Cardiovasc Surg. 2019;157:1545-1553.e5.
Meersch M, Schmidt C, Van Aken H, Martens S, Rossaint J, Singbartl K, Görlich D, Kellum JA, Zarbock A. Urinary TIMP-2 and IGFBP7 as early biomarkers of acute kidney injury and renal recovery following cardiac surgery. PLOS ONE. 2014;9:e93460.
Finge T, Bertran S, Roger C, Candela D, Pereira B, Scott C, Muller L, Louart B, Lefrant JY. Interest of Urinary [TIMP-2] × [IGFBP-7] for predicting the occurrence of acute kidney injury after cardiac surgery: a Gray Zone Approach. Anesth Analg. 2017;125:762–9.
Jan W, Carmen AP, Noelle S, Roman B, Juerg S, Gabor E, Joerg CS. (TIMP2) × (IGFBP7) as early renal biomarker for the prediction of acute kidney injury in aortic surgery (TIGER). A single center observational study. PLOS ONE. 2021;16:e0244658.
Acknowledgements
We would like to thank Editage (www.editage.com) for English language editing. We thank Ms. Sachi Shinmi for her technical assistance. In addition, we thank Dr. Miki Sakamoto, Dr. Makito Yokozuka, Dr. Yu Sato, Dr. Yuki Abukawa, Dr. Eriko Amano, Dr. Yu Somemura, Dr. Miyuna Sato, and Dr. Ayako Yamaura for sample collection.
Author information
Authors and Affiliations
Contributions
HO, YO, AKI, and SI contributed to the study design, execution of the study, and manuscript preparation. All authors have approved the final manuscript and attest to the integrity of the original data and the analyses described in the paper.
Corresponding author
Ethics declarations
Conflict of interest
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Okuda, H., Obata, Y., Kamijo-Ikemori, A. et al. Quantitative and qualitative analyses of urinary L-FABP for predicting acute kidney injury after emergency laparotomy. J Anesth 36, 38–45 (2022). https://doi.org/10.1007/s00540-021-03003-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-021-03003-w