
Abstract
Purpose
To evaluate patterns of primary prophylactic (PP) granulocyte colony–stimulating factor (G-CSF) use following chemotherapy by cancer type and febrile neutropenia (FN) risk.
Methods
Using a commercial administrative database, we identified adult patients diagnosed with breast, colorectal, lung, ovarian cancer, or non-Hodgkin lymphoma (NHL) who initiated chemotherapy with high risk (HR) or intermediate risk (IR) for FN between January 1, 2013, and August 31, 2017. We describe use of PP-G-CSF, proportion completing all their cycles with pegfilgrastim, timing of pegfilgrastim, and duration of short-acting G-CSF.
Results
Among 22,868 patients (breast 11,513; colorectal 3765; lung 4273; ovarian 1287; and NHL 2030), 36.8% received HR and 63.2% received IR (64.4% of whom had ≥ 1 risk factor [RF] for FN). Proportions of patients receiving PP-G-CSF in the first cycle were 76.1%, 28.2%, and 26.4% among patients receiving HR, IR, and IR plus ≥ 1 RF, respectively. Among breast cancer patients receiving HR regimens and initiating PP-pegfilgrastim, 60.4% (95% confidence interval [CI] 57.2–63.6%) initiating via on-body injector (OBI) and 51.9% (95% CI 48.0–55.8%) initiating via prefilled syringe (PFS) completed all their cycles with OBI and PFS, respectively. Among all cycles with PP-PFS, 8.5% received PFS on the same day as chemotherapy completion. Mean administrations/cycle were 3.2 (standard deviation [SD] 2.3) for filgrastim, 3.0 (SD 1.6) for filgrastim-sndz, and 4.3 (SD 2.5) for tbo-filgrastim.
Conclusions
There is under- and mistimed use of PP-G-CSF among patients at HR for FN. Novel pegfilgrastim delivery devices could help breast cancer patients at HR for FN complete all their cycles with timely prophylaxis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Scientific discovery is leading to rapid advances in our understanding of cancer and is delivering new targeted medicines [1,2,3], leading to substantial clinical benefit. Despite these advances, most patients diagnosed with cancer today are still treated with chemotherapy [4] and are thus at risk of experiencing chemotherapy-related adverse effects such as fatigue, infusion reactions, cognitive dysfunction, cardiovascular or gastrointestinal toxicity, and febrile neutropenia (FN) [5, 6]. Patients diagnosed with solid tumors who develop FN are frequently hospitalized for multiple days at a time [7] often resulting in delays or modifications to scheduled chemotherapy sessions [8], and in some instances, more severe complications including death [9]. The National Comprehensive Care Network (NCCN®) clinical practice guidelines [10] recommend prophylactic use of granulocyte colony–stimulating factor (G-CSF) to promote the growth and differentiation of neutrophils for patients receiving chemotherapy regimens associated with a high risk of developing FN (> 20%) or regimens with intermediate risk of FN (10–20%) and ≥ 1 patient-level risk factor.
There have been important developments in recent years regarding FN management, including greater focus placed on high-quality, low-cost cancer care through efforts such as the Oncology Care Model (OCM) by the Centers for Medicare and Medicaid Services (CMS) [11], the entrance of biosimilars of filgrastim [12,13,14] and pegfilgrastim [15, 16] in the USA, and the introduction of new, patient-centric drug delivery devices [17]. The effects that these changes have had on prescribing patterns and persistence with chemotherapy regimens are largely unknown but are important to establish for future requisite investigations into the clinical consequences of such therapeutic decisions.
To that end, we used data from a nationally representative population of patients with commercial and Medicare Advantage insurance to evaluate the patterns of G-CSF prophylaxis in patients diagnosed with various types of cancer and receiving chemotherapy regimens with high/intermediate FN risk.
Methods
Study design and data source
We used a retrospective cohort study design. The data used in this study came from the Optum™ Clinformatics™ Data Mart (Optum Insight, Eden Prairie, MN) which has been described previously [18]. Briefly, the Optum™ Clinformatics™ Data Mart includes de-identified eligibility, pharmacy, laboratory, medical, and standard pricing data for approximately 15 million people enrolled annually in commercial and Medicare advantage plans by United Health Group and is fully compliant with the Health Insurance Portability and Accountability Act of 1996 [19]. Approximately 20% of Medicare advantage patients in the USA are represented in this database. The population is geographically diverse and spans all 50 states. We used the Date of Death (DOD) data series of the Optum™ Clinformatics™ Data Mart that includes dates of death obtained from the Social Security Administration death master file.
Study population
We identified patients ≥ 18 years of age diagnosed with breast, colorectal, lung, ovarian cancer, or non-Hodgkin lymphoma (NHL) who had initiated myelosuppressive chemotherapy regimens with high/intermediate risk for FN as defined in the 2017 v2. NCCN® clinical practice guidelines [20] (Online Resource 1) from January 1, 2013, to August 31, 2017. Initiation of myelosuppressive chemotherapy was defined as first observed myelosuppressive chemotherapy treatment during the study period without any evidence of myelosuppressive chemotherapy during the preceding 365 days. The date of myelosuppressive chemotherapy initiation was assigned as the index date. All patients were required to have ≥ 365 days of continuous enrollment prior to the index date (i.e., baseline period) to assess patient characteristics and comorbidities (Online Resource 2). The study follow-up period started on the index date and ended on the earliest date of last day of the last cycle of chemotherapy course, last day of cycle 8 of chemotherapy course, occurrence of FN-related hospitalization (≥ 1 inpatient diagnosis claim in any position), bone marrow or stem cell transplant or radiation therapy (≥ 1 inpatient or outpatient diagnosis/procedure claim in any position) (Online Resource 3), death, disenrollment from commercial plan, or December 31, 2017.
We categorized patients by the cancer diagnosis most proximal to the index date of the myelosuppressive chemotherapy (within 365 days preceding and 30 days following the index date) based on the presence of 1 inpatient diagnosis or 2 outpatient diagnoses (separated by ≥ 7 days) from the International Classification of Diseases 9th/10th Revision Clinical Modification (ICD-9-CM/ICD-10-CM) codes (Online Resource 4). Cancer diagnosis was identified using modification of a commonly used algorithm in administrative claims research requiring at least 1 inpatient or at least 2 outpatient diagnoses claims [21]. Because this algorithm has reported high specificity but moderate sensitivity, we required the 2 outpatient diagnoses claims to be ≥ 7 days apart and allowed for a 30-day window beyond the index date to improve its sensitivity. Calendar year cohorts of patients with 5 distinct cancer types were identified: breast, colorectal, lung, ovarian, and NHL. Patients were required to have survived the first 6 days after the index date to ensure enough time to identify the chemotherapy regimen and day of chemotherapy completion in the first chemotherapy cycle. Claims of appropriate injectable chemotherapeutic agents were identified at specified intervals for each chemotherapy regimen and its variations as defined in the source publication listed in NCCN® guidelines (Online Resource 5) [20]. Dose of chemotherapeutic agents was unavailable in the claims database. We excluded patients with ≥ 1 type of non-myeloid cancer diagnosis, and patients with evidence of bone marrow or stem cell transplant or radiation therapy during the baseline period.
Covariate assessment
Age in years and sex were assessed at the index date. Comorbidities were defined based on the presence of ≥ 1 diagnosis claim in an inpatient setting or ≥ 2 diagnosis claims in an outpatient setting (separated by ≥ 30 days) during the baseline period. Neutropenia hospitalization was defined as an inpatient stay with a diagnosis of neutropenia (ICD-9 288.0X; ICD-10 D70.X) in any position. The modified Charlson comorbidity index (CCI) score, adapted for use with administrative claims data and including updated severity weights, was calculated [22, 23].
Patient-level FN risk factors that were assessed during baseline included age > 65 years, liver or renal dysfunction, human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) identified by NCCN® guidelines [10], and also cardiovascular disease (defined as myocardial infarction, heart failure, peripheral vascular disease, or stroke), chronic obstructive pulmonary disease, diabetes mellitus, and metastatic disease considered as FN risk factors by the authors (Online Resource 3).
Outcome assessment
Prophylactic G-CSF was defined as the receipt of ≥ 1 administration of G-CSF from the chemotherapy initiation date up to 5 days following the last chemotherapy administration in the first cycle. Short-acting G-CSFs (sG-CSFs; filgrastim, filgrastim-sndz, and tbo-filgrastim) were identified using established Healthcare Common Procedure Coding System (HCPCS) and National Drug Code (NDC) numbers (Online Resource 6). Number of prophylactic sG-CSF administrations was defined as number of days with sG-CSF claims during the entire cycle; multiple claims on the same day were considered a single administration. NDC and Current Procedural Terminology (CPT) codes were used to distinguish between two modes of pegfilgrastim administration: prefilled syringe (PFS) and on-body injector (OBI) (Online Resource 7). The OBI is applied to the patient’s abdomen or arm on the same day as chemotherapy to automatically deliver pegfilgrastim approximately 27 h after application. Claims with HCPCS codes for pegfilgrastim alone were categorized as “pegfilgrastim, route unknown.” Timing for administration of prophylactic pegfilgrastim PFS or OBI was identified by a claim for pegfilgrastim PFS or OBI relative to day 0 (i.e., same day as chemotherapy completion) through day 5 after chemotherapy completion. Use of prophylactic G-CSF in the second and all subsequent cycles was defined similarly. For each eligible patient in the study cohort, the number of completed chemotherapy cycles (i.e., cycles identified within a course) up to 8 was identified.
Statistical analysis
Descriptive statistics for continuous variables included mean and standard deviation (SD) and median and interquartile range (quartile 1 [Q1] and quartile 3 [Q3]), and categorical variables included count (n) and percentages (%) with 95% binomial confidence intervals (CIs). Standardized differences were calculated to compare age, sex, and comorbidities of patients receiving versus not receiving G-CSF. Results were stratified by calendar year, cancer type, and risk category of the chemotherapy regimen. Prophylactic G-CSF use was assessed by number and proportion across all cycles during the chemotherapy course. The mean (SD) number of prophylactic sG-CSF administrations per cycle was calculated using all eligible cycles that received ≥ 1 administration of prophylactic sG-CSF.
During the post-OBI approval period (i.e., after March 1, 2015), persistence of prophylactic pegfilgrastim was calculated for PFS and OBI following chemotherapy completion. Among patients who received prophylactic pegfilgrastim in the first cycle, persistence of prophylactic pegfilgrastim was calculated as proportion of patients completing 100% of their cycles (up to 8 cycles) with the same type of pegfilgrastim they used in first cycle.
Results
The source population from which patients with the 5 cancer types were identified ranged from 13.3 million in 2013 to 16.4 million in 2017. A total of 22,868 cancer patients (11,513 breast; 4273 lung; 3765 colorectal; 2030 NHL; and 1287 ovarian) met the study inclusion criteria (Online Resource 8). Among these patients, 36.8% were receiving chemotherapy regimens with high FN risk and 63.2% were receiving chemotherapy regimens with intermediate FN risk (among these, 64.4% had ≥ 1 FN risk factor) (Online Resource 8). Chemotherapy regimens with high FN risk were most common in breast cancer patients (71.8%) compared with ≤ 6% for patients with other cancer types (Online Resource 8).
Overall and across cancer types among patients receiving chemotherapy with high FN risk, comorbidity profiles were similar between those who received versus those who did not receive prophylactic G-CSF (Table 1, Online Resource 8). Among all patients with intermediate FN risk (35.0% versus 20.2%) and intermediate FN risk with ≥ 1 risk factor (53.0% versus 33.6%), those not receiving prophylactic G-CSF were more likely to have a baseline metastatic diagnosis compared to patients receiving prophylactic G-CSF. The high likelihood of baseline metastasis for patients not receiving prophylactic G-CSF and receiving chemotherapy regimens with intermediate FN risk was observed only for breast cancer but was not evident among other cancer types (Table 1, Online Resource 8).
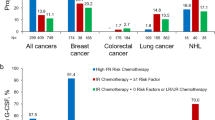
Proportions of patients receiving prophylactic G-CSF in the first cycle were 76.1%, 28.2%, and 26.4% for patients receiving chemotherapy with high risk, intermediate risk, or intermediate risk for FN with ≥ 1 risk factor, respectively (Fig. 1, Online Resource 8). Prophylactic G-CSF use among patients receiving chemotherapy regimens with intermediate FN risk versus those receiving chemotherapy regimens with intermediate FN risk with ≥ 1 risk factor was similar across the 5 cancer types.

Proportion of eligible patients receiving prophylactic G-CSF in the first cycle, stratified by the FN risk category of the chemotherapy regimen and cancer type. Error bars are 95% confidence intervals. FN febrile neutropenia, HR chemotherapy regimen with high FN risk, IR chemotherapy regimen with intermediate FN risk, IR + ≥ 1RF chemotherapy regimen with intermediate FN risk and ≥ 1 patient-level risk factor, N/A not applicable because patients diagnosed with colorectal cancer did not receive any chemotherapy regimen with high FN risk, NHL non-Hodgkin lymphoma, PP-G-CSF primary prophylactic-granulocyte colony–stimulating factor
Among patients receiving prophylactic G-CSF, ≥ 96% were administered pegfilgrastim and this remained unchanged over the study period (Fig. 2, Online Resource 9). Prophylactic pegfilgrastim use was similar across patients receiving chemotherapy regimens with high (98.0%), intermediate (94.7%), and intermediate FN risk with ≥ 1 risk factor (94.4%). Use of the OBI formulation increased to 44.9% by 2017 (42.3% of use could not be classified as either PFS or OBI) (Fig. 2). Among patients receiving prophylactic sG-CSFs, biosimilar filgrastim use increased to ≥ 70% by the end of the time period. Filgrastim use decreased from 100% in 2013 to 26.2% in 2017, with an increase in filgrastim-sndz and tbo-filgrastim use (Fig. 2). Overall, there was no major difference between mean number of administrations per cycle for filgrastim (3.2 [SD 2.3]), filgrastim-sndz (3.0 [SD 1.6), and tbo-filgrastim (4.3 [SD 2.5]) (Online Resource 9).

Proportion of prophylactic G-CSF use by type among patients receiving chemotherapy with high/intermediate FN risk and prophylactic G-CSF in the first cycle by calendar year, and by G-CSF type (a), Pegfilgrastim type (b), and sG-CSF type (c). aRoute unknown: pegfilgrastim users who could not be classified as pegfilgrastim PFS or OBI. FN febrile neutropenia, G-CSF granulocyte colony–stimulating factor, OBI on-body injector, PFS prefilled syringe, prophylactic G-CSF primary prophylaxis G-CSF, sG-CSF short-acting G-CSF
Among cancer patients receiving chemotherapy regimens with high FN risk and prophylactic pegfilgrastim (Fig. 3), 60.6% (95% CI 57.4%, 63.8%) of patients receiving prophylactic pegfilgrastim with the OBI in the first cycle completed all their cycles in their course with the OBI (i.e., persistence); however, only 52.2% (95% CI 48.3%, 56.1%) of patients receiving prophylactic pegfilgrastim with the PFS in the first cycle completed all their cycles in their course with the PFS. These findings were largely driven by the breast cancer population. There were no material differences in completion rates across the two formulations among patients receiving chemotherapy regimens with intermediate FN risk (Online Resource 10).

Proportion of patients completing all cycles in their chemotherapy course with prophylactic pegfilgrastim (i.e., persistence), stratified by pegfilgrastim type and FN risk category of the chemotherapy regimen (March 1, 2015, to December 31, 2017). FN febrile neutropenia, HR chemotherapy regimen with high FN risk, IR chemotherapy regimen with intermediate FN risk, IR + ≥ 1RF chemotherapy regimen with intermediate FN risk and ≥ 1 patient-level risk factor, NHL non-Hodgkin lymphoma, OBI pegfilgrastim on-body injector, PFS pegfilgrastim prefilled syringe, prophylactic pegfilgrastim primary prophylaxis pegfilgrastim
Overall, among all patient cycles receiving pegfilgrastim prophylaxis, the proportion of patient cycles receiving pegfilgrastim on the same day as completion of chemotherapy with high/intermediate FN risk was 9% for pegfilgrastim PFS and 0% for pegfilgrastim OBI (Fig. 4). The proportion of patients receiving pegfilgrastim PFS on the same day was highest for the first cycle (13.2%) and declined in the subsequent cycles to 2.8% in cycle 8 (Online Resource 11).

Day of pegfilgrastim administration following chemotherapy completion by mode of delivery and FN risk category of the chemotherapy regimen. On-body injector automatically administers pegfilgrastim at 27 h after application. aClaims appearing before chemotherapy completion date (i.e., day 0) but after chemotherapy initiation were considered primary prophylactic and were 0.2%. FN febrile neutropenia
Discussion
Using data from a nationally representative population with commercial and Medicare Advantage insurance, we describe the use of G-CSF prophylaxis in 5 cancer types treated with chemotherapy regimens with high/intermediate FN risk in clinical practice. We found that 76% of patients receiving chemotherapy regimens with high FN risk were receiving prophylactic G-CSF, but only 28% of patients receiving regimens with intermediate FN risk received prophylactic G-CSF. Presence of ≥ 1 patient risk factor for FN among patients receiving regimens with intermediate FN risk did not seem to affect the decision to provide prophylaxis. During the study period, > 95% of patients received long-acting G-CSF, with a steady increase in the use of the OBI delivery device. Patients with breast cancer were most likely to receive chemotherapy regimens with high FN risk. In this population, users of the OBI delivery device were more likely to complete all their chemotherapy cycles with pegfilgrastim compared to users of the PFS. During the study period, biosimilar sG-CSF use increased steadily, with filgrastim-sndz accounting for most of the sG-CSF use by the end 2017.
Our results are consistent with prior studies that reported suboptimal use of prophylactic G-CSF [24, 25]. Ramsey and colleagues linked the Western Washington State Surveillance, Epidemiology, and End Results (SEER) registry data with data from 4 major insurers (Medicare, Medicaid, Premera Blue Cross, and Regence Blue Shield) for patients treated for breast cancer, non-small cell lung cancer, and colorectal cancer from 2002 to 2005 [24]. They observed prophylactic G-CSF use of 33% and 10% among patients receiving high risk FN chemotherapy and intermediate FN risk chemotherapy, respectively. In a retrospective cohort study using a 20% Medicare sample from 2007 to 2011, Sosa and colleagues observed that 74% of breast cancer patients and 62% of NHL patients receiving high FN risk chemotherapy received prophylactic G-CSF in the first cycle [25]. In their study, prophylactic G-CSF use among patients receiving intermediate FN risk chemotherapy was 10% for breast cancer and 20% for lung cancer patients. The relatively higher use of prophylactic G-CSF among patients receiving high FN risk chemotherapy observed in our study and in the study by Sosa and colleagues compared to the older study by Ramsey et al. is a reflection of the gradual increase in use of prophylactic G-CSF since 2002, primarily due to the introduction of pegfilgrastim [26].
Uniquely, in our study, we observed that eligible patients not receiving prophylaxis were not dissimilar from patients who received prophylactic G-CSF in terms of age and major comorbidities. The only difference we observed was a higher proportion of metastatic diagnosis among breast cancer patients treated with chemotherapy regimens with intermediate FN risk and not receiving prophylactic G-CSF compared to those receiving G-CSF. Treatment for metastatic patients is usually palliative and focused on improving quality of life, and the evidence of impact of dose intensity on patient outcomes is not conclusive [27]. This may explain the lower proportion of metastatic diagnosis among patients receiving prophylactic G-CSF, which aligns with prior observational studies [28] and shows oncologists’ adherence to American Society of Clinical Oncology guidelines on prophylactic G-CSF use in the metastatic setting [29]. We also observed that patients receiving chemotherapy regimens with intermediate FN risk chemotherapy and ≥ 1 risk factor did not have a higher use of G-CSF compared to patients receiving chemotherapy regimens with intermediate FN risk. This finding demonstrates a need for wider dissemination of the NCCN® guidelines that recommend consideration of G-CSF use among patients receiving chemotherapy regimens with intermediate risk for FN with ≥ 1 risk factor.
Patients who continue to be persistent with pegfilgrastim in subsequent cycles of a chemotherapy course have a lower risk for developing FN than those who discontinue early [30, 31]. In a non-inferiority randomized trial of early breast cancer patients receiving a chemotherapy regimen with high FN risk, Aarts and colleagues [30] found a more than 3-fold higher incidence of FN (36% versus 10%) among patients assigned to receive pegfilgrastim for the first 2 cycles only compared to those who received pegfilgrastim through all 6 cycles. Consequently, it is important to understand if novel pegfilgrastim delivery devices such as the OBI [17] offer any persistent benefit to high FN risk patients compared to the traditional PFS delivery. In breast cancer patients receiving chemotherapy regimens with high FN risk, we observed an 8.5% increase in patients who completed all their cycles with pegfilgrastim support if they started with pegfilgrastim OBI (60.4%) compared to pegfilgrastim PFS (51.9%).
Similar to our findings, prior studies reported considerable proportions of patients receiving same-day administration of PFS [32, 33]. In a retrospective cohort study using 2 large commercial claims databases from 2003 to 2011, Weycker and colleagues reported that among primary solid tumor and NHL patients receiving pegfilgrastim PFS prophylaxis (n = 37,095), PFS was administered on the same day as chemotherapy completion in 12% of the cycles [32]. A follow-up study by the same investigators using the same databases from 2010 to 2015 but restricted to chemotherapy regimens with high/intermediate risk for FN reported that 8% of the 21,7273 cycles received pegfilgrastim on the same day as chemotherapy completion [33]. In our study, we observed that 9% of all cycles received pegfilgrastim PFS on the same day, with almost no pegfilgrastim use via OBI administration occurring on the same day. Note that the claim for OBI application appears in the database on the same day as chemotherapy completion and the automatic administration of pegfilgrastim occurs 27 h after the application. Uniquely, we observed same-day administration was highest in the first cycle and decreased in subsequent cycles in our study. Given the increased risk for FN associated with same-day administration of pegfilgrastim [32,33,34] and the increased risk for FN in the first cycle compared to subsequent cycles [35], an automated OBI that can deliver pegfilgrastim in the ideal time window can alleviate travel burden and fulfill an unmet need for these patients. Future studies are needed to quantify the FN risk reduction resulting from the improved persistence and appropriately timed pegfilgrastim administration offered by novel drug delivery devices.
In recent years, biosimilars for both filgrastim (filgrastim-sndz and filgrastim-aafi) [12, 13] and pegfilgrastim (pegfilgrastim-jmdb and pegfilgrastim-cbqv) [15, 16] and an original sG-CSF (tbo-filgrastim) [14] have been approved and marketed in the USA. The increasing adoption of filgrastim biosimilars including filgrastim-sndz and tbo-filgrastim observed in our study aligns with the timeline and proportions presented in previous publications using Anthem administrative claims [36] and Medicare databases [37]. The (mean [SD]) administration days of prophylactic filgrastim (3.2 [2.3]) observed in our study was higher than that reported by Schwartzberg et al. [38] (2.1 [1.4]), but lower than that reported by Naeim et al. [39] (4.8 [3.3]). Schwartzberg et al. used information from the Optum™ database between March 2015 and June 2016 and did not restrict their study to NCCN®-recommended chemotherapy regimens with high/intermediate FN risk; the lower mean observed in their study could be a result of capturing all possible instances of prophylactic filgrastim use. Nevertheless, patients in real-world settings are receiving shorter duration of sG-CSF compared to the 10–11 days suggested by non-inferiority studies comparing filgrastim with pegfilgrastim [40, 41]. To our knowledge, this is the first study to describe the increasing use of novel delivery devices such as OBI among patients receiving chemotherapy regimens with high/intermediate FN risk. By 2017, of all patients that received prophylactic pegfilgrastim, 12.8% received PFS, 44.9% received OBI, and 42.3% received pegfilgrastim by an unknown mode of delivery.
Several limitations need to be considered for our study. First, the administrative claims database we used did not include patient-level risk factors for FN, such as persistent neutropenia, bone marrow involvement by tumor, recent surgery and/or open wounds, or poor performance status. Other determinants of prophylactic G-CSF use, such as practice-level guidelines, therapeutic intent, or patient preferences, were also unavailable in the claims database. We included type 2 diabetes, cardiovascular disease, chronic obstructive pulmonary disease, and baseline metastasis based on expert guidance as patient-level risk factors, although these are not included in the NCCN® list of risk factors. Nevertheless, the presence of ≥ 1 risk factor did not increase an eligible patient’s likelihood of receiving prophylactic G-CSF compared to a broader subgroup of patients receiving a chemotherapy regimen with intermediate FN risk. Secondly, we were unable to accurately discriminate a portion of pegfilgrastim users as PFS or OBI after the launch date of the OBI (March 1, 2015) because of the lack of a specific J-code for the OBI. If the ratio of OBI:PFS in 2017 in the pegfilgrastim route unknown subgroup is similar to the ratio of the pegfilgrastim route known subgroup (45:13), OBI would make up 78% of all pegfilgrastim administrations in 2017. Thirdly, chemotherapy dose is not described in the claims database, which may have resulted in inclusion of patients with reduced dose intensity (i.e., ineligible for prophylactic G-CSF) in the subgroups, thus leading to an underestimation of prophylactic G-CSF use. Assuming chemotherapy dose reduction occurs more frequently in later cycles, we expect minimal underestimation of prophylactic G-CSF use from our definition in the first cycle in this study. Fourthly, we included patients only until August 31, 2017. This limited the follow-up period to capture treatment in later cycles for patients entering the cohort near the end of the inclusion period, effectively reducing the precision of our estimates. While this study provides important data on chemotherapy and prophylactic G-CSF use in patients with various tumors, it was not able to determine the reasons for cycle interruptions. It is hypothesized that a non-trivial proportion may be due to FN but further research is needed to better understand this multi-factorial process. Finally, the population in this study was obtained from a nationally representative insurer but the results may not generalize to patients with Medicare or for patients without insurance.
In conclusion, the results from this nationally representative database demonstrate that cancer patients at high risk for FN may be vulnerable because of under- or mistimed use of prophylactic G-CSF. Future studies are required to understand the reasons for G-CSF underutilization and quantify the FN risk reduction resulting from improved persistence and appropriately timed dosing of pegfilgrastim administered through a novel delivery device compared to pegfilgrastim administered through the PFS.
References
Brahmer JR, Tykodi SS, Chow LQ, Hwu WJ, Topalian SL, Hwu P, Drake CG, Camacho LH, Kauh J, Odunsi K, Pitot HC, Hamid O, Bhatia S, Martins R, Eaton K, Chen S, Salay TM, Alaparthy S, Grosso JF, Korman AJ, Parker SM, Agrawal S, Goldberg SM, Pardoll DM, Gupta A, Wigginton JM (2012) Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N Engl J Med 366:2455–2465
June CH, Sadelain M (2018) Chimeric antigen receptor therapy. N Engl J Med 379:64–73
Kantarjian H, Stein A, Gokbuget N, Fielding AK, Schuh AC, Ribera JM, Wei A, Dombret H, Foà R, Bassan R, Arslan Ö, Sanz MA, Bergeron J, Demirkan F, Lech-Maranda E, Rambaldi A, Thomas X, Horst HA, Brüggemann M, Klapper W, Wood BL, Fleishman A, Nagorsen D, Holland C, Zimmerman Z, Topp MS (2017) Blinatumomab versus chemotherapy for advanced acute lymphoblastic leukemia. N Engl J Med 376:836–847
Marquart J, Chen EY, Prasad V (2018) Estimation of the percentage of US patients with cancer who benefit from genome-driven oncology. JAMA Oncol 4:1093–1098
Baldo P, Fornasier G, Ciolfi L, Sartor I, Francescon S (2018) Pharmacovigilance in oncology. Int J Clin Pharm 40:832–841
Dale DC (2002) Colony-stimulating factors for the management of neutropenia in cancer patients. Drugs 62(Suppl 1):1–15
Tai E, Guy GP, Dunbar A, Richardson LC (2017) Cost of cancer-related neutropenia or fever hospitalizations, United States, 2012. J Oncol Pract 13:e552–e561
Aapro MS, Bohlius J, Cameron DA, Dal Lago L, Donnelly JP, Kearney N, Lyman GH, Pettengell R, Tjan-Heijnen VC, Walewski J, Weber DC, Zielinski C (2011) 2010 update of EORTC guidelines for the use of granulocyte-colony stimulating factor to reduce the incidence of chemotherapy-induced febrile neutropenia in adult patients with lymphoproliferative disorders and solid tumours. Eur J Cancer 47:8–32
Kuderer NM, Dale DC, Crawford J, Lyman GH (2007) Impact of primary prophylaxis with granulocyte colony-stimulating factor on febrile neutropenia and mortality in adult cancer patients receiving chemotherapy: a systematic review. J Clin Oncol 25:3158–3167
NCCN® Clinical Practice Guidelines in Oncology. Hematopoietic growth factors. V2.2019. National Comprehensive Cancer Network website. https://www.nccn.org/professionals/physician_gls/pdf/growthfactors.pdf. Accessed 4 June 2019
Centers for Medicare and Medicaid Services. Oncology Care Model. https://innovation.cms.gov/initiatives/oncology-care/. Accessed 4 June 2019
Food and Drug Administration. Filgrastim-sndz [prescribing information]. https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/125553lbl.pdf. Accessed 4 June 2019
Food and Drug Administration. Filgrastim-aafi [prescribing information]. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/761080s000lbl.pdf. Accessed 4 June 2019
Food and Drug Administration. Tbo-filgrastim [prescribing information]. http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/125294s0000lbl.pdf. Accessed 4 June 2019
Food and Drug Administration. Pegfilgrastim-jmdb [prescribing information]. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/761075s000lbl.pdf. Accessed 4 June 2019
Food and Drug Administration. Pegfilgrastim-cbqv [prescribing information]. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/761039s000lbl.pdf. Accessed 4 June 2019
Food and Drug Administration. Pegfilgrastim [prescribing information]. https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/125031s180lbl.pdf. Accessed 4 June 2019
Seeger J, Daniel GW (2012) PART III sources of data for pharmacoepidemiologic studies. Commercial insurance databases. In: Storm BL, Kimmel SE, Hennessy S (eds) Pharmacoepidemiology. Wiley-Blackwell, Hoboken, pp 189–208
Optum™ Optum Clinformatics Data Mart. https://www.optum.com/content/dam/optum/resources/productSheets/Clinformatics_for_Data_Mart.pdf. Accessed 10 October 2018
Crawford J, Becker PS, Armitage JO, Blayney DW, Chavez J, Curtin P, Dinner S, Fynan T, Gojo I, Griffiths EA, Hough S, Kloth DD, Kuter DJ, Lyman GH, Mably M, Mukherjee S, Patel S, Perez LE, Poust A, Rampal R, Roy V, Rugo HS, Saad AA, Schwartzberg LS, Shayani S, Talbott M, Vadhan-Raj S, Vasu S, Wadleigh M, Westervelt P, Burns JL, Pluchino L (2017) Myeloid growth factors, Version 2.2017, NCCN clinical practice guidelines in oncology. J Natl Compr Cancer Netw 15:1520–1541
Hebert PL, Geiss LS, Tierney EF, Engelgau MM, Yawn BP, McBean AM (1999) Identifying persons with diabetes using Medicare claims data. Am J Med Qual 14:270–277
Quan H, Li B, Couris CM, Fushimi K, Graham P, Hider P, Januel JM, Sundararajan V (2011) Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol 173:676–682
Klabunde CN, Legler JM, Warren JL, Baldwin LM, Schrag D (2007) A refined comorbidity measurement algorithm for claims-based studies of breast, prostate, colorectal, and lung cancer patients. Ann Epidemiol 17:584–590
Ramsey SD, McCune JS, Blough DK, McDermott CL, Clarke L, Malin JL, Sullivan SD (2010) Colony-stimulating factor prescribing patterns in patients receiving chemotherapy for cancer. Am J Manag Care 16:678–686
Sosa R, Li S, Molony JT, Liu J, Stryker S, Collins AJ (2017) Use of prophylactic growth factors and antimicrobials in elderly patients with cancer: a review of the Medicare database. Support Care Cancer 25:3123–3132
Goyal RK, Tzivelekis S, Rothman KJ, Candrilli SD, Kaye JA (2018) Time trends in utilization of G-CSF prophylaxis and risk of febrile neutropenia in a Medicare population receiving adjuvant chemotherapy for early-stage breast cancer. Support Care Cancer 26:539–548
Smith TJ, Hillner BE (2012) A way forward on the medically appropriate use of white cell growth factors. J Clin Oncol 30:1584–1587
Baig H, Somlo B, Eisen M, Stryker S, Bensink M, Morrow PK (2018) Appropriateness of granulocyte colony-stimulating factor use in patients receiving chemotherapy by febrile neutropenia risk level. J Oncol Pharm Pract 25:1576. https://doi.org/10.1177/1078155218799859
Smith TJ, Bohlke K, Lyman GH, Carson KR, Crawford J, Cross SJ, Goldberg JM, Khatcheressian JL, Leighl NB, Perkins CL, Somlo G, Wade JL, Wozniak AJ, Armitage JO, Oncology ASoC (2015) Recommendations for the use of WBC growth factors: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol 33:3199–3212
Aarts MJ, Peters FP, Mandigers CM, Dercksen MW, Stouthard JM, Nortier HJ, van Laarhoven HW, van Warmerdam LJ, van de Wouw AJ, Jacobs EM, Mattijssen V, van der Rijt CC, Smilde TJ, van der Velden AW, Temizkan M, Batman E, Muller EW, van Gastel SM, Borm GF, Tjan-Heijnen VC (2013) Primary granulocyte colony-stimulating factor prophylaxis during the first two cycles only or throughout all chemotherapy cycles in patients with breast cancer at risk for febrile neutropenia. J Clin Oncol 31:4290–4296
Weycker D, Bensink M, Wu H, Doroff R, Chandler D (2017) Risk of chemotherapy-induced febrile neutropenia with early discontinuation of pegfilgrastim prophylaxis based on real-world data from 2010 to 2015. Curr Med Res Opin 33:2115–2120
Weycker D, Li X, Figueredo J, Barron R, Tzivelekis S, Hagiwara M (2016) Risk of chemotherapy-induced febrile neutropenia in cancer patients receiving pegfilgrastim prophylaxis: does timing of administration matter? Support Care Cancer 24:2309–2316
Weycker D, Bensink M, Lonshteyn A, Doroff R, Chandler D (2017) Risk of chemotherapy-induced febrile neutropenia by day of pegfilgrastim prophylaxis in US clinical practice from 2010 to 2015. Curr Med Res Opin 33:2107–2113
Burris HA, Belani CP, Kaufman PA, Gordon AN, Schwartzberg LS, Paroly WS, Shahin S, Dreiling L, Saven A (2010) Pegfilgrastim on the same day versus next day of chemotherapy in patients with breast cancer, non-small-cell lung cancer, ovarian cancer, and non-Hodgkin’s lymphoma: results of four multicenter, double-blind, randomized phase II studies. J Oncol Pract 6:133–140
Lyman GH, Kuderer NM (2003) Epidemiology of febrile neutropenia. Support Cancer Ther 1:23–35
Chen X, Agiro A, Barron J, Debono D, Fisch M (2018) Early adoption of biosimilar growth factors in supportive cancer care. JAMA Oncol 4:1779–1781
Kozlowski S, Birger N, Brereton S, McKean SJ, Wernecke M, Christl L, Kelman JA (2018) Uptake of the biologic filgrastim and its biosimilar product among the Medicare population uptake of the biologic filgrastim and its biosimilar among the Medicare population letters. JAMA 320:929–931
Schwartzberg LS, Lal LS, Balu S, Campbell K, Brekke L, DeLeon A, Elliott C, Korrer S (2018) Clinical outcomes of treatment with filgrastim versus a filgrastim biosimilar and febrile neutropenia-associated costs among patients with nonmyeloid cancer undergoing chemotherapy. J Manag Care Spec Pharm 24:976–984
Naeim A, Henk HJ, Becker L, Chia V, Badre S, Li X, Deeter R (2013) Pegfilgrastim prophylaxis is associated with a lower risk of hospitalization of cancer patients than filgrastim prophylaxis: a retrospective United States claims analysis of granulocyte colony-stimulating factors (G-CSF). BMC Cancer 13:11
Holmes FA, O'Shaughnessy JA, Vukelja S, Jones SE, Shogan J, Savin M, Glaspy J, Moore M, Meza L, Wiznitzer I, Neumann TA, Hill LR, Liang BC (2002) Blinded, randomized, multicenter study to evaluate single administration pegfilgrastim once per cycle versus daily filgrastim as an adjunct to chemotherapy in patients with high-risk stage II or stage III/IV breast cancer. J Clin Oncol 20:727–731
Green MD, Koelbl H, Baselga J, Galid A, Guillem V, Gascon P, Siena S, Lalisang RI, Samonigg H, Clemens MR, Zani V, Liang BC, Renwick J, Piccart MJ, Group IPS (2003) A randomized double-blind multicenter phase III study of fixed-dose single-administration pegfilgrastim versus daily filgrastim in patients receiving myelosuppressive chemotherapy. Ann Oncol 14:29–35
Acknowledgments
The authors are grateful for the programming support provided by Corina Bennett of Amgen Inc. and Renee Jaramillo of Simulstat, and the medical writing support provided by Martha Mutomba (on behalf of Amgen Inc.) and Peter Alexander of Amgen Inc.
Funding
This study was supported by Amgen Inc.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Prasad L. Gawade and Michael A. Kelsh collected and analyzed the data, and all authors participated in the interpretation of the data. Prasad L. Gawade wrote the first draft of the manuscript and all authors commented on versions during the development of the manuscript. All authors read and approved the final manuscript for submission to Supportive Care in Cancer.
Corresponding author
Ethics declarations
Conflict of interest
Prasad L. Gawade, Brian D. Bradbury, Rajesh Belani, and Michael A. Kelsh are employees of and own stock in Amgen Inc. Nancy Smith was an employee of DOCS Global and was contracted to work with Amgen Inc. during the period of this study. Shuling Li is an employee of Chronic Disease Research Group, Hennepin Healthcare Research Institute, which has received project funding from Amgen Inc. David Henry has received honoraria for serving on an advisory board for Amgen Inc.
Research involving human participants and/or animals
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
Formal consent was not required as the article does not contain any studies involving human participants performed by any of the authors..
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(PDF 510 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gawade, P.L., Li, S., Henry, D. et al. Patterns of granulocyte colony–stimulating factor prophylaxis in patients with cancer receiving myelosuppressive chemotherapy. Support Care Cancer 28, 4413–4424 (2020). https://doi.org/10.1007/s00520-020-05295-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-020-05295-2