
Abstract
Background
Although several studies on telesurgery have been reported globally, a clinically applicable technique has not yet been developed. As part of a telesurgical study series conducted by the Japan Surgical Society, this study describes the first application of a double-surgeon cockpit system to telesurgery.
Methods
Surgeon cockpits were installed at a local site and a remote site 140 km away. Three healthy pigs weighing between 26 and 29 kg were selected for surgery. Non-specialized surgeons performed emergency hemostasis, cholecystectomy, and renal vein ligation with remote assistance using the double-surgeon cockpits and specialized surgeons performed actual telesurgery. Additionally, the impact of adding internet protocol security (IPsec) encryption to the internet protocol-virtual private network (IP-VPN) line on communication was evaluated to address clinical security concerns.
Results
The average time required for remote emergency hemostasis with the double-surgeon cockpit system was 10.64 s. A non-specialized surgeon could safely perform cholecystectomy or renal vein ligation with remote assistance. Global Evaluative Assessment of Robotic Skills and System Usability Scale scores were higher for telesurgical support-assisted surgery by a non-specialized surgeon using the double-surgeon cockpits than for telesurgery performed by a specialized surgeon without the double-cockpit system. Adding IPsec encryption to the IP-VPN did not have a significant impact on communication.
Conclusion
Telesurgical support through our double-surgeon cockpit system is feasible as first step toward clinical telesurgery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Telesurgery comprises robot-assisted surgery performed from a remote location. Telesurgery can be classified into three categories according to the type of remote assistance: telementoring, telesurgical support, and full telesurgery. Telementoring involves simply providing instructions from a remote location, while telesurgical support refers to the use of a robot to assist with surgery, and in full telesurgery, the entire surgery is performed from a remote location. Despite numerous studies conducted worldwide, the application of full telesurgery is not yet possible.
Among the three types of telesurgery, telementoring has recently attracted greater attention, mostly due to the rapid spread of robotic surgery driven by the coronavirus disease 2019 (COVID-19) pandemic. However, the COVID-19 pandemic has also made it difficult for physicians to provide on-site training for robotic surgery [2,3,4] and fulfill the large number of requests for such training. Thus, the need for telementoring and telesurgery has rapidly increased in recent years [5,6,7,8]. Recently, the Society of American Gastrointestinal and Endoscopic Surgeons issued a white paper listing the minimum requirements for telementoring [1]. However, methods for performing actual telesurgery, beyond telementoring, remain unclear.
The Japan Surgical Society (JSS) is currently performing a series of studies to establish the minimum requirements for telesurgery, particularly for the telesurgical support required to perform actual telesurgery [9,10,11]. Through this study series, we aim to introduce telesurgery using a general commercial network instead of a dedicated private or 5th-generation (5G) network. The studies to date have confirmed the bandwidth required to control two types of Japanese surgical-assisted robots [10] and proved that redundancy can be maintained by preparing two-type communication lines as backup [11].
In the present study, we installed two surgeon cockpits, one each at a local and a remote location and to verify the possibility of mentoring the local surgery from a remote location and maintaining effective telementoring and telesurgical support, while the priority operator is switched as needed. Further, we concurrently examined the impact of improving the technology’s security level on communication in an effort to enable its future use by the general public.
Materials and methods
Network connections
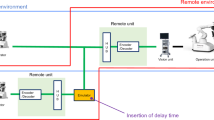
The operating rooms at the Kyushu University Animal Facility in Fukuoka and Beppu Hospital were connected across a 140-km distance through a fiber optic network, which was constructed using a guaranteed-type line (guaranteed bandwidth: 40 Mbps) and a best-effort line as a backup (Fig. 1). These lines were provided by the Nippon Telegraph and Telephone Corporation and established over an internet protocol-virtual private network (IP-VPN). We used the Zao-SH encoder and Zao-View decoder from Soliton Systems KK for compression and decompression, respectively, of the communication information. Guaranteed and best-effort lines were directly connected to the encoder. The decoder was connected to a layer 3 network switch (upper level of the network), which was configured to make the two lines redundant. We constructed encrypted communications using internet protocol security (IPsec) on the IP-VPN for advanced security testing and evaluated the round-trip time, packet size, and frame length.

System configuration diagram. A backup line is prepared to avoid sudden disconnections during telesurgery
Robotic system
We used a pneumatically driven robotic system (Riverfield, Inc., Tokyo, Japan). The robot is shown in Supplementary Fig. S1. This robot is in its final stage of development and is close to meeting production specifications. The developmental process comprised a quality management system process with ISO13485 certification.
The basic concept of the surgical robot is similar to that of the da Vinci surgical system, but differs in several ways. First, the surgical robot has three arms; a third arm is not installed. Second, the surgical console is not immersive, but has an open structure and looks similar to the SenHance Surgical System. Third, while the da Vinci surgical system mechanically restricts ports, our robot uses redundant joint control to realize virtual remote center of motion.
The axes (gimbals 1 and 2) of the holder arm’s wrist and the instrument driver are pneumatically driven, while the other axes are electric. The air pressure of the air cylinders in the instrument driver is monitored using pressure sensors, and the grasping force is estimated by changes in the measured pressure values. The estimated grasping force is fed back to the surgeon console's grip.
Six types of instruments are available, some of which are monopolar compatible.
Similar to that in the da Vinci system, our robot is operated using a hand-held controller to instruct the robot’s movement; however, our robot differs in that the grip is held by the thumb and index finger, and the clutch switch is operated by the middle finger.
We used a 26605AA endoscope (Karl Storz, Tuttlingen, Germany) and CuratOR EX3141-3D display (EIZO, Ishikawa, Japan). Two surgeon cockpits were installed, with one each at the Kyushu University Animal Facility and Beppu Hospital, and the robot was installed at Kyushu University.
Experimental animals
Three healthy pigs, weighing between 26 and 29 kg, were selected for surgery. Procedures were performed with a monopolar electrocautery scalpel, as in standard human surgeries. The animal experiments were carried out humanely, in accordance with the Regulations for Animal Experiments of Kyushu University. All protocols and procedures were approved by the Institutional Animal Experiment Committees of Kyushu University (approval number: A21-462-0).
Evaluation of double-surgeon cockpits for telesurgical support and telementoring
The participating surgeons were preoperatively interviewed regarding their years of surgical experience, training period for laparoscopic surgery, and number of laparoscopic and robotic surgeries performed.
Emergency hemostasis
To create an emergency hemostasis situation, the local surgeon made a mesenteric blood vessel incision. When the local mesenteric site started to bleed, the system forcibly switched the priority operator from the remote location to stop the bleeding. The time required to achieve hemostasis was calculated. Hemostasis time was defined as the time taken by the remote operator to switch the priority surgeon, who then moved the arm to stop the bleeding, followed by the completion of a hemostasis evaluation. Eight remote surgeons performed this procedure twice to determine the hemostasis time. Among the eight surgeons, three had no experience with robotic surgery (beginners) and five had experienced between 10 and 100 cases of robotic surgery (experts) prior to the study initiation.
Telesurgical support using the double-surgeon cockpit system
Three urologists performed cholecystectomies in three pigs, assisted by a gastroenterological surgeon from a remote surgical cockpit. The surgery involved gallbladder duct ligation conducted by the remote gastroenterological surgeon, followed by gallbladder removal by the local urologist. Similarly, three gastroenterological surgeons performed left renal vein ligations in three pigs, assisted by an urologist from a remote location; the urologist delineated the left renal vein from the remote surgeon cockpit and the local gastroenterological surgeon ligated it in each case.
As a control, three urologists and gastroenterological surgeons performed left renal vein ligations and cholecystectomies using gallbladder models, respectively, from the remote surgeon cockpit.
Robot operability in each surgery was evaluated using the System Usability Scale (SUS) [12] and Global Evaluative Assessment of Robotic Skills (GEARS) [13]. In the SUS, 10 items are ranked and converted to a score on a 100-point scale; in the GEARS, six items, including stereopsis and two-hand coordination, are ranked and converted to a score on a 30-point scale.
Statistical analysis
Statistical analysis was performed using JMP 11 software (SAS Institute Japan Ltd., Tokyo, Japan). Continuous variables were evaluated using the Student’s t test. Statistical significance was set at p < 0.05.
Results
Emergency hemostasis experiment (video 1)
The average hemostasis time across all operators was 10.64 s. The average hemostasis time was 9.45 and 12.64 s among the five surgeons with robotic surgery experience (experts) and the three surgeons without such experience (beginners), respectively; the difference was not significant (p = 0.17). Forced switching of the priority surgeon to stop the bleeding is shown in Video 1. A plot of the individual hemostasis times for each of the eight surgeons is provided in Supplementary Fig. S2.
Evaluation of telesurgical support
The three urologists successfully performed cholecystectomies in three pigs, assisted by a gastroenterological surgeon from a remote surgical cockpit (Fig. 2 and Video 2). The operation time ranged from 30 to 85 min. Additionally, the three gastroenterological surgeons successfully performed left renal vein ligations in three pigs, assisted by an urologist from a remote location. The operation time ranged from 30 to 60 min. The average GEARS and SUS scores of the participating surgeons are shown in Fig. 3A and B, respectively. The GEARS and SUS scores were higher for non-specialized surgeons performing the surgery locally with remote assistance than for specialized surgeons performing actual telesurgery.

A Surgeon cockpit at the local site, where an urologist performs cholecystectomy. B Surgeon cockpit at the remote site, 140 km away, where a gastroenterological surgeon assists the urologist

A Robotic skill evaluation on the Global Evaluative Assessment of Robotic Skills. The standard deviation is shown in the graph. The highest possible score is 30 points; a higher score indicates a better robot-operating experience by the surgeon. B Robotic usability evaluation on the System Usability Scale. The standard deviation is shown in the graph. The highest possible score is 50 points; a higher score indicates that the surgeon finds the robot easy to operate
Communication delays and security level verification
In the present study, a general commercial network carrier was used for telecommunication. The bandwidth usage of our robot was reported as 22.0–25.0 Mbps in a previous study; thus, we estimated that a bandwidth of 40 Mbps would be sufficient for a guaranteed line. We examined whether communication delays would occur when adding IPsec communication to the IP-VPN line and performing double encryption. Table 1 summarizes the communication delays and bandwidth usage findings. Figure 4A shows the IP-VPN traffic measurement results without IPsec communication. The communication bandwidth usage was 22.5–25.5 Mbps and did not exceed 33 Mbps; in addition, the average and maximum communication delays were 4.5 and 27 ms, respectively. When IPsec encryption was added, the communication bandwidth usage was 33.0–60.0 Mbps, and the average and maximum communication delays were 12.5 and 37 ms, respectively (Fig. 4B and Table 1).

A Communication capacity values without internet protocol security encryption. The dotted lines indicate the maximum bandwidth usage. B Communication capacity values with internet protocol security encryption. The dotted lines indicate the maximum bandwidth usage
Discussion
Since the first remote surgery was performed in 2001 [14], telesurgery has been gaining attention in Canada and other countries [15,16,17]. However, robot-assisted telesurgery did become widespread until recently. This may be because robot development companies were not actively developing remote surgery, and the quality of surgeries performed on commercial communication lines had deteriorated. Additionally, patients themselves rarely consented to telesurgery, preferring to rather travel several hundred kilometers to undergo surgery. However, the situation has dramatically changed recently. Communication lines have improved, enabling high-speed networks via fiber optic cables in hospitals worldwide. Furthermore, the COVID-19 pandemic restricted travel and movement. Accordingly, robotic surgeries are now becoming more common, with telementoring and telesurgery in increased demand, promoting robotic surgical training in young surgeons.
The JSS is currently taking measures to gradually introduce telesurgery clinically by conducting a study series. In the present study, we examined whether it is possible to remotely assist a surgery, while the priority surgeon is switched between two surgeon cockpits during an animal surgery and demonstrated that telesurgical support is possible using this system. Before telesurgical support can be established, preparing for emergency situations is necessary. Thus, we first examined whether hemostasis could be achieved when forcibly switching the priority surgeon cockpit. The 10.64-s hemostasis time required in this study may be shortened once the surgeon becomes accustomed to using the robot. In our system, the priority surgeon can be switched on the surgeon cockpit’s liquid crystal display (LCD) panel, and by stepping on a clutch once, the surgery can be switched to the remote operator. Issues may arise when the surgeon’s view is forced to leave the surgical field because of switching between views on the LCD panel. Similarly, the da Vinci surgical system also switches the priority operator of a double-cockpit system using the LCD panel, and the surgeon’s view is removed from the surgical field. A simple switching system that does not interrupt the surgical field view is needed.
We selected three pigs for surgery to evaluate our system under surgical conditions. When a non-specialized urologist performed cholecystectomy or a non-specialized gastroenterologist ligated the renal vein, telesurgical support by a specialized surgeon was provided. Additionally, surgical control between the local and remote cockpits was switched at least twice during each surgery. We used the GEARS and SUS as validated assessment tools for grading overall technical proficiency and measuring the ease of usability, respectively, for robotic surgery and found that the average GEARS and SUS scores were better for non-specialized surgery with telesurgical support than for full telesurgery performed by a specialized surgeon. Since these conditions were different, they cannot be considered as appropriate controls. However, all surgeries were performed successfully. Accordingly, telesurgical support may be a realistic option for telesurgery in future.
In addition, we considered the impact of cryptographic communication, which is necessary for clinical introduction. Telesurgery is performed better with an IP-VPN line from a general communication company instead of a 5G network. In the present study, we examined the effect of adding IPsec encryption to the IP-VPN line on communication. We estimated that a communication bandwidth of 40 Mbps was sufficient for our robot, expecting it to increase at most by approximately 1 Mbps after the addition of IPsec. However, when IPsec encrypted communication was performed, the bandwidth increased more than expected and delayed the communication. The maximum frame length that could be transferred in the encrypted configuration was 1280 bytes, which is the default value for VPN routers. Larger packets were divided and retransmitted; therefore, the number of packets in the IPsec configuration was approximately double that in the configuration without IPsec. This is because the maximum communication frame length generated by the encoder/decoder exceeded that which can be transferred by the VPN router. Therefore, this issue may be solved by tuning the maximum transmission unit/maximum segment size of both devices when performing IPsec encryption and designing the devices to avoid packet division due to encryption. No previous studies have reported on the effect of adding IPsec to the IP-VPN line on communication, and no established standard yet exists for communication security in telesurgery. Based on the present findings, implementing double security on IP-VPN with IPsec encryption did not have a significant impact on communication; we believe that the resulting communication delay is acceptable.
A major limitation of the present study is that it comprised an animal study with a small sample size. Additionally, the robot we used has not yet received regulatory approval. Nevertheless, the present study showed that telesurgical support is feasible by installing a cockpit at each of two locations, 140 km apart; this double-surgeon cockpit system is a good first step toward realizing telesurgery. Furthermore, we demonstrated that dual-security communication is possible for telesurgery. Clinical trials are necessary before telesurgical support can be introduced into actual clinical practice in future.
References
Bogen EM, Schlachta CM, Ponsky T (2019) White paper: technology for surgical telementoring-SAGES project 6 technology working group. Surg Endosc 33:684–690. https://doi.org/10.1007/s00464-00018-06631-00468
Rodríguez García JI, Contreras Sáiz E, García Munar M, García Flórez L, Granero Trancón J (2021) Telemedicine, telementoring and telematic evaluation in surgery. Is it your time after COVID-19? Cir Esp (Engl Ed) 99:474–475. https://doi.org/10.1016/j.cireng.2021.1005.1005
Raborn LN, Janis JE (2021) Overcoming the Impact of COVID-19 on surgical mentorship: a scoping review of long-distance mentorship in surgery. J Surg Educ 78:1948–1964. https://doi.org/10.1016/j.jsurg.2021.1905.1001
Greenberg JA, Schwarz E, Paige J, Dort J, Bachman S (2021) At-home hands-on surgical training during COVID19: proof of concept using a virtual telementoring platform. Surg Endosc 35:1963–1969. https://doi.org/10.1007/s00464-00021-08470-00466
Kirkpatrick AW, McKee JL, Tomlinson C, Donley N, Ball CG, Wachs J (2022) A randomized controlled pilot trial of video-modelling versus telementoring for improved hemorrhage control wound packing. Am J Surg 5:00097–96
Din N, Chan CC, Cohen E, Iovieno A, Dahan A, Rootman DS, Litvin G (2022) Remote surgeon virtual presence: a novel telementoring method for live surgical training. Cornea 41:385–389. https://doi.org/10.1097/ICO.0000000000002921
Prince SW, Kang C, Simonelli J, Lee YH, Gerber MJ, Lim C, Chu K, Dutson EP, Tsao TC (2020) A robotic system for telementoring and training in laparoscopic surgery. Int J Med Robot 16:e2040. https://doi.org/10.1002/rcs.2040
Erridge S, Yeung DKT, Patel HRH, Purkayastha S (2019) Telementoring of surgeons: a systematic review. Surg Innov 26:95–111. https://doi.org/10.1177/1553350618813250
Morohashi H, Hakamada K, Kanno T, Kawashima K, Akasaka H, Ebihara Y, Oki E, Hirano S, Mori M (2022) Social implementation of a remote surgery system in Japan: a field experiment using a newly developed surgical robot via a commercial network. Surg Today 52:705–714. https://doi.org/10.1007/s00595-00021-02384-00595
Ebihara Y, Oki E, Hirano S, Takano H, Ota M, Morohashi H, Hakamada K, Urushidani S, Mori M (2022) Tele-assessment of bandwidth limitation for remote robotics surgery. Surg Today 12:1–7
Akasaka H, Hakamada K, Morohashi H, Kanno T, Kawashima K, Ebihara Y, Oki E, Hirano S, Mori M (2022) Impact of the suboptimal communication network environment on telerobotic surgery performance and surgeon fatigue. PLoS One 17:e0270039. https://doi.org/10.1371/journal.pone.0270039
D’Onofrio G, Fiorini L, Sorrentino A, Russo S, Ciccone F, Giuliani F, Sancarlo D, Cavallo F (2022) Emotion recognizing by a robotic solution initiative (EMOTIVE project). Sensors (Basel) 22:2861. https://doi.org/10.3390/s22082861
Aghazadeh MA, Jayaratna IS, Hung AJ, Pan MM, Desai MM, Gill IS, Goh AC (2015) External validation of global evaluative assessment of robotic skills (GEARS). Surg Endosc 29:3261–3266. https://doi.org/10.1007/s00464-00015-04070-00468
Marescaux J, Leroy J, Gagner M, Rubino F, Mutter D, Vix M, Butner SE, Smith MK (2001) Transatlantic robot-assisted telesurgery. Nature 413:379–380. https://doi.org/10.1038/35096636
Anvari M (2007) Remote telepresence surgery: the Canadian experience. Surg Endosc 21:537–541. https://doi.org/10.1007/s00464-00006-09040-00468
Anvari M, McKinley C, Stein H (2005) Establishment of the world’s first telerobotic remote surgical service: for provision of advanced laparoscopic surgery in a rural community. Ann Surg 241:460–464. https://doi.org/10.1097/1001.sla.0000154456.0000169815.ee
Sebajang H, Trudeau P, Dougall A, Hegge S, McKinley C, Anvari M (2006) The role of telementoring and telerobotic assistance in the provision of laparoscopic colorectal surgery in rural areas. Surg Endosc 20:1389–1393. https://doi.org/10.1007/s00464-00005-00260-00460
Acknowledgements
The authors thank Ms. Junko Eguchi for her assistance with the experiment and manuscript preparation. This work was funded by AMED under grant number JP21hs0122001s0602. We would like to thank Editage (www.editage.com) for English language editing.
Funding
This research was supported by AMED under Grant No: JP21hs0122001h0002.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Drs. Eiji Oki, Mitsuhiko Ota, Tomonori Nakanoko, Yasushi Tanaka, Satoshi Toyota, Qingjiang Hu, Yu Nakaji, Ryota Nakanishi, Koji Ando, Yasue Kimura, Yuichi Hisamatsu, Koshi Mimori, Yoshiya Takahashi, Hajime Morohashi, Kotaro Tadano, Hironobu Takano, Yuma Ebihara, Masaki Shiota, Junichi Inokuchi, Masatoshi Eto, Tomoharu Yoshizumi, Satoshi Hirano, and Masaki Mori have no conflicts of interest or financial ties to disclose. Takahiro Kanno and Kenji Kawashima received stock options from Riverfield, Inc. Kenichi Hakamada has received research funding from AMED and honoraria for lectures and manuscripts from the following organizations: Japan Medical Association, Keidanren, NTT East Corporation, Nankodo, Tokyo Igakusha, and Medical Sciences International.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.


464_2023_10061_MOESM2_ESM.jpg
Supplementary file2 (JPG 36 KB) The hemostasis time is plotted for experts and beginners. Horizontal lines indicate mean values
Supplementary file3 (MP4 82141 KB) From a remote location, the surgeon can switch the operating initiative to perform hemostasis
Supplementary file4 (MP4 121044 KB) Telesurgical support can be provided from an area 140 km away, with the possibility of switching surgeons at any time
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

{kind=link}
{kind=link}
Cite this article
Oki, E., Ota, M., Nakanoko, T. et al. Telesurgery and telesurgical support using a double-surgeon cockpit system allowing manipulation from two locations. Surg Endosc 37, 6071–6078 (2023). https://doi.org/10.1007/s00464-023-10061-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-023-10061-6