
Summary
Background
Traditional risk factors for cardiovascular disease (CVD) play an important role in the clinical evaluation of patients with symptoms suggestive of coronary artery disease (CAD). The utility of the diagonal earlobe crease (DELC) in predicting the presence of CAD is controversial.
Purpose
To investigate the association between DELC, traditional CVD risk factors, and obstructive CAD.
Methods
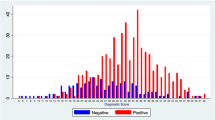
This prospective study included 1377 patients (mean age 65 ± 10 years, 64% male) who underwent invasive coronary angiography for suspected acute or chronic coronary syndromes. In addition to routine clinical assessment, all patients underwent visual examination of both earlobes for the presence of DELC. All assessments were made by three independent readers, with a majority vote in the case of disagreement. Obstructive CAD was defined by invasive coronary angiography as > 50% stenosis of the left main coronary artery or > 70% stenosis in any other major epicardial coronary artery.
Results
Bilateral DELC was observed more frequently in patients with obstructive CAD than in those without it (67% vs. 33%, p = 0.022). In the multivariate logistic regression model, bilateral DELC was independently associated with CAD (odds ratio [OR] 1.36, 95% confidence interval [CI] 1.07–1.74), along with smoking (OR 1.86, 95% CI 1.44–2.38), diabetes mellitus (OR 1.67, 95% CI 1.29–2.15), male sex (OR 2.04, 95% CI 1.61–2.58), and dyslipidemia (OR 1.54, 95% CI 1.12–2.30); however, the diagnostic accuracy of DELC was modest and resembled that of traditional CVD risk factors.
Conclusion
Despite being independently associated with obstructive CAD, DELC is not a reliable stand-alone clinical marker of CAD due to modest diagnostic accuracy.




Similar content being viewed by others


References
Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. GBD-NHLBI-JACC Global Burden of Cardiovascular Diseases Writing Group. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J Am Coll Cardiol. 2020;76(25):2982–3021.
Holthuis EI, Visseren FLJ, Bots ML, Peters SAE, UCC-SMART study group on behalf of the. Risk Factor Clusters and Cardiovascular Disease in High-Risk Patients: The UCC-SMART Study. Global Heart. 2021;16(1):85.
van Bussel EF, Hoevenaar-Blom MP, Poortvliet RKE, Gussekloo J, van Dalen JW, van Gool WA, Richard E, Moll van Charante EP. Predictive value of traditional risk factors for cardiovascular disease in older people: A systematic review. Prev Med. 2020;132:105986.
Vaes B, Indestege P, Serneels T, Hegendörfer E, van Peet PG, Poortvliet RKE, Wallemacq P, Gussekloo J, Degryse J. Biomarkers versus traditional risk factors to predict cardiovascular events in very old adults: cross-validated prospective cohort study. Bmj Open. 2020;10(6):e35809.
Karmali KN, Persell SD, Perel P, Lloyd-Jones DM, Berendsen MA, Huffman MD. Risk scoring for the primary prevention of cardiovascular disease. Cochrane Database Syst Rev. 2017;3(3):CD6887.
Frank ST. Aural Sign of Coronary-Artery Disease. N Engl J Med. 1973;289:327–8.
Lucenteforte E, Romoli M, Zagli G, Gensini GF, Mugelli A, Vannacci A. Ear lobe crease as a marker of coronary artery disease: a meta-analysis. Int J Cardiol. 2014;175(1):171–5.
Więckowski K, Gallina T, Surdacki A, Chyrchel B. Diagonal Earlobe Crease (Frank’s Sign) for Diagnosis of Coronary Artery Disease: A Systematic Review of Diagnostic Test Accuracy Studies. J Clin Med. 2021;10(13):2799.
Maddox TM, Stanislawski MA, Grunwald GK, Bradley SM, Ho PM, Tsai TT, Patel MR, Sandhu A, Valle J, Magid DJ, Leon B, Bhatt DL, Fihn SD, Rumsfeld JS. Nonobstructive coronary artery disease and risk of myocardial infarction. JAMA. 2014;312(17):1754–63.
Verma SK, Khamesra R, Bordia A. Ear-lobe crease and ear-canal hair as predictors of coronary artery disease in Indian population. Indian J Chest Dis Allied Sci. 1988;30:189–96.
Hou X, Jiang Y, Wang N, Shen Y, Wang X, Zhong Y, Xu P, Zhou L. The Combined Effect of Ear Lobe Crease and Conventional Risk Factor in the Diagnosis of Angiographically Diagnosed Coronary Artery Disease and the Short-Term Prognosis in Patients Who Underwent Coronary Stents. Medicine. 2015;94:e815.
Lichstein E, Chadda KD, Naik D, et al. Diagonal ear-lobe crease: prevalence and implications as a coronary risk factor. N Engl J Med. 1974;290:615–6.
Liu Z, Qiu C, Xu J, Zhang Y, Cui Q, Guan G, Pan S. Ear Crease Features Are Associated with Complexity of Coronary Lesions. Med Sci Monit. 2020;26:e923343.
Wang Y, Mao L, Jia E, et al. Relationship between diagonal earlobe creases and coronary artery disease as determined via angiography. Bmj Open. 2016;6:e8558.
Brady PM, Zive MA, Goldberg RJ, Gore JM, Dalen JE. A New Wrinkle to the Earlobe Crease. Arch Intern Med. 1987;147:65–6.
Faxas E, Vigoa A, Chuckram A, Valdés R, Fariñas H. Earlobe crease and ischemic heart disease. Rev Cubana Med. 1995;34:14–21.
Brady PM, Zive MA, Goldberg RJ, Gore JM, Dalen JE. A New Wrinkle to the Earlobe Crease. Arch Intern Med. 1987;147(1):65–6.
Kaukola S. The diagonal ear-lobe crease, a physical sign associated with coronary heart disease. Acta Med Scand Suppl. 1978;619:1–49.
Higuchi Y, Maeda T, Guan JZ, Oyama J, Sugano M, Makino N. Diagonal earlobe crease are associated with shorter telomere in male Japanese patients with metabolic syndrome. Circ J. 2009;73(2):274–9.
Rossiello F, Jurk D, Passos JF, d’Adda di Fagagna F. Telomere dysfunction in ageing and age-related diseases. Nat Cell Biol. 2022;24(2):135–147.
Peppa M, Uribarri J, Vlassara H. Glucose, Advanced Glycation End Products, and Diabetes Complications: What Is New and What Works. Clin Diabetes. 2003;21(4):186–7.
Hamlin CR, Kohn RR, Luschin JH. Apparent Accelerated Aging of Human Collagen in Diabetes Mellitus. Diabetes. 1975;24(10:902–4.
Morita A. Tobacco smoke causes premature skin aging. J Dermatol Sci. 2007;48(3):169–75.
Kennedy C, Bastiaens MT, Bajdik CD, Willemze R, Westendorp RG, Bouwes Bavinck JN. Leiden Skin Cancer Study. Effect of smoking and sun on the aging skin. J Invest Dermatol. 2003;120(4:548–54.
Eriksson D, Khoshnood A, Larsson D, Lundager-Forberg J, Mokhtari A, Ekelund U. Diagnostic Accuracy of History and Physical Examination for Predicting Major Adverse Cardiac Events Within 30 Days in Patients With Acute Chest Pain. J Emerg Med. 2020;58(1):1–10.
Lin S, Li Z, Fu B, Chen S, Li X, Wang Y, Wang X, Lv B, Xu B, Song X, Zhang YJ, Cheng X, Huang W, Pu J, Zhang Q, Xia Y, Du B, Ji X, Zheng Z. Feasibility of using deep learning to detect coronary artery disease based on facial photo. Eur Heart J. 2020;41(46):4400–11.
Özbilgin F, Kurnaz Ç, Aydın E. Prediction of Coronary Artery Disease Using Machine Learning Techniques with Iris Analysis. Diagnostics. 2023;13(6):1081.
Vashi NA, de Castro Maymone MB, Kundu RV. Aging Differences in Ethnic. Skin J Clin Aesthet Dermatol. 2016;9(1):31–8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
B. Gakovic, S.A. Neskovic, I. Vranic, K. Grujicic, S. Mijatovic, A. Ljubojevic and I. Stankovic declare that they have no competing interests.
Ethical standards
All procedures performed in studies involving human participants or on human tissue were in accordance with the ethical standards of the institutional and/or national research committee and with the 1975 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Gakovic, B., Neskovic, S.A., Vranic, I. et al. The relationship of diagonal earlobe crease (Frank’s sign) and obstructive coronary artery disease in patients undergoing coronary angiography. Wien Klin Wochenschr 135, 667–673 (2023). https://doi.org/10.1007/s00508-023-02297-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00508-023-02297-y