
Abstract
Background and aims
Although colorectal endoscopic submucosal dissection (ESD) has become a standardized procedure worldwide, the difficulty of the procedure is well known. However, there have been no studies assessing the causes of treatment interruption. The present study aimed to evaluate the factors involved in the interruption of colorectal ESD.
Methods
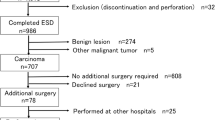
We retrospectively analyzed 1116 consecutive superficial colorectal neoplasms of 1012 patients who were treated with ESD between August 2008 and September 2018. The clinicopathological characteristics and treatment outcomes were analyzed.
Results
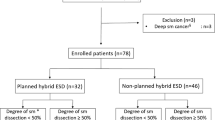
Interrupted ESD was reported in 14 lesions (1.3%) of the total study population. Univariate analysis of clinical characteristics indicated that age, 0–I macroscopic-type tumor, and tumor location on the left side colon were risk factors for interruption. Multivariate analysis revealed that 0–I macroscopic-type tumor was the sole preoperative independent risk factor for interruption. Univariate analysis revealed that the presence of muscle-retracting sign (MRS), deep submucosal tumor invasion, and intermediate invasive growth pattern represented the etiology of interruption. Multivariate analysis indicated that MRS can be a sole key sign for the interruption. Additionally, the resectability and curability of 0–I type tumors were significantly inferior to those of predominantly lateral spreading tumors. Observations of 0–I macroscopic-type tumors, MRS, and submucosal deep invasion were significantly more frequent in interrupted cases. Conventional endoscopic images without magnification endoscopy were more associated with interruption than irregular surfaces or Vi pit patterns in cases with 0–I type tumors.
Conclusion
ESD of 0–I type tumors is highly disruptive, and undiagnosable submucosal infiltration can reduce the curability.


Similar content being viewed by others

Abbreviations
- ESD:
-
Endoscopic submucosal dissection
- EMR:
-
Endoscopic mucosal resection
- EPMR:
-
Endoscopic piecemeal mucosal resection
- IRB:
-
Institutional Review Board
- JGES:
-
Japan Gastroenterological Endoscopy Society
- LST:
-
Laterally spreading tumor
- OR:
-
Odds ratio
- MRS:
-
Muscle-retracting sign
- pSM2:
-
Submucosal deep invasive cancer (≥ 1000 µm)
- INF:
-
Infiltration pattern
- CI:
-
Confidence interval
References
Tanaka S, Oka S, Kaneko I et al (2007) Endoscopic submucosal dissection for colorectal neoplasia: possibility of standardization. Gastrointest Endosc 66:100–107
Saito Y, Uraoka T, Yamaguchi Y et al (2010) A prospective, multicenter study of 1111 colorectal endoscopic submucosal dissections (with video). Gastrointest Endosc 72:1217–1225
Tanaka S, Oka S, Chayama K (2008) Colorectal endoscopic submucosal dissection: present status and future perspective, including its differentiation from endoscopic mucosal resection. J Gastroenterol 43:641–651
Tanaka S, Terasaki M, Kanao H et al (2012) Current status and future perspectives of endoscopic submucosal dissection for colorectal tumors. Dig Endosc 24:73–79
Toyonaga T, Man-i M, Fujita T et al (2010) Retrospective study of technical aspects and complications of endoscopic submucosal dissection for laterally spreading tumors of the colorectum. Endoscopy 42:714–722
Imai K, Hotta K, Ono H et al (2016) Preoperative indicators of failure of en bloc resection or perforation in colorectal endoscopic submucosal dissection: implications for lesion stratification by technical difficulties during stepwise training. Gastrointest Endosc 83:954–962
Kim ES, Cho KB, Park KS et al (2011) Factors predictive of perforation during endoscopic submucosal dissection for the treatment of colorectal tumors. Endoscopy 43:573–578
Iacopini F, Saito Y, Bella A et al (2017) Colorectal endoscopic submucosal dissection: predictors and neoplasm-related gradients of difficulty. Endosc Int Open 05(E839):E846
Toyonaga T, Tanaka S, Man-I M et al (2015) Clinical significance of the muscle-retracting sign during colorectal endoscopic submucosal dissection. Endosc Int Open 3:E246–E251
Bae JH, Yang DH, Byeon JS et al (2016) Clinical outcomes of endoscopic submucosal dissection for large colorectal neoplasms: a comparison of protruding and laterally spreading tumors. Surg Endosc 30:1619–1628
Tanaka S, Kashida H, Saito Y et al (2015) JGES guidelines for colorectal endoscopic submucosal dissection/endoscopic mucosal resection. Dig Endosc 4:417–434
Matsuda T, Fujii T, Saito Y et al (2008) Efficacy of the invasive/non-invasive pattern by magnifying chromoendoscopy to estimate the depth of invasion of early colorectal neoplasms. Am J Gastroenterol 103:2700–2706
Lambert R (2003) The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon: November 30 to December 1 2002. Gastrointest Endosc 58(6 Suppl):S3–S43
Kudo S, Lambert R, Allen JI et al (2008) Nonpolypoid neoplastic lesions of the colorectal mucosa. Gastrointest Endosc 68:S3–S47
Kobayashi R, Hirasawa K, Ikeda R et al (2017) The feasibility of colorectal endoscopic submucosal dissection for the treatment of residual or recurrent tumor localized in therapeutic scar tissue. Endosc Int Open 5:E1242–E1250
Kobayashi R, Hirasawa K, Sato C et al (2018) Utility of multi-detector computed tomography scans after colorectal endoscopic submucosal dissection: a prospective study. Gastrointest Endosc 87:818–826
Japanese Society for Cancer of the Colon and Rectum (2019) Japanese classification of colorectal carcinoma, 3rd edn. Kanehara & Co., Ltd., Tokyo
Schlemper RJ, Riddell RH, Kato Y et al (2000) The Vienna classification of gastrointestinal epithelial neoplasia. Gut 47:251–255
Matsuda T, Saito Y, Nakajima T et al (2011) Macroscopic estimation of submucosal invasion in the colon. Tech Gastrointes Endosc 13:24–32
Hirasawa K, Sato C, Makazu M et al (2015) Coagulation syndrome: delayed perforation after colorectal endoscopic treatments. World J Gastrointest Endosc 7:1055–1061
Liu HH, Kudo SE, Juch JP (2003) Pit pattern analysis by magnifying chromo endoscopy for the diagnosis of colorectal polyps. J Formos Med Assoc 102:178–182
Matsumoto A, Tanaka S, Oba S et al (2010) Outcome of endoscopic submucosal dissection for colorectal tumors accompanied by fibrosis. Scand J Gastoenterol 45:1329–1337
Takezawa T, Hayashi Y, Shinozaki S et al (2019) The pocket-creation method facilitates colonic endoscopic submucosal dissection (with video). Gastrointest Endoscop 89:1045–1053
Toyonaga T, Ohara Y, Baba S et al (2018) Peranal endoscopic myectomy (PAEM) for rectal lesions with severe fibrosis and exhibiting the muscle-retracting sign. Endoscopy 50:813–817
Rahni DO, Toyonaga T, Ohara Y et al (2017) First reported case of per anal endoscopic myectomy (PAEM): a novel endoscopic technique for resection of lesions with severe fibrosis in the rectum. Endosc Int Open 5:E146–E150
Shimura T, Ebi M, Yamada T et al (2014) Magnifying chromoendoscopy and endoscopic ultrasonography measure invasion depth of early stage colorectal cancer with equal accuracy on the basis of a prospective trial. Clin Gastroenterol Hepatol 12:662–668
Saitoh Y, Obara T, Einami K et al (1996) Efficacy of high-frequency ultrasound probes for the preoperative staging of invasion depth in flat and depressed colorectal tumors. Gastrointest Endosc 44:34–39
Stergiou N, Haji-Kermani N, Schneider C et al (2003) Staging of colonic neoplasms by colonoscopic miniprobe ultrasonography. Int J Colorectal Dis 18:445–449
Ritsuno H, Sakamoto N, Osada T et al (2014) Prospective clinical trial of traction device-assisted endoscopic submucosal dissection of large superficial colorectal tumors using the S–O clip. Surg Endosc 28:3143–3149
Yamamoto K, Hayashi S, Saiki H et al (2015) Endoscopic submucosal dissection for large superficial colorectal tumors using the ‘‘clip-flap method’’. Endoscopy 47:262–265
Yamasaki Y, Takeuchi Y, Uedo N et al (2016) Traction-assisted colonic endoscopic submucosal dissection using clip and line: a feasibility study. Endosc Int Open 4:E51–E55
Author information
Authors and Affiliations
Contributions
Conception and design (KH, TF); acquisition of data (KH, TF, CS, MM, HK, RI, AS, YO); analysis and interpretation of data (KH, TF, MT, SM); drafting of the article (KH); critical revision of the article (KH, SM); statistical analysis (MT, KH, TF); final approval of the article (KH, SM). All authors listed have contributed substantially to the design, data collection and analysis, and editing of the manuscript.
Corresponding author
Ethics declarations
Disclosures
Dr. Takehide Fukuchi, Kingo Hirasawa, Chiko Sato, Makomo Makazu, Hiroaki Kaneko, Ryosuke Kobayashi, Masafumi Nishio, Ryosuke Ikeda, Atsushi Sawada, Masataka Taguri, and Shin Maeda have no conflicts of interest or financial ties to disclose.
Ethical approval
The study and its protocols were approved by the ethical review boards of our hospital (Yokohama City University Certified Institutional Review Board; D1602024). All patients were informed of the risks and benefits of treatment before they underwent the procedure.
Informed consent
Informed consent or alternative versions were obtained from all patients included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Fukuchi, T., Hirasawa, K., Sato, C. et al. Factors influencing interruption of colorectal endoscopic submucosal dissection. Surg Endosc 35, 5497–5507 (2021). https://doi.org/10.1007/s00464-020-08042-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-020-08042-0