
Abstract
Background
Concerns regarding the aerosolized transmission of SARS-CoV-2 via SS have caused significant apprehension among surgeons related to the use of minimally invasive surgery (MIS) during the COVID19 pandemic. While a limited number of studies have previously demonstrated the presence of viral material in SS, no comprehensive systematic review exists on the subject of viral transmission in SS.
Methods
A systematic review of the literature was conducted as per PRISMA guidelines. MEDLINE, EMBASE, and CENTRAL databases were searched for publications reporting the primary outcome of the presence of viral particles in SS and secondary outcomes of indices suggesting transmission of viable virus particles in SS producing clinically important infection. All human, animal, and in vitro studies which used accepted analytic techniques for viral detection were included. A meta-analysis was not complete due to methodologic heterogeneity and inconsistent reporting of outcomes of interest.
Results
23 publications addressed the presence of viral components in SS, and 19 (83%) found the presence of viral particles in SS. 21 publications additionally studied the ability of SS to induce clinically relevant infection in host cells, with 9 (43%) demonstrating potential for viral transmission.
Conclusion
Evidence exists for viral transmission via SS. However, HPV remains the only virus with documented transmission to humans via SS. While meaningful translation into practical guidelines during the COVID pandemic remains challenging, no evidence exists to suggest increased risk in MIS.
Similar content being viewed by others


SARS-CoV-2 is a novel coronavirus with zoonotic origins causing the illness COVID19, which has rapidly progressed from an isolated epidemic in the city of Wuhan and Hubei province of the People’s Republic of China to a worldwide pandemic affecting more than 15.7 million in 213 countries and territories, as of the day of submission of this article [1, 2].
Coronaviruses are enveloped large single-stranded RNA viruses that can infect animals and humans [1]. The COVID19 virus is of the beta-subfamily of coronaviruses with 96% whole-genome analysis matching that found in bats and is similar to SARS-CoV [3]. Although COVID19 was initially detected by identifying a cluster of unusual cases of pneumonia and thereafter thought to cause predominantly respiratory influenza like symptoms, it is now recognized that COVID19 may affect multiple organ systems and cause a range of presentations including (i) asymptomatic or presymptomatic carriers; (ii) respiratory or influenza like symptoms: fever, persistent cough, nasal congestion, dyspnea, hypoxemia, pneumonia; (iii) gastrointestinal symptoms: nausea, diarrhea, non-specific abdominal pain; (iv) head and neck symptoms: anosmia, ageusia; (v) cardiovascular: direct cardiac effects, abnormal blood clotting; (vi) other: fatigue/malaise, myalgia, headache, neuropathy and worsening of underlying chronic medical, and psychiatric conditions [4,5,6,7,8]. Preliminary reports in Chinese patients indicate that the majority, 81% of those affected will have a mild form of the disease, while 14% will develop severe symptoms and 5% require critical care admission [6]. COVID19 has affected all age groups with the youngest reported case in a 1 month old; however, the majority of affected persons are between 30–69 years old with a reported slight male predominance [6]. Mortality rates have been reported to be greatest in the extremes of age and in those with a greater burden of comorbidities [9]. The case fatality rate varies between affected countries, however, in general is thought to approximate 2–4% [10]. The basic reproductive number (Ro) of COVID19 or infection rate without social distancing or other intervention has been estimated at between 1.4 and 3.9 [11]. COVID19 has been isolated in respiratory secretions, stool, blood, and peritoneal fluid [12]. Further, the virus has been shown to spread through droplet and contact transmission through mucous membranes, fecal–oral transmission, and through aerosol transmission during aerosol-generating medical procedures (AGMP). Airborne transmission outside of AGMP’s and blood borne transmission have not been demonstrated [13].
In response to the identification of a significant number of medical professionals being affected by COVID19 and initial lack of certainty related to modes of transmission, major surgical societies released guidelines urging caution with respect to AGMPs, including surgery, and, in particular, minimally invasive (MIS) surgery [14]. These recommendations appeared to initially have created wide spread confusion and apprehension toward MIS within the surgical community during the pandemic.
It has long been recognized that surgical smoke (SS), otherwise known as surgical plume or aerosols (defined as any gaseous byproduct from the use of electrosurgical, ultrasonic, and surgical lasers which contain both cellular and acellular material) pose an occupational health risk [15]. The small particles created with these devices vary with the particular device modality, device settings, tissue characteristics, and length of device activation [16]. SS contains particles which can lead to respiratory and cardiovascular inflammation, carcinogens, viable malignant cells, and viable pathogens such as bacteria and viruses [15,16,17]. The latter has been demonstrated with human papilloma virus (HPV), hepatitis B (HepB), and human immunodeficiency virus (HIV), although outside of HPV, no documented cases of transmission in SS have been observed. Further, it has been postulated that during laparoscopy, due to the contained nature of the pneumoperitoneum, that these small particles build to high concentrations and, with unfiltered release through the trocar, may lead to a high velocity jet which increases particle dispersion and potentially particle concentration within an operating room. Hence, the latter two findings, of the theoretical potential for viral transmission and increased SS generation and dispersion with unfiltered evacuation of pneumoperitoneum, have generated extraordinary apprehension among some surgeons following the release of practical guidance from the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) in the setting of COVID19 [14]. However, to our knowledge, very limited data on the subject exist; therefore, we performed a systematic review of the literature to better outline what is known regarding the risk of viral transmission in SS.
Methods and materials
Objective
The primary objective of this study was to determine the risk of viral transmission from a carrier patient to operating room personnel via SS during open and laparoscopic surgery. In particular, the primary outcome of interest was whether viral particles including viral DNA, RNA, proteins, or viable virus-infected cells can be detected in the SS generated during a broad spectrum of surgical procedures.
Study selection
A systematic review of the literature was conducted and reported in accordance with the Preferred Reporting of Items for Systematic Reviews and Meta-Analyses (PRISMA) protocols [18]. A comprehensive search of the MEDLINE, EMBASE, and CENTRAL databases was conducted with a medical librarian. The search was conducted from database inception—1946 (MEDLINE), 1974 (EMBASE), and 1991 (CENTRAL) to April 2nd 2020 and limited to English language studies. The search was performed using three domains of different permutations of medical subject heading (MeSH) or EmTree headings linked with the Boolean operator “OR,” and subsequently combined with “AND.” The first domain includes all surgical subspecialties, as well as surgical and dermatologic procedures; the second SS and instruments generating SS; and the third virus and viral particles. See Supplemental Fig. 1 for full search strategies. Duplicated studies were removed. All abstracts and studies included for full-text review were screened by two independent reviewers (TW, CR-M). Additional studies were identified through a reference review. This systematic review was submitted to PROSPERO prior to data abstraction.

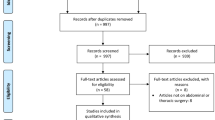
PRISMA diagram of study selection in the systematic literature search (Color figure online)
Inclusion criteria
All human, animal, and in vitro primary research articles were included if they documented the presence or effects of viral particles in SS generated by energy-based surgical instruments across all surgical specialties. Studies were excluded if they were preclinical experimental work or did not include a laboratory-based method for detection of viral constituents or effects from exposure to SS.
Abstraction and analysis
Data abstraction and quality assessment of included studies were performed by two independent reviewers (TW and CR-M). Quality of evidence was assessed based on the 2011 Oxford Centre for Evidence-Based Medicine Levels of Evidence [19]. Methodological quality and bias were assessed using the National Institutes of Health Quality Assessment Tool for case series and case reports [20]. Data abstraction was carried out using a standardized form encompassing study design, surgical instrument, procedure, virus, detection method, plume location, and specialty represented. Our primary outcome of interest was the presence of viral components in SS. Secondary outcomes were indices suggesting transmission of viable virus particles in SS producing clinically important infection. Given the wide heterogeneity among studies, a meta-analysis was not performed.
Results
The search strategy, after removing duplicates, identified 738 abstracts for screening, of which 55 articles were retained for full manuscript review and an additional 3 articles were identified through a manual search of the article references. As seen in the PRISMA flow diagram (Fig. 1), 35 articles and abstracts met the aforementioned inclusion criteria and underwent data abstraction [21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55].
As demonstrated in Table 1, all studies included were either case series or quasi-experimental studies of a low level of evidence, based on the 2011 Oxford CEBM levels of evidence document and were identified to have methodological weaknesses, when assessed using the National Institutes of Health quality assessment tool for case series. Significant methodological heterogeneity was observed.
All studies
Overall, 23 publications addressed the primary outcome of interest, the presence of viral DNA, RNA, or viral-infected cells contained within SS [21,22,23,24,25, 27, 31,32,33, 35,36,37, 39, 40, 42, 45,46,47, 49, 50, 52,53,54]. On the other hand, 21 publications, either additionally or solely, sought to identify if those viral particles in SS could produce clinically important infection of operating room personnel [26,27,28,29,30,31, 33, 34, 38, 41, 43, 44, 46, 48,49,50,51,52,53,54]. Findings from individual studies are summarized in Tables 2 and 3, respectively.
Twelve different viruses or bacteriophage models for viruses were investigated (as outlined in Tables 2 and 3), the vast majority addressed HPV. Publications came from 8 different surgical specialties. Gynecology, dermatology, otolaryngology, and ophthalmology represented the majority with 22.9, 22.9, 17.1, and 11.4% of publications, respectively. General surgery, urology, and orthopedic surgery specialties were poorly represented. As can be seen in Tables 2 and 3, although SS generated by a total of 10 different instruments was investigated, the most commonly studied modalities were the CO2 laser and electrocautery.
Studies addressing viral particles in SS
Of the 23 publications which investigated for the primary outcome of viral particles (DNA, RNA, protein, virus-infected cells) within SS, 17 (74%) addressed the presence of HPV or models of HPV (BPV or mmuPV1), 3 (13%) HepB virus, 2 (9%) HIV, and 1 (4%) varicella zoster virus (VZV). A total of 19 (83%) studies found the presence of viral particles from the target virus in SS using well-accepted laboratory methodology. All exceptions were in publications investigating HPV. The cause of the discrepant results is unknown. Significant heterogeneity within study methodology was observed with 18 (78%) using in vivo, 5 (21%) using in vitro, 2 (9%) using ex vivo techniques; 4 publications reported findings in animal models; 10 different surgical devices were used to generate SS; 9 different types of surgical procedures where SS is created were investigated; and finally the location, method of collection, and processing of SS samples were seen to vary.
Studies addressing infectivity of viable viral particles in SS
A total of 21 publications were identified that sought to determine if viable viral particles in SS could produce clinically important infection of operating room personnel. Three general methods were used: (1) the culture of live virus from the SS samples, (2) the culture of live virus from samples taken in clinically important locations on operating room personnel, or (3) the ability of the SS to induce clinically relevant infection in cell cultures or an animal model. Each method was used in 12 (57%), 7 (33%), and 4 (19%) of the publications, respectively. Viral pathogens investigated were 12 (57%) HPV or models of HPV (BPV or mmuPV1), 1 (5%) model of HIV (simian immunodeficiency virus, SIV) and 1 (5%) VZV, 3 (14%) other viral models, and 3 (14%) bacteriophage models of small viruses. Potential for transmission of viral infection through viable viral particles in SS was confirmed in 9 (43%), unable to be demonstrated in 9 (43%) and was equivocal in 1 (4%) publication. Once again, there was significant heterogeneity in the utilized methodology; 12 (57%) used in vivo and 9 (43%) used in vitro techniques; 3 publications reported findings in animal models while 10 used infected cell cultures, 7 different surgical devices were used to generate SS, and sampling protocols varied considerably.
Discussion
Major findings
In this systematic review, our objective was to identify and summarize the extent of what is known regarding the risk of viral transmission in SS. Although this has been addressed in previous narrative and systematic reviews as a minor topic within the broader subject of occupational health implications of SS, to our knowledge, this paper represents the most comprehensive systematic review focused entirely on the risk of viral transmission in SS.
A total of 35 publications with relevant findings were ultimately identified [21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54]. The publications were grouped by the outcome of interest with two predominant themes observed in the study outcomes. The first category, including 23 publications, investigated whether viral DNA, RNA, proteins, or viral-infected cells were contained within the SS [21,22,23,24,25, 27, 31,32,33, 35,36,37, 39, 40, 42, 45,46,47, 49, 50, 52,53,54]. The premise being that if viral particles are contained within SS, then there exists at least a theoretical risk that SS can lead to viral transmission. However, the ability of a viral particle to establish a clinically relevant infection in a host is dependent on a number of factors outside of their mere presence. Hence, the assertion that these studies show a theoretical risk, not definitive proof of concept. In this vein, a second group of 21 publications were found that addressed this knowledge gap by either additionally or solely, investigating if those viral particles in SS could produce clinically important infection of operating room personnel [26,27,28,29,30,31, 33, 34, 38, 41, 43, 44, 46], [48,49,50,51,52,53,54]. This was accomplished in three different manners: first, by the ability to culture live virus from samples of SS or samples taken in clinically important locations on the operating room personnel. Establishing that the viral particles in SS are indeed viable and can be found in locations that are susceptible to viral infection of a host, in this case, operating room personnel. Second, by the ability of the SS to induce pathologic changes in cell cultures; and third, by the ability of the SS to produce clinically relevant infection in an animal model. Both of which confirm that the viable viral particles in SS retain the ability to interact with host cells and generate the known clinical sequela from their infection.
These combined publications have shown there to be definitive evidence that transmission of viable viral particles in SS is possible and can produce clinically important infections in exposed operating room personnel or models thereof. However, as can be seen in our systematic review, although a number of viral pathogens have been found to have theoretical risk for transmission in SS, the definitive evidence for establishing clinically important infection has been shown only for a limited number. In more detail, viral particles of HPV (or HPV models), HepB, HIV, and VZV have all been isolated from SS; however, only HPV, adenovirus, herpes simplex virus (HSV), SPVV, and bacteriophage φX174 (model for submicron viruses) have been shown to produce clinically relevant pathologic changes in cell cultures or induce infection in an animal model exposed to the respective SS [22,23,24, 26, 27, 29, 31,32,33, 35, 36, 38,39,40, 42,43,44,45,46,47, 50,51,52, 54]. Further, to date, HPV is the only virus to our knowledge which has been shown to produce clinical infection in humans exposed to SS [56, 68,69,70].
Of the publications looking for the presence of viral particles in SS, it should be stated that 74% investigated for HPV or models of HPV in SS and that the presence of HPV viral particles within the SS was not uniform, with 30% of these studies returning a negative result. Although the cause of the discrepant results is unknown, differences in the modality used (CO2 or YAG laser), distance of collection of SS from the lesion (> 5 cm, adjacent hand piece), laboratory techniques used (southern blot, PCR), or lesion used to produce the SS (oropharyngeal SCC, laryngeal papilloma) was seen to differ 21,37,49,53]. The works of Higashi et al. and Hirota et al. on HepB were similar in methodology, and both were ex vivo experiments ablating virus-infected cell cultures and human liver samples with electrocautery. The SS collection occurred within 1-2 cm of the ablated tissue; hence, unsurprisingly, similar positive results were seen in both works [35, 36]. Kwak et al. represent the only in vivo study on a virus other than HPV; in particular, these investigators demonstrated the presence of HepB viral particles in SS evacuated from trocars during relatively long (> 1 hr) robotic or laparoscopic gastric, colon, or liver surgery wherein electrocautery was used in patients with known HepB chronic infection [42]. Baggish et al. confirmed the presence of HIV particles in SS after ablating an infected cell culture with a CO2 laser, once again the SS was taken within 1 cm of the ablated cell [24]. Johnson et al. subjected a number of different tissues with HIV-infected blood cells to different SS generating orthopedic instruments and collected the smoke at varying distance from the affected tissue. HIV particles were detected in the SS from the router blade and bone saw but not detect when electrocautery was the used modality [39]. Lastly, Taravella et al. ablated VZV-infected cells with an excimer laser and detected VZV particles in the ensuant SS at an unknown distance from the ablate cells [50].
Similarly, of the publications addressing the infectivity of viable viral particles in SS, 12 (57%) investigated HPV or models of HPV, and 41% of these did not demonstrate changes in cell cultures or animal models suggestive of infection. Differences in outcome could not be explained by the modality of surgical instrument used, however, may relate to the procedure performed, the lesion the procedure was performed on or the distance of collection of the sample of SS [30, 31, 41, 49, 53]. For example, Zhou et al. demonstrated that HPV concentration in SS had an inverse relationship with the distance of sample collection from the source [54]. The majority of studies on HPV did confirm that clinical infection is possible when the host is exposed to SS containing HPV particles. This confirms previously published case reports and case series of operating room personnel contracting laryngeal HPV during ablative procedures of genital and laryngeal condyloma and will not be further addressed [56, 68,69,70]. Adenovirus, HSV or a model thereof, and a bacteriophage model of small viruses were also seen to induce cytopathologic changes suggestive of infection in cell cultures exposed to the respective SS [29, 43, 44, 51, 55]. It should be stated, however that no evidence of infection of animal or human hosts exposed to SS currently exists. Once again, it is not clear why discrepant results were obtained in similar studies on VZV, pseudorabies virus (model of HIV or HSV), and SIV (model of HIV). Whether this indicates a difference in the behavior of these viruses or differences in study design is uncertain [28, 34, 48, 50].
Taken together, these studies indicate that multiple factors, other than the type of virus, are important in determining whether viral particles are found in SS and whether these viral particles retain the ability to produce clinically relevant infections in those exposed to SS. SS is composed predominantly of water in the form of steam, while only 5% is made of particulate matter from cellular debris [17]. Components of SS include compounds which cause inflammation in respiratory and vascular tissue, carcinogens, malignant cells, and pathogens [17]. Many of these components have been well documented elsewhere and are beyond the scope of this review [17, 57, 60]. Germaine to our current work is the observation that the composition and particle size of SS have been shown to vary depending on the modality, device settings, length of device activation, length of surgical procedure, and the type of tissue on which is being operated [17, 57,58,59]. Electrocautery produced from contemporary electrosurgery devices and surgical lasers heat the target tissue to the boiling point with resultant cell rupture generating SS. Electrosurgical device settings affect the rapidity of tissue heating, and hence, the characteristics of particulate matter in the resultant SS and may also affect viability of pathogens. On the other hand, SS generated from ultrasonic surgical devices is produced by vibration of cells causing relatively low-temperature vaporization. Particulate matter from each of these modalities has been noted to differ from one another. The mean particle size is smallest with electrosurgery devices < 0.1 microns, whereas with surgical lasers, it is 0.31 microns, and with ultrasonic surgery devices, it is 0.35–6.5 microns. Particles < 5 microns are known to be able to be inhaled and deposited at all levels of the airway and alveoli, and those < 0.1 microns may access the circulatory system [17, 60, 61]. Smaller particles tend to travel a further distance from the source device, with the furthest distance measured up to 100cm [60]. Additionally, small particulate matter has been postulated to cause a greater risk for chemical effects related to SS while larger particles may be more at risk for pathogen transmission. Interestingly, SS from ultrasonic devices has been shown to contain more concentrated particulate matter than that of electrosurgical devices [60]. Hence, the characteristics of SS due to difference in these factors between studies may have impacted the results observed in our systematic review with respect to viral transmission in SS. Given that the majority of these factors were not controlled for, the magnitude and direction of the effect on our results are not ascertainable.
Regarding previous assertions by several authors of the potential for increased risk of viral transmission associated with SS generated during MIS procedures, it is important to recognize that these are entirely theoretical [57, 62]. Although it has been shown that the SS contained in samples taken from the pneumoperitoneum during MIS procedures contains high concentrations of small particulate matter with chemicals which may cause inflammation, mutagenic agents, and carbon monoxide, no direct comparison between SS from MIS procedures and open surgery exist [57]. To our knowledge, there are only two studies which compare the background concentration of SS in the atmosphere of an operating room during the two forms of surgery [59, 63]. Despite being recently used to suggest otherwise, the publication of Li et al. showed a small non-statistically significant increase in atmospheric particulate matter concentration in the operating room at a single time point in a laparoscopic gynecologic procedure compared to an open procedure [63]. It should be highlighted that the study design was weak, did not control for many of the previously stated factors important in determining the characteristics of SS, did not report on trocar type used and hence propensity for air leakage to occur, and did not use a smoke evacuation system of any type in the laparoscopic procedure [63]. The study of Wang et al. was of better design; however, once again, air samples were taken after unfiltered release of pneumoperitoneum [59]. Importantly, our systematic review identified only a single publication wherein the SS of MIS procedures was found to contain viral particles (HepB DNA), and no publications investigated viral infectivity with MIS procedures [42]. Therefore, any comments espoused about an increased risk of viral transmission with MIS procedures should be viewed as speculation until rigorous scientific investigation suggests otherwise. Further, to date, no case reports of documented viral transmission to operating room personnel exist with MIS procedures. And last, both passive and active smoke evacuation systems have been investigated for MIS and when combined with a high efficacy particulate air (HEPA) or ultralow particulate air (ULPA) filters not only improve visibility but remove or reduce the concentration of chemical compounds from SS and capture 99.97% and 99.99% of airborne particles > 0.3 and 0.05 microns, respectively. The smallest relevant viral particle which could lead to viral transmission in SS has been shown to be approximately 0.12 microns [64].
Limitations
This is the first comprehensive review of the risk for viral transmission in SS; however, there are several limitations to this study. The methodological heterogeneity, methodological weaknesses, study design, and small sample sizes limit the ability to translate the findings of our review into practical recommendations. Additionally, due to these limitations, a pooled analysis to ascertain an estimate of the relative risk of viral transmission in SS was not possible. Furthermore, advancements in laboratory techniques over the past decades, with increasing sensitivity in isolating and detecting viral particles, make interpretation of early studies challenging. An important limitation to the detection of viral components in SS is the use of techniques such as Southern blot and PCR which can also detect fragments of DNA/RNA. Except for Garden et al. (2002), these studies did not differentiate between detecting intact nucleic acids from complete virions capable of infecting another host. Similarly, as viable cells have been described in SS [65,66,67], virus containing aerosolized cells cannot be excluded as the primary potentiator of transmission. This is an important distinction that significantly impacts the level of protective measures in the operating room. Finally, while we kept our search broad to encapsulate multiple specialties and surgical procedures to ensure a comprehensive review, case reports and studies that did not include a laboratory-based detection method were excluded as the causative role for transmission is often difficult to establish and inclusion introduces unnecessary bias. Several case reports and survey studies on HPV transmission were, therefore, excluded [56, 68,69,70,71].
Conclusion and recommendations
In this systematic review on the risk of viral transmission through SS, we have shown there to be definitive evidence that transmission of viable viral particles in SS is possible and can produce clinically important infections. However, although a number of viral pathogens have been found to have theoretical risk for transmission in SS, definitive evidence that clinically important infection is established has been shown only for a limited number. Specifically, to date, HPV is the only virus which has been shown to produce clinical infection in humans exposed to SS. Hence, although we agree that there is a theoretical risk that SARS-CoV-2 may be spread in surgical smoke, we reject the notion that MIS procedures are at greater risk than traditional open procedures. In fact, MIS allows for the filtration of aerosolized material in a contained field as opposed to open surgery, concurrently minimizing spillage of fluids and cells [67]. Additionally, MIS, especially robotic surgery, allows for less personnel in the immediate operating field, decreasing the potential for transmission via more traditional occupational health injury mechanisms [69]. Further, any small risk of viral transmission in SS with MIS procedures may be mitigated by following the practical recommendations disseminated by SAGES and partner organizations including (i) the use of smoke evacuation systems with a HEPA or ULPA filter with complete desufflation prior to specimen extraction or conversion to open; (ii) being conscious of avoiding air leaks through appropriate selection of entry techniques, trocars, and using the lowest necessary insufflation pressures; (iii) taking measures to minimize the generation of SS by using the lowest settings on energy devices, avoiding long sequences of tissue desiccation, using non-energy-based instruments for dissection where appropriate; and (iv) through the proper use of recommended personal protective equipment including diligence in donning/doffing techniques [64].
References
Weston S, Frieman MB (2020) COVID-19: Knowns, Unknowns, and Questions. mSphere. https://doi.org/10.1128/mSphere.00203-20
Johns Hopkins University Center for Systems Science and Engineering. COVID-19 Dashboard [Internet]. Baltimore: JHU CSSE; 2019 [cited May 11, 2020] Available from: https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6.
Zhou P, Yang XL, Wang XG, Hu B, Zhang L, Zhang W, Si HR, Zhu Y, Li B, Huang CL, Chen HD, Chen J, Luo Y, Guo H, Jiang RD, Liu MQ, Chen Y, Shen XR, Wang X, Zheng XS, Zhao K, Chen QJ, Deng F, Liu LL, Yan B, Zhan FX, Wang YY, Xiao GF, Shi ZL (2020) A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 579(7798):270–273
Hoehl S, Rabenau H, Berger A, Kortenbusch M, Cinatl J, Bojkova D, Behrens P, Böddinghaus B, Götsch U, Naujoks F, Neumann P, Schork J, Tiarks-Jungk P, Walczok A, Eickmann M, Vehreschild MJGT, Kann G, Wolf T, Gottschalk R, Ciesek S (2020) Evidence of SARS-CoV-2 Infection in Returning Travelers from Wuhan. China N Engl J Med 382(13):1278–1280
D’Amico F, Baumgart DC, Danese S, Peyrin-Biroulet L (2020) Diarrhea during COVID-19 infection: pathogenesis, epidemiology, prevention and management. Clin Gastroenterol Hepatol. https://doi.org/10.1016/j.cgh.2020.04.001
Novel Coronavirus Pneumonia Emergency Response Epidemiology Team (2020) The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi. 41(2):145–151
Hopkins C, Surda P, Kumar N (2020) Presentation of new onset anosmia during the COVID-19 pandemic. Rhinology. https://doi.org/10.4193/Rhin20.116
Tavazzi G, Pellegrini C, Maurelli M, Belliato M, Sciutti F, Bottazzi A, Sepe PA, Resasco T, Camporotondo R, Bruno R, Baldanti F, Paolucci S, Pelenghi S, Iotti GA, Mojoli F, Arbustini E (2020) Myocardial localization of coronavirus in COVID-19 cardiogenic shock. Eur J Heart Fail. https://doi.org/10.1002/ejhf.1828
Onder G, Rezza G, Brusaferro S (2020) Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA. https://doi.org/10.1001/jama.2020.4683
Khafaie MA, Rahim F (2020) Cross-Country Comparison of Case Fatality Rates of COVID-19/SARS-COV-2. Osong Public Health Res Perspect 11(2):74–80
Liu Y, Gayle AA, Wilder-Smith A, Rocklöv J (2020) The reproductive number of COVID-19 is higher compared to SARS coronavirus. J Travel Med. https://doi.org/10.1093/jtm/taaa021
Wang W, Xu Y, Gao R, Lu R, Han K, Wu G, Tan W (2020) Detection of SARS-CoV-2 in Different Types of Clinical Specimens. JAMA 11:e203786
Public Health Ontario. COVID-19 – What We Know So Far About… Routes of Transmission [Internet]. Toronto: PHO; 2020 [cited 2020 April 20]. Available at: https://www.publichealthontario.ca/-/media/documents/ncov/wwksf-routes-transmission-mar-06-2020.pdf?la=en.
Society of American Gastrointestinal and Endoscopic Surgeons (SAGES). SAGES and EAES recommendations regarding surgical response to covid-19 crisis [Internet]. Los Angeles: SAGES; 2020 [cited 2020 April 24]. Available at: https://www.sages.org/recommendations-surgical-response-covid-19/.
Alp E, Bijl D, Bleichrodt RP, Hansson B, Voss A (2006) Surgical smoke and infection control. J Hosp Infect 62(1):1–5
Karjalainen M, Kontunen A, Saari S, Rönkkö T, Lekkala J, Roine A, Oksala N (2018) The characterization of surgical smoke from various tissues and its implications for occupational safety. PLoS ONE 13(4):e0195274
Limchantra IV, Fong Y, Melstrom KA (2019) Surgical Smoke Exposure in Operating Room Personnel: A Review. JAMA Surg. https://doi.org/10.1001/jamasurg.2019.2515
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA, PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) (2015) statement. Syst Rev. https://doi.org/10.1186/2046-4053-4-1
OCEBM Levels of Evidence Working Group. The Oxford 2011 Levels of Evidence. 2011 [Internet]. Oxford: OCEBM Group; 2011 [cited 2020 April 10]. Available at: https://www.cebm.net/wp-content/uploads/2014/06/CEBM-Levels-of-Evidence-2.1.pdf.
National Heart, Lung, and Blood Institute. NHLBI Study Quality Assessment Tools [Internet]. Bethesda: NHLBI; 2014 [cited 2020 April 10]. Available at: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools.
Abramson AL, DiLorenzo TP, Steinberg BM (1990) Is papillomavirus detectable in the plume of laser-treated laryngeal papilloma? Archives of Otolaryngology-Head & Neck Surgery 116(5):604–607
Akbarov I, Tok A, Wieland U, Engelmann U, Wille S. HPV-contamination of laser smoke during laser treatment of condylomata acuminata. European Urology, Supplements.Conference: 28th Annual Congress of the European Association of Urology, EAU.Milan Italy. Conference Publication: (var.pagings) 2013;12(1):e624.
Andre P, Orth G, Evenou P, Guillaume JC, Avril MF (1990) Risk of papillomavirus infection in carbon dioxide laser treatment of genital lesions. J Am Acad Dermatol 22(1):131–132
Baggish MS, Poiesz BJ, Joret D, Williamson P, Refai A (1991) Presence of human immunodeficiency virus DNA in laser smoke. Lasers Surg Med 11(3):197–203
Bellina JH, Stjernholm RL, Kurpel JE (1982) Analysis of plume emissions after papovavirus irradiation with the carbon dioxide laser. J Reprod Med 27(5):268–270
Bergbrant IM, Samuelsson L, Olofsson S, Jonassen F, Ricksten A (1994) Polymerase chain reaction for monitoring human papillomavirus contamination of medical personnel during treatment of genital warts with CO2 laser and electrocoagulation. Acta Derm Venereol 74(5):393–395
Best SR, Esquivel D, MellingerPilgrim R, Roden RBS, Pitman MJ (2020) Infectivity of murine papillomavirus in the surgical byproducts of treated tail warts. Laryngoscope 130(3):712–717
Capizzi PJ, Clay RP, Battey MJ (1998) Microbiologic activity in laser resurfacing plume and debris. Lasers Surg Med 23(3):172–174
Ediger MN, Matchette LS (1989) In vitro production of viable bacteriophage in a laser plume. Lasers Surg Med 9(3):296–299
Ferenczy A, Bergeron C, Richart RM (1990) Carbon dioxide laser energy disperses human papillomavirus deoxyribonucleic acid onto treatment fields. Am J Obstet Gynecol 163(4 Pt 1):1271–1274
Ferenczy A, Bergeron C, Richart RM (1990) Human papillomavirus DNA in CO2 laser-generated plume of smoke and its consequences to the surgeon. Obstet Gynecol 75(1):114–118
Garden JM, O’Banion MK, Shelnitz LS, Pinski KS, Bakus AD, Reichmann ME, Sundberg JP (1988) Papillomavirus in the vapor of carbon dioxide laser-treated verrucae. JAMA 259(8):1199–1202
Garden JM, O’Banion MK, Bakus AD, Olson C (2002) Viral disease transmitted by laser-generated plume (aerosol). Arch Dermatol 138(10):1303–1307
Hagen KB, Kettering JD, Aprecio RM, Beltran F, Maloney RK (1997) Lack of virus transmission by the excimer laser plume. Am J Ophthalmol 124(2):206–211
Higashi S, Miyazaki Y, Makino T, Takahashi T, Kurokawa Y, Yamasaki M, Takiguchi S, Mori M, Doki Y, Nakajima K. Surgical smoke as potential biohazard: Is viral DNA contained?. Surgical Endoscopy and Other Interventional Techniques 2017 Scientific Session of the Society of American Gastrointestinal and Endoscopic Surgeons, SAGES;Conference:2017.
Hirota M, Higashi S, Takahashi H, Miyazaki ., Takahashi T, Kurokawa Y, Yamasaki M, Mori M, Doki K, Nakajima K. Potential biological hazard in the surgical plume: It contains DNA fragments of virus derived from the host. Surg Endosc 2018 International Congress of the European Association for Endoscopic Surgery, EAES;Conference:26th.
Hughes PSH, Hughes AP (1998) Absence of human papillomavirus DNA in the plume of erbium:YAG laser- treated warts. J Am Acad Dermatol 38(3):426–428
Ilmarinen T, Auvinen E, Hiltunen-Back E, Ranki A, Aaltonen L, Pitkaranta A (2012) Transmission of human papillomavirus DNA from patient to surgical masks, gloves and oral mucosa of medical personnel during treatment of laryngeal papillomas and genital warts. Eur Arch Otorhinolaryngol 269(11):2367–2371
Johnson GK, Robinson WS (1991) Human immunodeficiency virus-1 (HIV-1) in the vapors of surgical power instruments. J Med Virol 33(1):47–50
Kashima HK, Kessis T, Mounts P, Shah K (1991) Polymerase chain reaction identification of human papillomavirus DNA in CO2 laser plume from recurrent respiratory papillomatosis. Otolaryngol Head Neck Surg 104(2):191–195
Kunachak S, Sithisarn P, Kulapaditharom B (1996) Are laryngeal papilloma virus-infected cells viable in the plume derived from a continuous mode carbon dioxide laser, and are they infectious? A preliminary report on one laser mode. J Laryngol Otol 110(11):1031–1033
Kwak HD, Kim SH, Seo YS, Song KJ (2016) Detecting hepatitis B virus in surgical smoke emitted during laparoscopic surgery. Occup Environ Med 73(12):857–863
Matchette LS, Faaland RW, Royston DD, Ediger MN (1991) In vitro production of viable bacteriophage in carbon dioxide and argon laser plumes. Lasers Surg Med 11(4):380–384
Moreira LB, Sanchez D, Trousdale MD, Stevenson D, Yarber F, McDonnell PJ (1997) Aerosolization of infectious virus by excimer laser. Am J Ophthalmol 123(3):297–302
Neumann K, Cavalar M, Rody A, Friemert L, Beyer DA (2018) Is surgical plume developing during routine LEEPs contaminated with high-risk HPV? A pilot series of experiments. Arch Gynecol Obstet 297(2):421–424
Sawchuk WS, Weber PJ, Lowy DR, Dzubow LM (1989) Infectious papillomavirus in the vapor of warts treated with carbon dioxide laser or electrocoagulation: detection and protection. J Am Acad Dermatol 21(1):41–49
Sood AK, Bahrani-Mostafavi Z, Stoerker J, Stone IK (1994) Human papillomavirus DNA in LEEP plume. Infectious Diseases in Obstetrics & Gynecology 2(4):167–170
Starr JC, Kilmer SL, Wheeland RG (1992) Analysis of the carbon dioxide laser plume for simian immunodeficiency virus. Journal of Dermatologic Surgery & Oncology 18(4):297–300
Subbarayan RS, Shew M, Enders J, Bur AM, Thomas SM (2019) Occupational exposure of oropharyngeal human papillomavirus amongst otolaryngologists. Laryngoscope. https://doi.org/10.1002/lary.28383
Taravella MJ, Weinberg A, Blackburn P, May M (1997) Do intact viral particles survive excimer laser ablation? Arch Ophthalmol 115(8):1028–1030
Taravella MJ, Weinberg A, May M, Stepp P (1999) Live virus survives excimer laser ablation. Ophthalmology 106(8):1498–1499
Weyandt GH, Tollmann F, Kristen P, Weissbrich B (2011) Low risk of contamination with human papilloma virus during treatment of condylomata acuminata with multilayer argon plasma coagulation and CO 2 laser ablation. Arch Dermatol Res 303(2):141–144
Wisniewski PM, Warhol MJ, Rando RF, Sedlacek TV, Kemp JE, Fisher JC (1990) Studies on the transmission of viral disease via the CO2 laser plume and ejecta. Journal of Reproductive Medicine for the Obstetrician and Gynecologist 35(12):1117–1123
Zhou Q, Hu X, Zhou J, Zhao M, Zhu X, Zhu X (2019) Human papillomavirus DNA in surgical smoke during cervical loop electrosurgical excision procedures and its impact on the surgeon. Cancer Manag Res 29(11):3643–3654
Matchette LS, Vegella TJ, Faaland RW (1993) Viable bacteriophage in CO2 laser plume: Aerodynamic size distribution. Lasers Surg Med 13(1):18–22
Calero L, Brusis T (2003) Larynxpapillomatose - erstmalige Anerkennung als Berufskrankheit bei einer OP-Schwester [Laryngeal papillomatosis - first recognition in Germany as an occupational disease in an operating room nurse]. Laryngorhinootologie. 82(11):790–793
Barrett WL, Garber SM (2003) Surgical smoke: a review of the literature. Is this just a lot of hot air? Surg Endosc. https://doi.org/10.1007/s00464-002-8584-5
Tan W, Zhu H, Zhang N, Dong D, Wang S, Ren F, Xiang J, Wu R, Lv Y (2019) Characterization of the PM2.5 concentration in surgical smoke in different tissues during hemihepatectomy and protective measures. Environ Toxicol Pharmacol. https://doi.org/10.1016/j.etap.2019.103248
Wang HK, Mo F, Ma CG, Dai B, Shi GH, Zhu Y, Zhang HL, Ye DW (2015) Evaluation of fine particles in surgical smoke from an urologist’s operating room by time and by distance. Int Urol Nephrol 47(10):1671–1678
Okoshi K, Kobayashi K, Kinoshita K, Tomizawa Y, Hasegawa S, Sakai Y (2015) Health risks associated with exposure to surgical smoke for surgeons and operation room personnel. Surg Today 45(8):957–965
Weld KJ, Dryer S, Ames CD, Cho K, Hogan C, Lee M, Biswas P, Landman J (2007) Analysis of surgical smoke produced by various energy-based instruments and effect on laparoscopic visibility. J Endourol 21(3):347–351
Zheng MH, Boni L, Fingerhut A (2020) Minimally Invasive Surgery and the Novel Coronavirus Outbreak: Lessons Learned in China and Italy. Ann Surg. https://doi.org/10.1097/SLA.0000000000003924
Li CI, Pai JY, Chen CH (2020) Characterization of smoke generated during the use of surgical knife in laparotomy surgeries. J Air Waste Manag Assoc 70(3):324–332
Society of American Gastrointestinal and Endoscopic Surgeons (SAGES). Resources for smoke & gas evacuation during open, laparoscopic, and endoscopic procedures [Internet]. Los Angeles: SAGES; 2020 [cited 2020 April 24]. Available at: https://www.sages.org/resources-smoke-gas-evacuation-during-open-laparoscopic-endoscopic-procedures/.
In SM, Park DY, Sohn IK, Kim CH, Lim HL, Hong SA, Jung DY, Jeong SY, Han JH, Kim HJ (2015) Experimental study of the potential hazards of surgical smoke from powered instruments. Br J Surg 102(12):1581–1586
Ikramuddin S, Lucus J, Ellison EC, Schirmer WJ, Melvin WS (1998) Detection of aerosolized cells during carbon dioxide laparoscopy. J Gastrointest Surg. 2(6):580–583
Fletcher JN, Mew D, DesCôteaux JG (1999) Dissemination of melanoma cells within electrocautery plume. Am J Surg 178(1):57–59
Hallmo P, Naess O (1991) Laryngeal papillomatosis with human papillomavirus DNA contracted by a laser surgeon. Eur Arch Otorhinolaryngol 248(7):425–427
Rioux M, Garland A, Webster D, Reardon E (2013) HPV positive tonsillar cancer in two laser surgeons: case reports. J Otolaryngol Head Neck Surg 42(1):54
Lobraico RV, Schifano MJ, Brader KR (1989) Acquired HPV lesions compared in laser and nonlaser users. J Gynecol Surg 5(1):77–85
Gloster HM Jr, Roenigk RK (1995) Risk of acquiring human papillomavirus from the plume produced by the carbon dioxide laser in the treatment of warts. J Am Acad Dermatol 32(3):436–441
Acknowledgements
The authors would like to thank Eleri Staiger-Williams, biomedical librarian at UBC Woodward Library for her invaluable assistance with the search algorithm for this review.
Author information
Authors and Affiliations
Contributions
TW—conceptualization, methodology, data collection/analysis, manuscript original writing. CR-M—conceptualization, methodology, data collection/analysis, manuscript original writing.
Corresponding author
Ethics declarations
Disclosures
Drs. Ted Wu and Connal Robertson-More have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Robertson-More, C., Wu, T. A knowledge gap unmasked: viral transmission in surgical smoke: a systematic review. Surg Endosc 35, 2428–2439 (2021). https://doi.org/10.1007/s00464-020-08261-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-020-08261-5