
Abstract
Purpose
Increased glucose variability may be associated with worse outcomes in critically ill patients. Hyperinsulinemic normoglycemia provides intensive glucose control during surgery and may reduce glucose variability. Our objective was to compare glycemic variability between two methods of glucose control in cardiac surgical patients: hyperinsulinemic normoglycemia vs standard insulin infusion. We also assessed whether the effect differed between patients with and without diabetes mellitus.
Methods
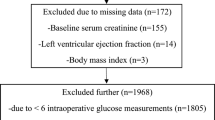
We compared measures of glycemic variability, including the primary outcome, average real variability (ARV), and secondary outcomes, within-patient standard deviation (SD) and glucose lability index (GLI), in 252 patients who received hyperinsulinemic normoglycemia and 266 patients who received standard therapy. Data was randomly sampled from each patient treated with hyperinsulinemic normoglycemia, so patients in each group had a similar number of glucose measurements. The significance level for each hypothesis was 0.05, and 0.025 within diabetic status.
Results
For nondiabetic patients, hyperinsulinemic normoglycemia reduced mean glucose measure-to-measure variability for ARV by an estimated −0.23 (97.5% CI −0.30, −0.16) mg/dl/min (P < 0.001) versus standard care. There was no difference in glycemic variability between groups for diabetic patients, with difference in means (97.5% CI) of −0.10 (−0.20, 0.02) mg/dl/min, P = 0.07. Mean SD was lower for hyperinsulinemic normoglycemia patients overall, with difference in means (95% CI) of −19 (−22, −16), P < 0.001, with a stronger effect in nondiabetics (interaction P = 0.042). GLI was also lower with hyperinsulinemic normoglycemia.
Conclusion
Hyperinsulinemic normoglycemia decreases glucose variability for cardiac surgical patients with a stronger effect in nondiabetic patients.


Similar content being viewed by others


References
Duncan AE, Abd-Elsayed A, Maheshwari A, Xu M, Soltesz E, Koch CG. Role of intraoperative and postoperative blood glucose concentrations in predicting outcomes after cardiac surgery. Anesthesiology. 2010;112:860–71.
The DCCT Research Group. The relationship of a glycemic exposure (HbA1c) to the risk of development and progression of retinopathy in the diabetes control and complications trial. Diabetes. 1995;44:968–83.
Klein R. Hyperglycemia and microvascular and macrovascular disease in diabetes. Diabetes Care. 1995;18:258–685.
Quagliaro L, Piconi L, Assaloni R, Martinelli L, Motz E, Ceriello A. Intermittent high glucose enhances apoptosis related to oxidative stress in human umbilical vein endothelial cells: the role of protein kinase C and NAD(P)H-oxidase activation. Diabetes. 2003;52:2795–804.
Monnier L, Mas E, Ginet C, Michel F, Villon L, Cristol JP, Colette C. Activation of oxidative stress by acute glucose fluctuations compared with sustained chronic hyperglycemia in patients with type 2 diabetes. JAMA. 2006;295:1681–7.
Risso A, Mercuri F, Quagliaro L, Damante G, Ceriello A. Intermittent high glucose enhances apoptosis in human umbilical vein endothelial cells in culture. Am J Physiol Endocrinol Metab. 2001;281:E924–30.
Ali NA, O’Brien JM Jr, Dungan K, Phillips G, Marsh CB, Lemeshow S, Connors AF Jr, Preiser JC. Glucose variability and mortality in patients with sepsis. Crit Care Med. 2008;36:2316–21.
Egi M, Bellomo R, Stachowski E, French CJ, Hart G. Variability of blood glucose concentration and short-term mortality in critically ill patients. Anesthesiology. 2006;105:244–52.
Sato H, Carvalho G, Sato T, Bracco D, Codere-Maruyama T, Lattermann R, Hatzakorzian R, Matsukawa T, Schricker T. Perioperative tight glucose control with hyperinsulinemic-normoglycemic clamp technique in cardiac surgery. Nutrition. 2010;26:1122–9.
Hassanain M, Metrakos P, Fisette A, Doi SA, Schricker T, Lattermann R, Carvalho G, Wykes L, Molla H, Cianflone K. Randomized clinical trial of the impact of insulin therapy on liver function in patients undergoing major liver resection. Br J Surg. 2013;100:610–8.
Sato H, Hatzakorzian R, Carvalho G, Sato T, Lattermann R, Matsukawa T, Schricker T. High-dose insulin administration improves left ventricular function after coronary artery bypass graft surgery. J Cardiothorac Vasc Anesth. 2011;25:1086–91.
Duncan AE, Kateby Kashy B, Sarwar S, Singh A, Stenina-Adognravi O, Christoffersen S, Alfirevic A, Sale S, Yang D, Thomas JD, Gillinov M, Sessler DI. Hyperglycemic normoglycemia does not meaningfully improve myocardial performance during cardiac surgery. Anesthesiology. 2015;123:272–87.
Mascha EJ, Yang D, Weiss S, Sessler DI. Intraoperative mean arterial pressure variability and 30-day mortality in patients having noncardiac surgery. Anesthesiology. 2015;123:79–91.
Ryan EA, Shandro T, Green K, Paty BW, Senior PA, Bigam D, Shapiro AM, Vantyghem MC. Assessment of the severity of hypoglycemia and glycemic lability in type 1 diabetic subjects undergoing islet transplantation. Diabetes. 2004;53:955–62.
Rodbard D. New and improved methods to characterize glycemic variability using continuous glucose monitoring. Diabetes Technol Ther. 2009;11:551–65.
Dungan KM, Binkley P, Nagaraja HN, Schuster D, Osei K. The effect of glycaemic control and glycaemic variability on mortality in patients hospitalized with congestive heart failure. Diabetes Metab Res Rev. 2011;27:85–93.
NICE-SUGAR Study Investigators. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360:1283–97.
Van den Berghe G, Wilmer A, Hermans G, Meersseman W, Wouters PJ, Milants I, Van Wijngaerden E, Bobbaers H, Bouillon R. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006;354(5):449–61.
Van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, Vlasselaers D, Ferdinande P, Lauwers P, Bouillon R. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345:1359–67.
NICE-SUGAR Study Investigators. Hypoglycemia and risk of death in critically ill patients. N Engl J Med. 2012;367:1108–18.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest. Dr. Abd-Elsayed performs consultancy work for Ultimaxx Health, Halyard and Innocol, which is not related to this work.
About this article

Cite this article
Abd-Elsayed, A., Mascha, E.J., Yang, D. et al. Hyperinsulinemic normoglycemia decreases glucose variability during cardiac surgery. J Anesth 31, 185–192 (2017). https://doi.org/10.1007/s00540-016-2295-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-016-2295-x