
Abstract
Purpose
We evaluated whether longer term hemodialysis (HD) is associated with a higher incidence of vasoplegic syndrome (VS) after cardiac surgery.
Methods
This retrospective, single-center cohort study included 562 consecutive patients who underwent cardiac surgery in a tertiary hospital from January 2015 to December 2016. We assessed VS occurrence and its relationship with HD duration and other risk factors. To assess the effect of the HD duration on VS occurrence, we constructed ordinal variables: HD = 0 (non-HD), 0 < HD ≤ 5 (HD ≤ 5 years), 5 < HD ≤ 10, and 10 < HD.
Results
The overall mean (± standard deviation) age of patients was (73 ± 11) years, and there were 60.9% men. Forty-one patients (7.3%) were HD dependent. Cardiac surgeries included all coronary artery bypass graft procedures, all valvular procedures, and aortic surgery involving cardiopulmonary bypass (CPB). Sixty-six patients (10%) developed VS. Most preoperative patient characteristics were comparable between the VS and no-VS groups; a chronic HD status and a total CPB time of > 180 min were significantly more common in the VS group (P < 0.0001 and P = 0.02, respectively). Longer term HD significantly correlated with VS incidence (P < 0.0001). Ordinal variables for the HD duration and age and known risk factors for VS (preoperative use of angiotensin-converting enzyme inhibitors and beta-blockers, low left-ventricular ejection fraction, and CPB time > 180 min) were subjected to multivariate regression analysis. Long-term HD was identified as an independent predictor of VS (odds ratio, 2.29, 95% confidence interval, 1.66–3.18).
Conclusions
Longer term HD may be associated with a higher VS incidence after cardiac surgery. VS should be given attention after cardiac surgery in chronic HD-dependent patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Vasoplegic syndrome (VS) frequently occurs in the early postoperative period of cardiac surgery. Its incidence rate is about 10–20% in the post-cardiac surgery setting [1]. VS occurring after cardiac surgery is the second most common cause of vasoplegia, next to sepsis [2]. It is characterized by significant hypotension, with decreased systemic vascular resistance, decreased arteriolar reactivity, increased requirements for vasopressors, and high or normal cardiac output [3, 4].
Some risk factors such as preoperative use of angiotensin-converting enzyme (ACE) inhibitors and beta-blockers, a low left-ventricular ejection fraction (EF), and cardiopulmonary bypass (CPB) surgery, among others have been reported [4,5,6,7,8,9]. Although there is an overall agreement regarding the effect of specific risk factors for VS, other factors are more controversial. In recent literature, chronic hemodialysis (HD)-dependent renal failure has been suggested to be a risk factor for VS because of its chronic inflammatory status [10, 11]. Repeated dialysis treatments in patients with chronic renal failure (CRF) are considered to promote an inflammatory response [12], although the duration of HD has not yet been examined in detail. We hypothesized that a longer period of dialysis results in an increased frequency of VS. Thus, our study aimed to evaluate whether longer term hemodialysis (HD) is associated with a higher incidence of VS after cardiac surgery.
Methods
This single-center, retrospective cohort study was conducted after approval from the institutional review board at the Kobe City Medical Center General Hospital (Approval number: 3, March 3, 2017), which waived the requirement for informed consent because of the anonymous nature of the data. Consecutive patients who underwent cardiac surgery in a tertiary hospital in Japan from January 2015 to January 2016 were included. Patients older than 18 years who presented for elective cardiac surgery were considered eligible.
Cardiac surgery included all coronary artery bypass graft (CABG) procedures (on-pump, off-pump), all valvular procedures, and aortic surgery requiring circulatory arrest. Patients requiring mechanical support via an intra-aortic balloon pump or ventilator-assisted extracorporeal membrane oxygenation on admission to the intensive care unit (ICU) were excluded.
For each patient, we recorded the mean arterial pressure (MAP), cardiac index (CI), and central venous pressure (CVP). A pulmonary artery flotation catheter (PAC) was inserted during surgery, and its placement was checked by chest radiography on admission to ICU. CI was measured by a continuous thermodilution catheter. MAP was measured using a femoral or radial arterial catheter inserted during surgery. CVP was measured using the proximal port of PAC. These values were documented at 0, 2, 4, 8, and 16 h after transfer to ICU. We also recorded the following preoperative variables: sex; age; type of surgical procedure; EF; use of ACE inhibitors; use of beta-blockers; and the presence of diabetes mellitus, hypercholesterolemia, systemic hypertension, stroke, obesity (body mass index [BMI] > 25 kg/m2), myocardial infarction, angina pectoris, and chronic obstructive pulmonary disease (COPD). We noted the following intraoperative variables: CPB use, pump time, and cross-clamp time.
Definitions
There were no clear diagnostic criteria for VS; therefore, we based our definition of VS on previous reports [7], adapted to a clinical context. VS was defined as present when three of the following four conditions were met: (1) MAP < 65 mmHg, (2) a decreased systemic vascular resistance index (SVRI) < 1.600 dyn∙s/cm5/m2, (3) a high CI (CI > 2.5 L/min/m2), and (4) requirement of pharmacological support from norepinephrine (> 0.03 μg/kg/min) or vasopressin. Patients who met these criteria at two consecutive time points within 0, 2, 4, 8, and 16 h after transfer to ICU were diagnosed with VS. More specifically we categorized VS as mild if MAP was between 50 and 60 mmHg and one vasopressor was being administered; moderate if MAP was between 50 and 60 mmHg and two or more vasopressors were being administered, or MAP was < 50 mmHg and one vasopressor was being administered; severe if MAP was < 50 mmHg and two or more vasopressors were being administered, based on the previous literature [10]. The vasopressors utilized included norepinephrine, vasopressin, and epinephrine.
Statistical analysis
Nominal variables are reported as counts and percentages, while continuous variables are reported as means and standard deviations (SDs). Chi-square and Fisher’s exact tests for nominal variables and t test for continuous variables were used to compare patients who developed VS with those who did not. A multivariate logistic regression model was used to assess the risk factors for VS. Age and known risk factors for VS reported in a previous study (preoperative use of ACE inhibitors and beta-blockers, a low left-ventricular EF, and CPB time > 180 min) were subjected to multivariate analysis. To assess the effect of the HD duration on the occurrence of VS, we constructed ordinal variables, namely non-HD (HD = 0), 0 < HD ≤ 5 (≤ 5 years), 5 < HD ≤ 10, and 10 < HD, and included them in the multivariate logistic model. A two-tailed P value of < 0.05 was considered statistically significant. All statistical analyses were performed using JMP 13 software (SAS Institute Inc., Cary, NC).
Results
During the study period, a total of 598 patients who had undergone elective cardiac surgery were identified. In total, 32 patients were excluded because they required mechanical support via an intra-aortic balloon pump or ventilator-assisted extracorporeal membrane oxygenation on admission to ICU. Four patients were excluded because of missing data. Finally, 562 patients were included. The demographic data of all patients are shown in Table 1. Except for hypertension, preoperative patient characteristics were not significantly different between the two groups. The overall mean (± SD) age of patients was (73 ± 11) years. The prevalences of hypercholesterolemia, systemic hypertension, stroke, obesity (BMI > 25 kg/m2), myocardial infarction, angina pectoris, and COPD were not significantly different between the two groups.
Number of operations
Cardiac surgeries included all CABG procedures (on-pump [N = 101] and off-pump [N = 37]), all valvular procedures (N = 259), and large vascular surgery involving CPB (N = 149; Table 2). Aortic surgery involved ascending aorta replacement, aortic root replacement, aortic arch replacements, and descending aorta replacement.
Perioperative parameters
In total, 66 patients (10%) developed VS; 27 (40.9%), 15 (22.7%), 15 (22.7%), and 9 (13.6%) were diagnosed at 0–2, 2–4, 4–8, and 8–16 h after transfer to the ICU, respectively. Of these 66 patients, 48 (72.7%) had mild, 15 (22.7%) had moderate, and 3 (4.5%) had severe VS. Overall, 41 (7.3%) patients were chronically HD dependent, while the remaining 521 (92.7%) were not. Table 3 shows the perioperative parameters for the patients. Chronic HD dependence and a total CPB time exceeding 180 min were significantly more common in the VS group than in the control group (P < 0.0001 and P = 0.02, respectively). Preoperative use of ACE inhibitors and beta-blockers was not statistically significantly different between the two groups.
Postoperative parameters and clinical course
The postoperative variables are shown in Table 4, which reveals the cardiovascular data and requirement for vasopressor and inotropic agents for the two groups. For the purpose of our analysis, minimal MAP, minimal SVRI, maximal CI, and the actual maximum dosage of norepinephrine required by each group are listed in Table 4. Minimal SVRI and minimal MAP were significantly lower in the VS group than in the control group (P < 0.001, respectively). Maximal CI was significantly higher in the VS group than in the control group (3.6 (± 0.66) vs 2.9 (± 0.64) L/min/m2, P < 0.001, respectively). The dosage of norepinephrine required was significantly higher in the VS group than in the control group (0.076 (± 0.07) vs 0.004 (± 0.052) µg/kg/min, P < 0.001, respectively). The overall mean duration of norepinephrine infusion for the VS patients was 12.05 (± 5.98) h, while the duration for the patients with mild, moderate, and severe VS was 10.11 (± 6.03) h, 14.45 (± 5.78) h, and 8.23 (± 3.77) h.
The lengths of ICU stay and overall hospital stay were significantly longer in the VS group than in the control group (P < 0.001 and P = 0.03, respectively), while ICU and hospital mortality rates were higher in the VS group (P = 0.04 and P = 0.002, respectively).
Association between HD duration and VS incidence
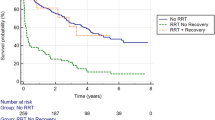
Figure 1 shows the association between the HD duration (HD = 0, 0 < HD ≤ 5, 5 < HD ≤ 10, 10 < HD) and the incidence of VS. The incidences of VS were 9.6% (HD = 0), 31.3% (0 < HD ≤ 5), 33.3% (5 < HD ≤ 10), and 50% (10 < HD), respectively. We found that longer term HD was significantly correlated with an increasing VS incidence (P < 0.0001).

Association between the hemodialysis duration and incidence of vasoplegic syndrome after cardiac surgery
Multivariate analysis
Ordinal variables for HD duration (HD = 0, 0 < HD ≤ 5, 5 < HD ≤ 10, 10 < HD), age, and known risk factors for VS (preoperative use of ACE inhibitors and beta-blockers, a low left ventricular EF, and CPB time > 180 min) were subjected to multivariate regression analysis (Table 5), which identified long-term HD as an independent predictor for post-cardiac surgery VS (odds ratio [OR], 2.29; 95% confidence interval [CI], 1.66–3.18). A total CPB duration of > 180 min was another independent predictor (OR, 1.81, 95%CI, 1.05–3.10).
Discussion
In our study, longer term HD and prolonged CPB were identified as predictors of VS after cardiac surgery. Our results are supported by the recent observations of Tsiouris et al. [10], who reported that HD-dependent renal failure is a predictive factor for VS. Hossne Junior et al. [11] demonstrated that CABG procedures with CPB in patients with CRF requiring dialysis therapy were an independent risk factor for the development of postoperative VS. However, accurate assessment of chronic HD as an independent risk factor for VS was difficult because of the small number of patients with chronic HD. In the present study, we demonstrated this by directly comparing chronic HD-dependent patients with non-dependent patients and adjusting the results for confounding factors in a multivariate regression analysis. We then examined the association between HD duration and the incidence of VS and found that a longer period of dialysis resulted in more frequent occurrences of VS, with a statistically significant difference. To the best of our knowledge, this is the first report to show that longer term HD increases the risk of VS after cardiac surgery.
VS is a well-known complication after cardiac surgery [13]. Patients who develop VS after cardiac surgery exhibit increased mortality and a longer hospital stay [14]. Multiple risk factors have been identified that can help predict VS, including preoperative use of ACE inhibitors and beta-blockers, a low left-ventricular EF, and CPB use [4,5,6,7,8,9].
Chronic HD has been suggested to be a risk factor for VS, but the mechanisms remain unclear. The pathophysiological mechanisms underlying VS remain controversial; however, there is a clear association between the expression of pro-inflammatory mediators and subsequent induction of nitric oxide production and cyclic guanosine monophosphate-mediated severe vasodilation [2, 15, 16]. Moreover, chronic inflammation is prevalent in patients with CRF [17], and repeated dialysis treatments in such patients lead to leucocyte activation and consequently, cytokine production [12]. We expected that longer term HD-dependent CRF would increase the risk of post-cardiac surgery VS. Moreover, we showed that chronic HD dependence is a risk factor for VS, and that VS develops more frequently in patients who require longer term HD. It is reasonable to surmise that the intrinsic chronic inflammatory status in patients with HD-dependent CRF promotes an inflammatory response leading to VS, and that longer term HD develops a strong tendency for this response.
Our findings can be utilized in clinical practice. When patients with chronic HD dependence, particularly long-term HD, exhibit distributive shock in postoperative care, VS should be considered as a differential diagnosis. It is very important to distinguish VS from other possible diagnoses, such as septic shock and anaphylactic shock, because this may change the treatment plans. The use of vasopressin did not produce a statistically significant improvement in the mortality rate of patients in a meta-analysis [18]. However, Hajjar et al. [14] found that vasopressin can be used as a first-line vasopressor for post-cardiac surgery VS and improves patient clinical outcomes. In the future, the threshold for vasopressin initiation for the treatment of distributive shock after cardiac surgery may change.
Our study had several limitations. First, because of the retrospective design, confounding factors may have affected our results. The influence of unknown risk factors cannot be ruled out. We included major known risk factors in the multivariate analysis to eliminate the influence of more confounding factors, but this might not have been sufficient. Second, we devised the diagnostic criteria for VS based on previous reports, because there are no clear or standardized criteria. The appropriate timing for evaluation also remains unclear. We determined the timing for evaluation as 0, 2, 4, 8, and 16 h after transfer to ICU in accordance with a previous representative report that specified these timings [5], but these different intervals may have affected VS diagnosis. The purpose of evaluation at two consecutive time points was to increase the specificity of the diagnostic criteria for VS. The early postoperative period is especially important for diagnosis because VS is characterized by occurring early after surgery; therefore, we consider our criteria to be clinically appropriate. Third, severity of VS in this study may have been relatively mild compared to previous reports. There were very few patients categorized as having severe VS, and the overall mortality rate was relatively low compared with previous reports [7, 10]. However, it cannot be said sweepingly, because there is no definitive severity classification of VS and there are very little data about VS mortality. Further studies are needed to clarify severity and prognosis of VS. Fourth, our study only assessed chronic HD dependence or non-dependence; thus, we did not assess the direct relationship between CRF and VS. It is unclear whether the main predictor of VS is HD or CRF, and whether mild CRF is a risk factor for VS. Further research is needed to assess the relationship between CRF, renal function, disease duration, and post-cardiac surgery VS.
In conclusion, chronic HD was identified as a predictor of VS, and longer term HD was associated with a higher incidence of VS after cardiac surgery. In the postoperative care of chronic HD-dependent patients who have undergone cardiac surgery, VS should be kept in mind as a differential diagnosis.
References
Cremer J, Martin M, Redl H, Bahrami S, Abraham C, Graeter T, Haverich A, Schlag G, Borst HG. Systemic inflammatory response syndrome after cardiac operations. Ann Thorac Surg. 1996;61:1714–20.
Lambden S, Creagh-Brown BC, Hunt J, Summers C, Forni LG. Definitions and pathophysiology of vasoplegic shock. Crit Care. 2018;22:174.
Levy B, Fritz C, Tahon E, Jacquot A, Auchet T, Kimmoun A. Vasoplegia treatments: the past, the present, and the future. Crit Care. 2018;22(1):52.
Mekontso-Dessap A, Houël R, Soustelle C, Kirsch M, Thébert D, Loisance DY. Risk factors for postcardiopulmonary bypass vasoplegia in patients with preserved left ventricular function. Ann Thorac Surg. 2001;71:1428–32.
Carrel T, Englberger L, Mohacsi P, Neidhart P, Schmidli J. Low systemic vascular resistance after cardiopulmonary bypass: incidence, etiology, and clinical importance. J Card Surg. 2000;15:347–53.
Egi M, Bellomo R, Langenberg C, Haase M, Haase A, Doolan L, Matalanis G, Seevenayagam S, Buxton B. Selecting a vasopressor drug for vasoplegic shock after adult cardiac surgery: a systematic literature review. Ann Thorac Surg. 2007;83:715–23.
Kristof AS, Magder S. Low systemic vascular resistance state in patients undergoing cardiopulmonary bypass. Crit Care Med. 1999;27:1121–7.
Sun X, Zhang L, Hill PC, Lowery R, Lee AT, Molyneaux RE, Corso PJ, Boyce SW. Is incidence of postoperative vasoplegic syndrome different between off-pump and on-pump coronary artery bypass grafting surgery? Eur J Cardiothorac Surg. 2008;34:820–5.
Ascione R, Lloyd CT, Underwood MJ, Lotto AA, Pitsis AA, Angelini GD. Inflammatory response after coronary revascularization with or without cardiopulmonary bypass. Ann Thorac Surg. 2000;69:1198–204.
Tsiouris A, Wilson L, Haddadin AS, Yun JJ, Mangi AA. Risk assessment and outcomes of vasoplegia after cardiac surgery. Gen Thorac Cardiovasc Surg. 2017;65:557–65.
Hossne Junior NA, Miranda M, Monteiro MR, Branco JN, Vargas GF, Pestana JO, Gomes WJ. Cardiopulmonary bypass increases the risk of vasoplegic syndrome after coronary artery bypass grafting in patients with dialysis-dependent chronic renal failure. Rev Bras Cir Cardiovasc. 2015;30:482–8.
Tbahriti HF, Meknassi D, Moussaoui R, Messaoudi A, Zemour L, Kaddous A, Bouchenak M, Mekki K. Inflammatory status in chronic renal failure: The role of homocysteinemia and pro-inflammatory cytokines. World J Nephrol. 2013;2:31–7.
Liu H, Yu L, Yang L, Green MS. Vasoplegic syndrome: an update on perioperative considerations. J Clin Anesth. 2017;40:63–71.
Hajjar LA, Vincent JL, Rhodes A, Landoni G, Osawa EA, Melo RR, Sundin MR, Grande SM, Gaiotto FA, Pomerantzeff PM, Dallan LO, Franco RA, Nakamura RE, Lisboa LA, de Almeida JP, Gerent AM, Souza DH, Gaiane MA, Fukushima JT, Park CL, Zambolim C, Rocha Ferreira GS, Strabelli TM, Fernandes FL, Camara L, Zeferino S, Santos VG, Piccioni MA, Jatene FB, Costa Auler JO, Jr FRK. Vasopressin versus norepinephrine in patients with vasoplegic shock after cardiac surgery: The VANCS Randomized Controlled Trial. Anesthesiology. 2017;126:85–93.
Fischer GW, Levin MA. Vasoplegia during cardiac surgery: current concepts and management. Semin Thorac Cardiovasc Surg. 2010;22:140–4.
Levin MA, Lin HM, Castillo JG, Adams DH, Reich DL, Fischer GW. Early on-cardiopulmonary bypass hypotension and other factors associated with vasoplegic syndrome. Circulation. 2009;120:1664–711.
Kaysen GA. Inflammation: cause of vascular disease and malnutrition in dialysis patients. Semin Nephrol. 2004;24:431–6.
Dünser MW, Bouvet O, Knotzer H, Arulkumaran N, Hajjar LA, Ulmer H, Hasibeder WR. Vasopressin in cardiac surgery: a meta-analysis of randomized controlled trials. J Cardiothorac Vasc Anesth. 2018;32:2225–32.
Acknowledgements
We greatly appreciate the cooperation of the members of clinical research, innovation and education center. We are also grateful to all the investigators in this study.
Author information
Authors and Affiliations
Contributions
MS: conceived and designed the study, performed the statistical analyses, and drafted the manuscript. DK: the principal supervisor of this project, organized the original study plan, and co-wrote the final manuscript. HU: conceived and designed the study and helped draft and revise the manuscript. TS: conceived and designed the study. HM: the supervisor of ethical approval. JI: revised the manuscript for important intellectual contributions. RS: revised the manuscript for important intellectual contributions. AK: revised the manuscript for important intellectual contributions. YN: conceived and designed the study. TM: helped design the study, analyze the data, and draft the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they do not have any conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Suga, M., Kawakami, D., Ueta, H. et al. Longer term hemodialysis-dependent chronic renal failure increases the risk of post-cardiac surgery vasoplegic syndrome. J Anesth 34, 243–249 (2020). https://doi.org/10.1007/s00540-019-02727-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-019-02727-0